
Abstract
Abstract
Purpose:
Single port laparoscopic surgery (SPLS) is a technique which is increasing in popularity. The benefit of SPLS in complex Crohn's disease (CD), which includes a significant cohort of young patients sometimes needing multiple operations, has not been comprehensively assessed. This study analyses our early experience with this technique.
Methods:
Patients who underwent SPLS for CD were included. Data were collected prospectively from January 2013 to December 2015. Ileocolic resections, right hemicolectomy, small bowel stricturoplasties, and resections were included in the complex CD cohort. Primary and redo operations were analyzed separately.
Results:
Forty-five patients were included in the study (39 ileocolic resections and 6 small bowel stricturoplasty/resections). Of the total, 27 were primary resections and 18 were redo resections. The median age was 41 years (range 14–72 years), and the median hospital stay was 8 days (range 3–28 days). The total complication rate was 35.5% most of which were Clavien-Dindo type 1 and 2. There was no difference in operating time, average blood loss, conversion rates, complication rate, and hospital stay, between those who had primary or redo surgery.
Conclusions:
SPLS can be performed safely in patients with complex CD even in redo surgery. There may be some technical advantages to the procedure in this group of patients.
Introduction
C
Patients frequently present for surgery with associated systemic effects of chronic illness, such as anemia, malnutrition with hypoalbuminemia, and immunosuppression. Surgery in these patients can be technically challenging as a result of fragile tissue, inflamed and hypertrophic mesenteric fat, intercurrent abscesses, and in the case of redo surgery adhesions. There is also a higher risk of postoperative complications, such as poor wound healing and fistula formation.
The benefits of laparoscopy in patients with complex CD are well described4–6 and over the last 20 years it has become the preferred approach, compared to open surgery, in these patients. One of the main advantages of laparoscopic surgery is the reduction in wound morbidity and improved cosmesis resulting from fewer and smaller incisions. As a result of the complex presentations associated with CD the reported conversion rates range from 5% to 21%.7–9
Over the last few years more minimally invasive techniques, such as single port laparoscopic surgery (SPLS), have been described and increased in popularity. The single, small abdominal incision is thought to cause less tissue trauma, be relatively less painful, and have a better cosmetic result than the three to five incisions needed in standard laparoscopy.10–14
There is a further potential advantage that it may reduce the conversion rate as it allows “open” and laparoscopic access to the peritoneal cavity. 15 Many studies have shown the efficacy and the safety of this technique in colorectal surgery although the authors have noted some technical difficulties and a steep learning curve. It has also been shown that sufficient training in advanced laparoscopic skills can be transferrable and allows the surgeon to safely perform SPLS with minimal complications. 16 Complex CD adds a different level of complexity as the risk of conversion in the presence of abscess formation, redo surgery, and multiple strictures is higher.14,16 The true benefit of SPLS is most likely to be in this group of patients by reducing the need for conversion.
We aim to show that SPLS can be offered safely in this group of patients with complex CD reducing the need for laparotomy.
Materials and Methods
Data from patients who underwent SPLS for CD from January 2013 to December 2015 were prospectively collected and included in the study. Ileocolic resection, right hemicolectomy, small bowel stricturoplasties, and resections were included in the complex CD cohort. Fistulas/abscesses and multiple or long-segment disease has been classified as complex CD. Patients were subcategorized into two groups as follows: patients who had primary surgery and patients who underwent redo surgery for complex CD (Table 1). The operative time, overall conversion rate, total blood loss, and hospital stay were analyzed. Short-term postoperative morbidity was assessed using the Clavien-Dindo classification. 17 Outcomes at 12 months were also analyzed.
Previous surgery in other Institute.
CCD, complex Crohn's disease; EEF, enteroenteric fistula; ECF, enterocutaneous fistula; ICR, ileocolic resection; IAA, intra-abdominal abscess; MS, multiple (or long) segments disease; SBR, small bowel resection; SPLS, single port laparoscopic surgery; STP, stricturoplasty; VLS, video-laparoscopic surgery.
The procedures were performed by a single surgeon (J.H.W) using a GelPOINT Port (Applied Medical, Rancho Santa Margarita, CA) that was placed through a 3 to 4 cm midline periumbilical incision. The device consists of a disposable circular wound retractor which is applied to the abdominal wall and a gel cap through which the ports are inserted. Three working ports were placed in the gel cap with a 12 mm port placed in the center and two 10 mm ports placed laterally. A standard 30° laparoscopic camera (Karl Storz, Tuttlingen, Germany) was used. The camera was placed in any of the ports as required. This approach also had the advantage of allowing exteriorization of the bowel through the port site for extracorporeal procedures as required. The intracorporeal parts of the procedures were carried out in a similar manner to that described for conventional laparoscopic surgery. Ileocolic resections were performed by mobilizing from medial to lateral using the Harmonic Scalpel (Ethicon, US). The ileocolic vessels were dissected, clipped, and divided as the first step. The right colon and hepatic flexure were mobilized, and the colon and ileum were exteriorized through the periumbilical incision and a stapled side-to-side functional end-to-end anastomosis performed with a linear stapler. All surgeries were performed by a single surgeon who was trained in SPLS.
Results
Between January 2013 and December 2015, 45 patients with complex CD were included. Of the total, 39 had ileocolic resection and 6 had small bowel stricturoplasty or resection. Twenty-seven were primary operations and 18 were redo operations. The median age was 41 years (range 14–72 years). Male to female ratio was 19:26. Forty patients were ASA 2 and 5 were ASA 3.
In the primary surgery group (n = 27), the median operative time was 120 minutes (range 90–210 minutes). The average blood loss was 150 mL (range 0–750 mL). Complications as assessed by the Clavien-Dindo classification at 30 days were 1:6, 2:2, 3:0, and 4:1 (Table 2). The only patient with a Clavien-Dindo four complication was a 65-year-old male (ASA 3) with a flare of CD and subacute bowel obstruction, who was on long-term corticosteroid therapy. He required 3 days of Intensive Care and 10 days stay in the high dependency unit (HDU) due to respiratory failure. The median hospital stay was 6 days (range 3–28 days).
Noninfectious diarrhea probably due to inflammatory bowel disease.
SBO, small bowel obstruction.
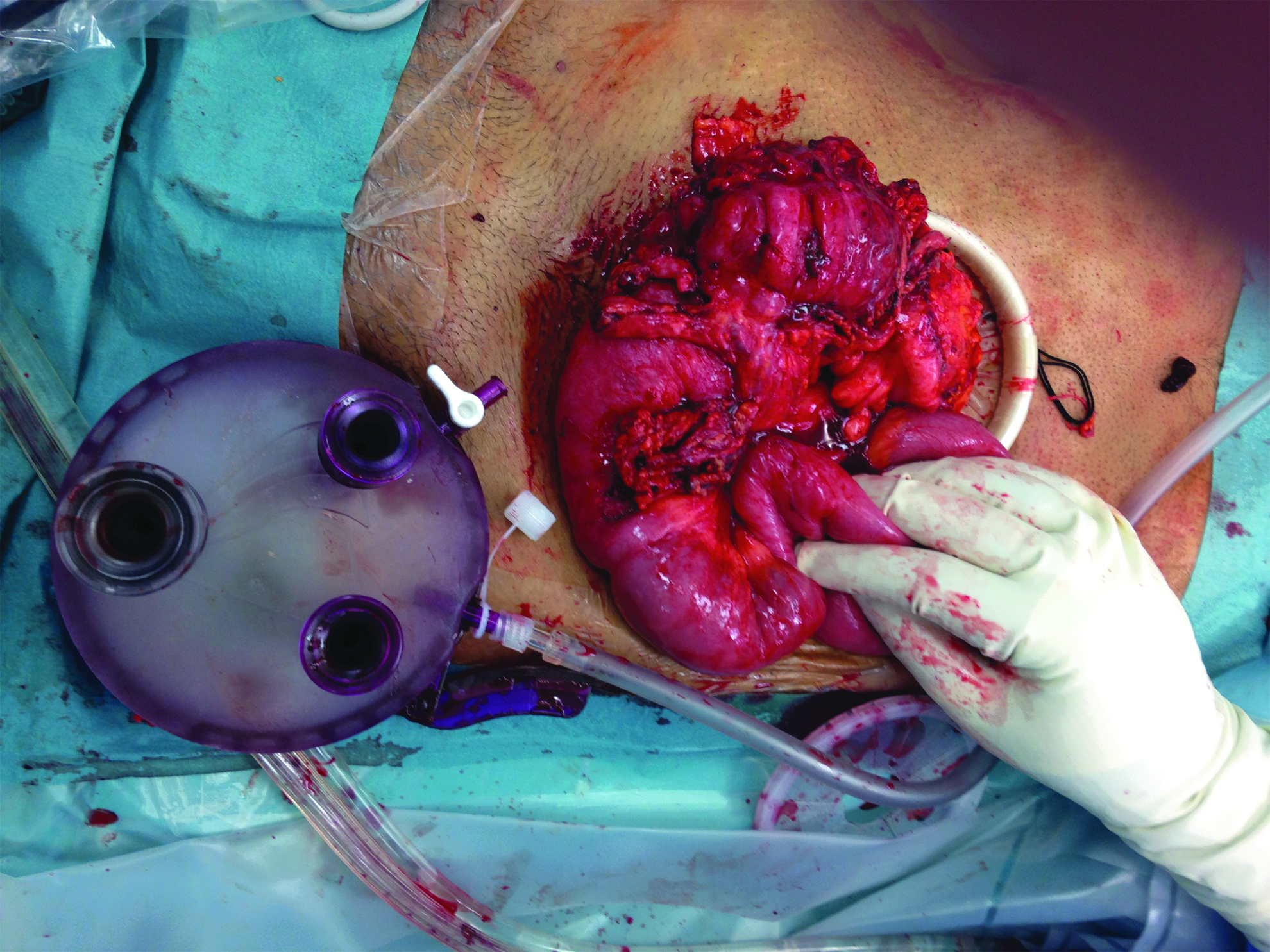
In the redo surgery group (n = 18), the median operative time was 130 minutes (range 90–220 minutes) and average blood loss was 180 mL (range 0–1200 mL). Two patients needed blood transfusion resulting from intraoperative blood loss. Both of them had low Hemoglobin before surgery. One patient required diversion with loop ileostomy due to preoperative intra-abdominal complications of CD; this patient presented initially with multiple intra-abdominal abscesses and multiple enterocutaneous and enteroenteric fistulas (Fig. 1). Complications as assessed by the Clavien-Dindo classification in this group at 30 days were 1:5, 2:1, 3:1, and 4:0 (Table 2). The median hospital stay was 7 days (range 5–14 days).

A patient required diversion with loop ileostomy. This patient presented initially with multiple intra-abdominal abscesses and multiple enterocutaneous and enteroenteric fistulas.
Three patients (11%) in the primary group and 2 patients (11%) in the secondary group required conversion to open surgery. In the primary surgery group 1 patient required conversion because of mesenteric bleeding and the other 2 for dense inflammatory adhesions. In the secondary surgery group both patients required conversion as a result of dense adhesions.
Comparing the results we observed that there was no significant difference between the primary surgery and redo surgery group with regard to operating time, average blood loss, conversion rates, complication rate, and hospital stay (Table 3). Four patients of the total cohort had follow-up less than 6 months. Forty-one patients had a follow-up at 1, 6, and 12 months.
There are no significant differences between the two groups (P > .05).
At 6 months there were no recorded long-standing complications. Minor complications at 1 month are recorded in Tables 1 and 2. There were no incisional hernias noted. Four patients had a keloid scarring. There were no anastomotic leaks and there were no deaths. Three patients were readmitted in the follow-up period. One patient was readmitted for an unrelated illness, and 2 patients had small bowel obstructions which settled with conservative treatment.
We did not find relevant complications at 12 months.
Discussion
In this series we have demonstrated that the single incision technique can be used safely in patients with complex CD with a lower conversion rate than what has been described in the literature for laparoscopic surgery in complex CD. Several articles from high volume inflammatory bowel disease centers have shown that the conversion rate for laparoscopic surgery ranges from 15% to 70%.18–21 These rates are particularly high especially when laparoscopic surgery is offered for complex cases. 21 The reduced conversion rate highlights the ability to switch between laparoscopy and open surgery at any stage of the operation without losing the advantages of laparoscopy. As a result we feel that this approach allows for easy visualization of the bowel if required especially where serosal tears may be present. The lack of any inadvertent injuries to the bowel in this series probably highlights the use of this approach. In standard laparoscopy once an extraction incision is made the advantages of laparoscopy are lost unless this incision is closed and reinsufflation is achieved. In this approach switching between the two techniques is easy and does not add to operative time (Figs. 2–4). Many case reports and series have shown feasibility and safety of the SPLS technique in CD. Kawahara et al. reported the first such case of a 36-year-old male who had a right hemicolectomy for recurrent CD: perioperative blood loss was 100 mL; operative time 130 minutes; and no complications were recorded. 22 Stewert et al., in 2011, published the first prospective database of 6 patients with complex CD (paracolic abscess, phlegmons, and fistulas) undergoing SPLS resections. Their results were comparable to standard laparoscopy. 23 Rijcken et al., in a larger cohort of patients, reported no statistical differences in postoperative pain scores, length of stay, and conversion rate between laparoscopic and SPLS groups. They also reported an operative time that was significantly lower in the SPLS group. 24

The SPLS (external global view). SPLS, single port laparoscopic surgery.
One of the main advantages of this technique is the ability to switch between laparoscopy and open surgery at any stage of the operation without losing the advantages of laparoscopy. In this case due to many adhesions the specimen is brought out for an open adhesiolysis.

Open adhesiolysis through the port. Once this is completed the surgeon can switch back to the laparoscopic approach completing the dissection safely.
More recent data, from Motfah et al., show that complex CD patients may benefit from SPLS in both elective and urgent operations. They present a prospective study of 33 patients with CD, 31 ileocolic resections and 2 sigmoid colectomies. No intraoperative or anastomotic complications were reported; however, 13 patients had complications (Clavien Dindo 1:8, 2:2, 3:3) reflecting the disease complexity. In their technique they describe the use of a “Surgical Glove Port” instead of a commercially available port, which has the added advantage of reducing costs. 25 This series also highlights the lower conversion rate, which has the added benefit for patients with CD who may require further surgery in the future.
The single incision technique can be used in both adults and children. The safety of SPLS has been also demonstrated in pediatric patients. Sharp et al. describe the first series of 28 patients (age range 11–18) all undergoing ileocecal resection for CD. Fifty-six percent of these patients were on steroid, 56% on anti-tumor necrosis factor (TNF) treatment, and 1 patient was on both therapies. They demonstrate a mean operative time of 86.5 minutes (range 56–166) with no conversions and no extra ports placed. They report four complications; one abscess, one wound infection, one small bowel obstruction, and one small bowel perforation. 26 Tam et al. also published a retrospective review of 19 children (age range 3–15) comparing SPLS with conventional laparoscopy and revealed no significant differences between the two groups. 27
The benefits of laparoscopic surgery over open surgery include improved cosmetic early return of bowel function, shorter postoperative stay, and reduced complications.4–6 The disadvantages of standard laparoscopic surgery compared to SPLS include multiple port sites and an additional or lengthened incision to remove the specimen leading to relatively worse cosmesis and increased pain. Also a higher number of port sites increase the risk of port site complications such as wound infections and incisional hernias. SPLS has all the advantages of standard multiport laparoscopy with the added benefit of improved cosmetic and pain outcomes. This technique also allows for easy delivery of the bowel through the incision for anastomosis and could prevent conversion to open surgery and a longer wound. Narouz et al. showed in a recent video the feasibility of this technique in difficult abdominal surgery. 16
The drawbacks of SPLS include the loss of the triangulation used in conventional multiport laparoscopy, the ergonomically unfavorable positions of the surgeon, the increased cost of new equipment in each procedure, and lack of training leading to increased operative time. We demonstrate that a well-trained laparoscopic surgeon can use SPLS safely in the context of complex CD patients with comparable operative times. The use of conventional laparoscopic instruments helps to reduce the cost. 28
We demonstrate that SPLS in complex CD patients is a feasible technique with a low conversion rate. The benefits of this are borne out mostly in those patients with complex CD as these patients are also at higher risk for further surgery than patients undergoing surgery for primary CD. Some criticisms of the single port approach have been the increased risk of incisional hernias described in early series of the technique. In this series we did not find any patients with incisional hernia on clinical examination up to 12 months follow-up and this may be as a result of the improved retraction systems associated with the newer single port devices. The main advantage is the ability to switch easily from laparoscopic to open surgery. Both primary patients and redo patients may have a benefit from SPLS and we have not seen any significant difference in operative time and complications. This technique has the potential to be the minimally invasive procedure of choice for patients with complex CD as it can combine the advantages of laparoscopic and open surgery with lower conversion rates and probably better cosmesis and acceptable complications in a cohort of patients who are young and have an increased risk of reoperation.
Footnotes
Disclosure Statement
No competing financial interests exist.