
Abstract
Abstract
Purpose:
The aim of this retrospective study is to demonstrate the safety and feasibility of the laparoscopic technique for treatment of massive incisional hernias (MIHs) and to compare three different fixation devices.
Methods:
From January 1, 2001, to December 31, 2014, we collected retrospective data from patients with large incisional hernias (IHs). Laparoscopic IH repair is performed by applying a three-dimensional polyester knit structure mesh with a resorbable collagen barrier on peritoneal side (Parietex™ Composite Mesh; Covidien, New Haven, CT). Patients were divided into three groups according to the different fixation devices. The mean follow-up was 19 (12–156) months.
Results:
The mean defect size was 12.83 cm (10–26 cm) and the mean body mass index was 30.8 kg/m2 (26–39 kg/m2). The EMS stapler™ was used on 260 patients, the Protack® on 210 patients, and the AbsorbaTack™ on 30 patients. The mean operative time was 69.9 minutes (38–130 minutes). Intraoperative morbidity rate was 1.6% (8 cases). Early reoperation rate was 0.2% (1 case). The mean length of hospital stay was 2.3 days (range 2–7 days). Seromas were observed in 20 patients (4.0%) and neuralgia in 10 patients (2.0%). Recurrence was observed in 12 patients (2.4%) with the majority in the absorbable tack group (10%). There were no conversions (0%) to open technique.
Conclusions:
The laparoscopic approach seems to be safe and appropriate for treatment of MIH. The Parietex composite mesh we used guarantees excellent intraabdominal laparoscopic repair of abdominal wall defects. Absorbatack system seems to give less postoperative neuralgia, but it is related to a high recurrence rate. Protack system seems to give more postoperative neuralgia than the Endopath EMS. In our experience, the best fixation system is the latter.
Introduction
I
Materials and Methods
From January 1, 2001 to December 31, 2014, we collected retrospective data from patients with large IHs (W3 according to EHS classification) who underwent laparoscopic surgical repair at the same institution. The decision to operate was made for one or more of the following reasons:
• Episodes of ileus or subileus • Low quality of life caused by parietal defect
We considered the following inclusion criteria:
• 10 cm as the minimum size of the IH • Presence of “Swiss cheese abdominal wall”
We considered the following exclusion criteria:
• Presence of other abdominal diseases • Pregnancy • Less than 18 years of age • Adhesions that contraindicate laparoscopy • Ongoing infection • Anesthesiology contraindications
Laparoscopic IH repair is performed by applying a three-dimensional polyester knit structure mesh with a resorbable collagen barrier on one side to limit visceral attachments on the peritoneal layer of the abdominal wall (Parietex™ Composite [PCO] Mesh; Covidien, New Haven, CT). Patients were divided into three groups according to the different fixation devices: Endopath® EMS (Ethicon US, West Somerville, NJ), Protack® (Covidien, New Haven, CT), and AbsorbaTack™ (Covidien, New Haven, CT). The Endopath EMS Endoscopic Multifeed Stapler is a sterile single-patient-use instrument designed to be used with the 10/11-mm diameter ENDOPATH Surgical Trocar. The device places rectangular titanium staples. Closed staple dimensions are ∼5.3 × 3.7 mm. The Protack system is a 5 mm mechanical fixation device. It is a sterile, single-patient-use instrument and utilizes titanium coils that are screwed into the tissues through the prosthesis. The AbsorbaTack system is a 5 mm sterile single-use device for fixation of prosthetic material. Tacks are in absorbable synthetic polyester copolymer derived from lactic and glycolic acid. The mean follow-up was 19 (12–156) months.
Surgical technique
The day before surgery, the patient is prepared with polyethylene glycol (PEG) solutions to empty the bowel and simethicone to reduce intestinal gas content. Under general anesthesia, the patient is placed in the supine position. Nasogastric tube and urinary catheter are placed during the procedure and removed once surgery is completed. Antibiotic prophylaxis with third-generation cephalosporin is used. The procedure starts by establishing pneumoperitoneum with the Veress needle technique. We test the abdominal wall with physiological saline and spinal needle to check for the absence of any adhesions in the area where the first trocar is inserted. We also recommend the use of an optical trocar where possible. The number of trocars and their insertion are crucial and related to the location and size of the hernia. After insertion of an optical trocar at 30°, it is possible to proceed with the exploration of the abdomen and the insertion of other trocars. The most frequent area for introduction of the first trocar is the left or right hypochondrium in the subcostal area. We normally use three trocars. If length is greater than width, trocars are placed on the side that will guarantee a wider working space. If the transverse diameter is >15 cm and the lateral trocar insertion is not feasible, the patient is placed with open legs and trocars are placed in suprapubic area, for the optics, (10 mm) and right (12 mm) and left (5 mm) iliac fossa. In all cases, trocars are placed to have good exposure and triangulation. Intraabdominal adhesiolysis is safely performed with blunt dissection and ultrasound dissectors. In case of bowel entrapment with partial obstruction, we perform a small incision of the hernia's ring freeing the bowel. We do not perform reduction or treatment of the IH sac. The herniary defect is drawn on the patient's abdominal wall to be able to select the prosthesis with the most suitable dimensions (the prosthesis must protrude over the defect edges by at least 4–5 cm). It is not necessary for the mesh to overlap the whole scar if no other defects can be identified. When the peritoneal side of the abdominal wall is completely freed (Fig. 1), the Parietex mesh is introduced through the 12-mm trocar. The smooth surface of the mesh must be oriented to the bowel and omentum. The prosthesis is then suspended and temporarily fixed to the abdominal wall with four to six transcutaneous straight needles. In this way, it is possible to obtain perfect centering of the prosthesis over the hernia defect, and it is easier to position the staples without the prosthesis when moving around inside the abdominal cavity. This is particularly true if the prosthesis is large. Pneumoperitoneum is reduced to 8 mmHg and two lines of tacks or staples are placed, regardless of which fixation device is used, creating a double-circle configuration with the outer line located 1 cm from the edge to prevent the mesh from folding on itself. After hemostasis is ensured, final inspection of the mesh (Fig. 2), bowel, and abdominal cavity is made. The trocars are then removed under direct observation and pneumoperitoneum is released. No drainage is usually placed and a compressive bandage is advocated for 7 days after surgery.
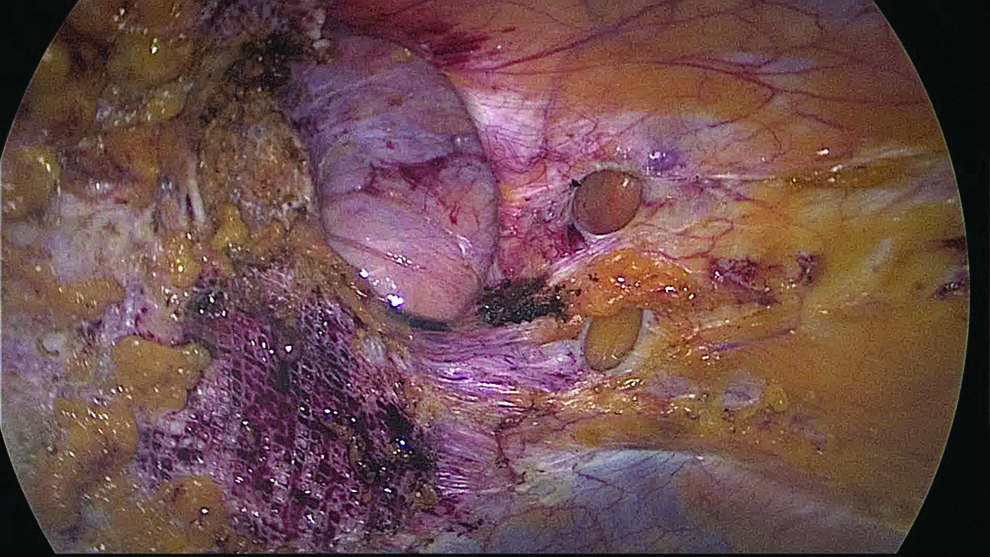
Swiss cheese abdominal wall.

Parietex mesh in situ.
Results
During the study period, 500 patients (mean age 56.6 years; range 42–73 years) with W3 IHs underwent laparoscopic IHR with synthetic double-layer mesh. The median follow-up was 19 months (range 12–156 months). The mean defect size was 12.83 cm (range 10–26 cm) and the mean body mass index was 30.8 kg/m2 (range 26–39 kg/m2; Table 1). The described laparoscopic technique was performed on 100% of patients. The Endopath EMS Endoscopic Multifeed Stapler was used on 260 patients, the Protack system was used on 210 patients and the AbsorbaTack system was used on 30 patients. Mesh size was 37 × 28 cm in 15 patients, 35 × 25 cm in 162 patients, 30 × 20 cm in 212 patients, and 25 × 20 cm in 107 patients. In 4 patients, the authors placed two 30 × 20 cm meshes. The mean operative time was 69.9 minutes (range 38–130 minutes). Intraoperative morbidities rate occurred was 1.6% (8 cases). They were characterized as bowel injuries occurring during surgery and sutured laparoscopically. There was 1 case (0.2%) of early reoperation for an unrecognized hollow viscus injury. It was treated laparoscopically with abdominal toilette, suture, and drainage: Parietex was not removed and no mesh or abdominal infections was observed. The mean length of hospital stay was 2.3 days (range 2–7 days). No surgical site infections were reported (0%) and mortality rate was 0.2% (1 case) caused by intestinal ischemia. During follow-up, seromas were observed in 20 patients (4.0%) and neuralgia in 10 patients (2.0%). Eight out of the 10 cases of neuralgia were observed in the Protack group, and in 3 of these cases, the authors removed the tacks because of drug-resistant pain. Recurrence rate was 2.4% (12 patients) with the majority observed in the absorbable tack group (10%). There were no conversions (0%) to open technique. Complications were registered during the first 12 months after surgery (Table 2).
Discussion
IH repair is one of the most performed surgeries in Western countries. It is estimated that 800,000 hernia repairs are performed in the United States and Europe every year.3,4 Low quality of life and subileus are the most important problems related to this entity. Laparoscopic IHR, first described by LeBlanc and Booth in 1993, 6 showed the same results regarding morbidity and mortality rates compared with open approach with better results concerning surgical site infections. 8 Even though these results are proven for IHs of all sizes, there is still debate regarding the best treatment choice for MIH. MIH is defined as herniation of the abdominal viscera through a wall defect of at least 10 cm in diameter (W3 according to EHS classification) or through a series of wall defects in which the minimum distance between the upper pole of the upper defect and the lower pole of the lower defect is at least 10 cm (Swiss cheese abdominal wall). MIH shows characteristic symptoms: respiratory distress, loss of domain for the herniated visceral mass, and rarefaction of the skin overlying the defect with risk of evisceration. Wormer et al., 9 in a prospective study in 2013, used similar dimensional criteria to define MIH. They showed a greater incidence of pain and activity limitation at 1 month of follow-up for patients undergoing laparoscopic or open MHR with large defect in widths (>10 cm) and total area (>100 cm2). Open treatment seems to be associated with increased early and chronic discomfort only in large defect in lengths. Ross et al., 10 in a prospective multicenter study in 2015, demonstrated that laparoscopic treatment of MIH shows better results than open surgery regarding postoperative pain and activity limitation at 1 month. In a recent review in 2015, Al Chalabi et al. 8 analyzed five randomized controlled trials regarding the comparison between laparoscopic and open IHR. A total of 611 patients were randomized: 306 patients to the laparoscopic group and 305 patients to the open repair group. They showed a higher wound infection rate in the open repair group (P < .001) although morbidity and mortality rates were similar. In other less recent works, the rate of wound complications after open surgery for IH was 27%.11–13 This single-center study analyzes retrospectively 500 cases of IH W3 (according to the EHS classification) treated with the laparoscopic technique. Our standard surgical technique provided mesh temporary fixing with four to six stitches at the abdominal wall. Above all, this technique is useful and safe when a large mesh (>500 cm2) is used as it allows the perfect Parietex calibration into the abdominal cavity. The characteristics of an ideal mesh should include adhesions prevention on one side and excellent fibrous ingrowth on the other side; for this reason manufacturers designed a two-layer mesh prosthesis. PCO (Covidien) is a three-dimensional multifilament polyester mesh bonded to a continuous, smooth hydrophilic, and absorbable collagen film that overlaps the cut edge of polyester by 5 mm. This mesh was designed to preserve brisk parietal tissue ingrowth while preventing adhesions on the visceral surface of the mesh. 14 It was designed with different materials for each layer: one layer to minimize or prevent adhesions to the visceral surface and one layer to maximize fibrous ingrowth on the parietal surface. Each layer is designed to meet the ideal characteristic of either the parietal or visceral surface. The adhesive qualities of prosthetic mesh in the intraperitoneal space are reduced with the use of a protected mesh as Parietex compared with the use of other types of mesh. McGinty et al., 15 in a 2005 comparative study, demonstrated that the number of PCO implants with adhesions was lower, and when adhesions were present, there was a significantly smaller area of mesh involved than expanded polytetrafluoroethylene (ePTFE) and polypropylene mesh (PPM). The use of PCO results in fewer and less severe visceral adhesions while providing adequate fibrous ingrowth of parietal tissue into the interstices of the mesh compared with ePTFE and PPM. In our opinion and according to the literature, PCO is able to combine tissue regrowth and prevent adhesions. The PCO mesh we used has the features required for excellent intraabdominal repair of abdominal wall defects. The softness of this prosthesis allows the surgeon to introduce it with extreme ease using a 12-mm trocar—even in the 30 × 20 cm format—thereby avoiding possible contaminations and infections (0.5%–6%), as described in the literature for other types of prosthesis whose thickness impedes their direct introduction through the trocar.16–20 The mean operative time (69.9 minutes, range 30–130) was not influenced by different fixation devices: EMS = 71.6 (38–130) minutes; Protack = 68.5 (40–120) minutes; Absorbatack = 65 (30–110) minutes. Longer operative times were observed in very large IHs with severe adhesions. Eight cases (1.6%) were complicated by bowel injuries occurred during viscerolysis and were treated with laparoscopic suture of the intestinal injury. The overall mortality rate was 0.2%, because of intestinal ischemia, and it did not seem to be related to different fixation devices. The overall postoperative morbidity rate was 7.6%. We have found a higher rate of postoperative neuralgia in the Protack group 3.8% (8 patients). Three of these patients required the removal of the tacks for drugs-resistant pain. The seromas rate at 6 weeks was 4.0% and it did not seem to be related to different fixation devices. Higher rate of recurrence was observed in the Absorbatack group (10.0%) than in the nonabsorbable fixation devices (EMS and Protack), for this reason we limited the number of patients treated with the absorbable tack. There was no difference in terms of recurrence rate (1.5% versus 2.3%), length of hospital stay (2.3 days versus 2.9 days), and seromas rate at 6 weeks (3.4% versus 4.7%) between EMS and Protack. No conversions to open technique and no wound infections were described.
Conclusions
Despite several limitations, this single-center study is one of the biggest series in the literature analyzing retrospectively 500 cases of IH W3 treated with the laparoscopic technique. The laparoscopic approach seems to be safe and feasible for the treatment of MIH. The PCO mesh we used has the features required for excellent intraabdominal laparoscopic repair of abdominal wall defects. Our temporary anchorage of Parietex Mesh to the abdominal wall is safe and allows perfect centering of the prosthesis over the hernia defect. Regarding the fixation devices, the Absorbatack system seems to be less related to postoperative neuralgia, but is related to a higher rate of recurrence than nonabsorbable systems. Concerning the nonabsorbable systems, the Protack system seems to give more postoperative neuralgia and necessity of tack removal than the Endopath EMS fixation system. In our experience, the best fixation system is the latter. Further studies are needed to confirm these pieces of evidence.
Footnotes
Disclosure Statement
No competing financial interests exist.