
Abstract
Abstract
Introduction:
Although laparoscopic liver resection (LLR) has developed rapidly, its usefulness for the treatment of large tumors is less clear, due to concerns about compromising oncological principles and patient safety. The purpose of this study was to explore the feasibility and safety of LLR for the treatment of hepatocellular carcinoma (HCC) with a tumor size larger than 5 cm.
Patients and Methods:
From January 2007 to December 2014, we performed LLR in 45 patients with HCC with a tumor size ≥5 cm. Perioperative outcome, tumor recurrence, and overall patient survival were analyzed.
Results:
Median age was 60 years (interquartile range [IQR] 52–68) and 64.4% (29/45) were male. Seven patients (15.6%) had larger than 10 cm of HCC. No operative deaths occurred and six of the laparoscopic procedures were converted to open resection (conversion rate 13.3%). Median operation time was 365 minutes (IQR 277–443) and median estimated blood loss (EBL) was 400.0 mL (IQR 275–600). There was no R1 or R2 resection and median resection margin was 19.0 mm (IQR 8.0–33.0). Complications above Clavien-Dindo classification grade III occurred in four patients (8.9%). The median overall follow-up time was 10.7 month (range 1.1–62.1). One-year recurrence free survival (RFS) and overall survival (OS) were 86.0% and 95.5%, and 3-year RFS and OS were 70.7% and 86.0%.
Conclusion:
LLR appears safe and feasible in patients with HCC with a tumor size larger than 5 cm. Expansion of indication for LLR in patients with HCC may be considered.
Introduction
H
Materials and Methods
Study population
We performed retrospective data collection of 377 consecutive patients who underwent LLR for HCC at Samsung Medical Center, South Korea, from January 2006 to September 2014. After excluding patients who were less than 5 cm of tumor size, 45 cases were suitable for analysis. The decision to undertake surgical resection was based on expert opinion delivered at a multidisciplinary meeting. Selection criteria for LLR were determined by the surgeon on the basis of tumor size and location, assessed by computed tomography (CT) and/or magnetic resonance imaging (MRI), and the perioperative risk evaluation was done using the American Society of Anesthesiologists (ASA) score. Patients presenting with an ASA score 4 were deemed to be unsuitable for surgical resection, including by laparoscopy.
Surgical procedures
All liver resections were intended to be totally laparoscopic and were performed according to the procedures described and the surgeon's usual practice. The patient was placed in a supine position with the legs apart, except in posterior liver (segments 6 and 7) resections, in which left lateral decubitus positioning with an elevated right arm was chosen. Pneumoperitoneum was created by carbon dioxide insufflation at a pressure of 11–12 mmHg, and a 0-degree flexible laparoscope camera was used. Parenchymal transection was performed with an ultrasonic dissector, advanced bipolar device, and/or cavitron ultrasonic surgical aspirator (CUSA. EXcel, Valleylab, Boulder, CO) in accordance with the surgeon's usual practice. The corresponding Glissonean branch was managed using temporary inflow control of the Glisson (TICGL) method and anterior approach was used whenever possible. Temporary increase of intra-abdominal pressure was up to 15 mmHg to balance the CVP. Small vessels were controlled with bipolar coagulation and larger vessels were clipped or electively stapled. The pedicle clamping was not used routinely but only when there was bleeding or when a long operation time was anticipated. The specimen was usually extracted through a Pfannenstiel incision but when there was a previous laparotomy scar, the previous incision was used.
Evaluation criteria
Intraoperative variables include operation duration, transfusion rate, need for and duration of pedicle clamping, and incidence of conversion to laparotomy. Postoperative parameters include pathological margins, postoperative complications above Clavian–Dindo classification grade III, 30- and 90-day mortality, and duration of hospital stay. Long-term survival and recurrence rates were estimated at 1 and 3 years. Data on clinicopathological factors, such as age, sex, ASA grade, preoperative hepatic function, underlying liver disease and its cause, number and size of tumors, vascular invasion, presence of satellite nodules, and pathological margins, were collected.
Statistical analysis
Clinical data were expressed as the median (interquartile range, [IQR]) or frequency as appropriate. Overall survival (OS) and recurrence-free survival (RFS) were computed from the date of operation. Survival curves were estimated using the Kaplan–Meier method. All statistical analyses were carried out using IBM SPSS statistics version 22.
Results
Patient characteristics
The clinical characteristics of the 45 patients with HCC are given in Table 1. Preoperative underlying liver disease was predominantly related to hepatitis B virus (HBV) infection in 73.3% (33/45). ASA class less than II were 91.9% (41/45) and 4 (8.9%) patients were class III. All patients were Child A but 17.8% patients had background liver cirrhosis with a median ICG R15 of 9.55%. Pretreatment was done in 12 patients. Among these patients, one received transarterail chemoembolization (TACE) twice and radiofrequency ablation (RFA) once and one received 20 times TACE, 2 times RFA, and 40 Gy radiation therapy (RT) due to uncontrolled HCC following TACE.
One patient had TACE and RFA, and another patient had TACE, RFA, and radiation therapy.
BMI, body mass index; aFP, alpha-fetoprotein; PT, prothrombin time; ICG, indocyanine green; ASA, American society of anesthesiologists; HBV, hepatitis B virus; HCV, hepatitis C virus; HCC, hepatocellular carcinoma; TACE, transarterial chemoembolization; RFA, radiofrequency ablation; PVE, portal vein embolization; IQR, interquartile range.
Surgical procedures
Types of resection and intraoperative data are given in Table 2. More than a half of patients (57.9%, 26/45) had liver resection more than 3 segments; 7 (15.6%) left hemihepatectomy; 16 (35.6%) right hemihepatectomy; and 3 (6.7%) extended right hemihepatectomy. We had to convert to laparotomy in 13.3% (6/45) of patients, the main cause being bleeding (5/6). A minilaparotomy was used for bleeding control in four patients, and conventional J incision was used in one patient. One patient was converted to open due to severe adhesion with the stomach. Median blood loss was 400.0 mL and intraoperative transfusion was done in eight (17.8%) patients. Among these eight patients, four were converted to laparotomy for bleeding control. Median operation time was 365 minutes.
Postoperative outcomes
Median hospital stay was 9 days and overall major morbidity (Clavien grades of III and IV) rate was 8.9% (4/45) (Table 3). One patient with HCC of 14cm developed controlled bile leak and died of air embolism after self-removal of internal jugular vein catheter 28 days after operation. One patient treated for 11cm HCC developed transient postoperative liver failure and was discharged with high bilirubin level (27.7 mg/dL) at POD 43. A patient experienced pretreatment with 20 times TACE, 2 times RFA, and 40 Gy RT, found duodenal fistula after operation, and healed after conservative therapy during 93 hospital days. One patient needed wound repair on general anesthesia. The median overall follow-up time was 10.7 month (range 1.1–62.1). One-year RFS and OS were 86.0% and 95.5%, and 3-year RFS and OS were 70.7% and 86.0% (Fig. 1).
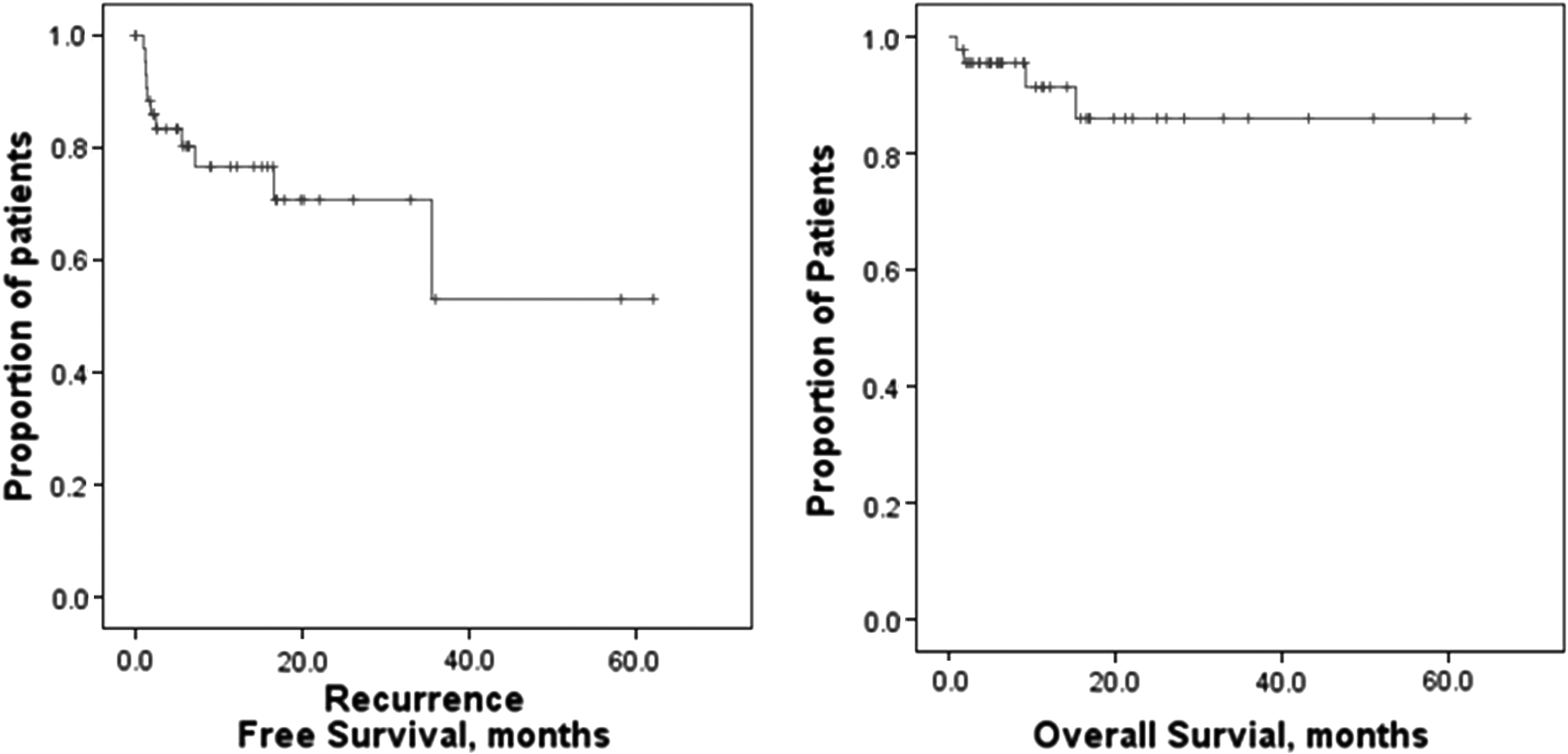
Recurrence-free survival and overall survival in 45 patients submitted to laparoscopic liver resection for hepatocellular carcinoma with larger than 5 cm.
Pathological features are given in Table 4. Median tumor size was 6.50 cm and 7 patients had larger than 10 cm of HCC. Thirteen (28.9%) patients had multiple tumor or satellite nodules. Eight patients had HCC with hepatic cirrhosis. All patients had R0 resection and median resection margin was 19.0 mm (IQR 8.0–33.0). Between tumor size 5–10 cm and larger than 10 cm, there was no statistically significant differences in postoperative outcomes (Data not shown).
Discussion
LLR has been widely and rapidly accepted in the field of hepatobiliary surgery because laparoscopic surgery is associated with a reduced need for narcotic pain relief, shorter hospital stay, earlier return to work, and less physiological stress than the open abdominal surgery. 6 The appeal of LLR is easy to appreciate, but it is a technically challenging procedure as expertise in both laparoscopy and open liver surgery are essential. Many studies suggested that it was preferable to use LLR only for tumors measuring ≤5 cm in diameter5–7,10 but the use laparoscopic approach in tumors larger than 5 cm is still controversial. Widespread use of laparoscopic hepatectomy for the large HCC has been hindered by fears of major hemorrhage and the technical challenges of portal, caval, and hepatic vein dissection. Technical advances have allowed LLR to be performed safely, but equivalent recurrence and survival rates must also be verified before LLR can be considered a suitable alternative to OLR. The first hepatectomies for the large HCC were reported by Huscher et al. 11 Recently, Dagher et al. 12 reported a prospective study of 210 laparoscopic major liver resections. Their results showed that a purely laparoscopic approach was used in 43.3% of cases, and conversion to laparotomy was required in 12.4% of cases. The mortality rate was 1% and the specific morbidity rate (hemorrhage, ascites, or biloma) was 8.1%. In patients with malignant disease, negative margins (R0 resections) were achieved in 97.4%.13,14 We successfully performed LLR for HCC larger than 5 cm for the first time in 2007. Since then, we have not restricted the application of LLR to HCC according to tumor size. This study showed favorable perioperative outcomes, postoperative morbidity, and survival rate when compared with those of previous reports that focused on LLR for tumor size less than 5 cm.15–22 Open conversion was only necessary in 13%, with 8.9% postoperative major complication. The 3-year RFS and OS rates were 70.7% and 86.0%, respectively. In addition, it was demonstrated that patients with HCC larger than 5 cm have a similar outcome compared with that of patients with HCC less than 5 cm. Our study had longer operative time because more than 50% of LLR was major hepatectomy. Although this longer operative time along with a tendency toward slightly higher rate of open conversion, these differences in early clinical outcome did not affect postoperative morbidity or oncologic results.
The main fear in laparoscopic approach in large tumors is the possibility of HCC dissemination due to tumor rupture because of lack of mobility. However, we have not observed any case of tumor dissemination in our study. Although laparoscopic approach has much restriction of motion compared to open, because of its flexibility to approach in areas that cannot easily be reached by open method without retracting the tumor such as around the caudate lobe or the caval ligament, it may be even advantageous to perform large tumors using laparoscopic approach. Nevertheless, our result is not concrete enough to draw a conclusion and this hypothesis needs further investigation. The main advantage of laparoscopic approach is the reduction of surgical trauma related with large incision. But this advantage is much reduced in large tumors since a relatively large incision is still necessary to extract the specimen. In our study about tumors larger than 10 cm, we have no case of open conversion but one patient submitted extended right hemihepatectomy with 14 cm of HCC and had controlled bile leak and one submitted right hemihepatectomy with 11 cm of HCC and suspected liver failure. According to our experience, because the shape of the right liver is round like a ball unlike the left which is long and slim, large tumors located on the right side usually need larger incisions compared to similar size tumor of the left side and the advantage of laparoscopic approach is reduced. So although laparoscopic approach may be feasible even in tumors larger than 10 cm, we recommend using laparoscopic approach more judiciously for large tumors located on the right side.
Although the conclusions drawn by our results is limited because of the small sample size and the limitations of the study design, we think that laparoscopic approach for HCC with a tumor size larger than 5 cm is safe and feasible in selected cases under experienced hand and it should not be regarded as a contraindication. We look forward for more data to come concerning this group of patients to draw a final conclusion.
Conclusion
LLR appears safe and feasible in patients with HCC with a tumor size larger than 5 cm in appropriately selected patients. Expansion of indication for LLR in patients with HCC may be considered.
Footnotes
Disclosure Statement
No competing financial interests exist.