
Abstract
Abstract
The robotic surgical technology introduced over the last decade and a half has revolutionized many aspects of performing complex procedures. It combines technological and clinical innovations to improve surgical quality and patient outcomes. Yet, to date, there is still a lack of standardization in training and certification of robotic surgeons. The criteria for proficiency and credentialing in robotic surgery vary widely among institutions. The aim of this review is to discuss the key points of training and surgeon assessment in robotic surgery, as well as the challenges that still need to be overcome.
Introduction
T
Despite the wide-spread adoption of robotic surgical technology, the education, training, assessment, and certification for robotic surgery have not been rigorously pursued. To date, there are no established standardized training programs for robotic surgery. 1 As a part of the approval process for the device, the Food and Drug Administration (FDA), requires companies that manufacture the robotic systems to develop technical instructional training.
The Intuitive Surgical, Inc. maintains an online community for training, marketing and peer-to-peer communication. Further, they provide online training modules, detailed step-by-step procedure descriptions for specific surgical operations, and full-length videos. Those step-by-step procedure descriptions are developed with, reviewed, and approved by independent surgeons. As helpful as that material may be, there is a key limitation: da Vinci Surgical System training programs are not a replacement for hospital policy regarding surgical credentialing and privileges.
Education and Training Assessment
Surgical quality improvement is an important mission of several governmental and national professional organizations. Among their goals are the mitigation of surgical morbidity and reduction in healthcare costs. Surgical educators are being tasked with developing innovative curricula for trainees and certification programs for practicing surgeons, while maintaining restrictions in duty hours.
Introduction of robotic technology into surgical practice has resulted in a rapidly expanding technical complexity. Some surgeons, self-described as “early adaptors,” are quickly jumping on the bandwagon to embrace this new technology. They are driven by a general desire to advance the field and push the envelope but, as long as there is no standardized credentialing, it is hard to gauge who among these early adaptors is really able to perform the new procedures safely. It is the responsibility of the surgical community to assure that its members, while adopting new methods and techniques, adhere to the best practice guidelines and ethical standards.
Curricula
Currently there are four main robotic curricula in various stages of development: (1) Fundamentals of Robotic Surgery (FRS), (2) Fundamental skills of Robotic Surgery (FSRS), (3) Proficiency-based robotic curriculum, and (4) European Robotic Urology Section (ERUS) curriculum. After reviewing them, Fisher et al. conclude that FRS and the ERUS have the strongest offerings to become the gold standard for robotic surgery. 2
The FRS, based on the consensus of expert members of 14 international societies is being created to validate basic skill training for the use of robotic assisted surgery. 3 The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), which is responsible for the development and wide acceptance of Fundamentals of Laparoscopic Surgery (FLS), participated in this initiative. The FLS was used as the prototype for the development of the FRS. The skills training and assessment can be performed with a box trainer using the da Vinci robot or virtual reality simulators.
The Robotic Urology Section (ERUS) of the European Association of Urology (EAU) developed a curriculum that includes four modules: (1) e-learning, (2) simulation training with dry lab, virtual reality and wet lab, (3) operation room training under supervision, and (4) videoed full procedure and trainer's report, which will be used for certification. The wider range of training modalities compared to the FRS allows skills to be more transferable to the operating room (OR). 4
Task analysis
A series of consensus conferences have convened to compile the outcome measures to form the basis for a FRS program. In 2012, Dulan et al. 1 identified the cognitive and procedural skills needed for robotic surgery using a list of 23 tasks. The same year, this list was discussed at the SLS (Society of Laparoendoscopic Surgery) consensus meeting in Boston, resulting in the definition of 25 specific outcome measures, categorized into preoperative, intraoperative, and postoperative tasks (Table 1). These tasks can now become the accepted standard for training and certification. 5
OR, operating room.
Learning curve
The concept of a learning curve (LC) was first described in aircraft manufacturing, where the amount of man-hours required to produce a single unit decreased at a uniform rate as the production quantity was doubled. 6 In other words, performance improves with time and experience, with rapid improvement seen during the early stages of learning. The LC is often used to illustrate this phenomenon and can be described as having three components: the starting point, the slope of the curve, and the plateau (Fig. 1).
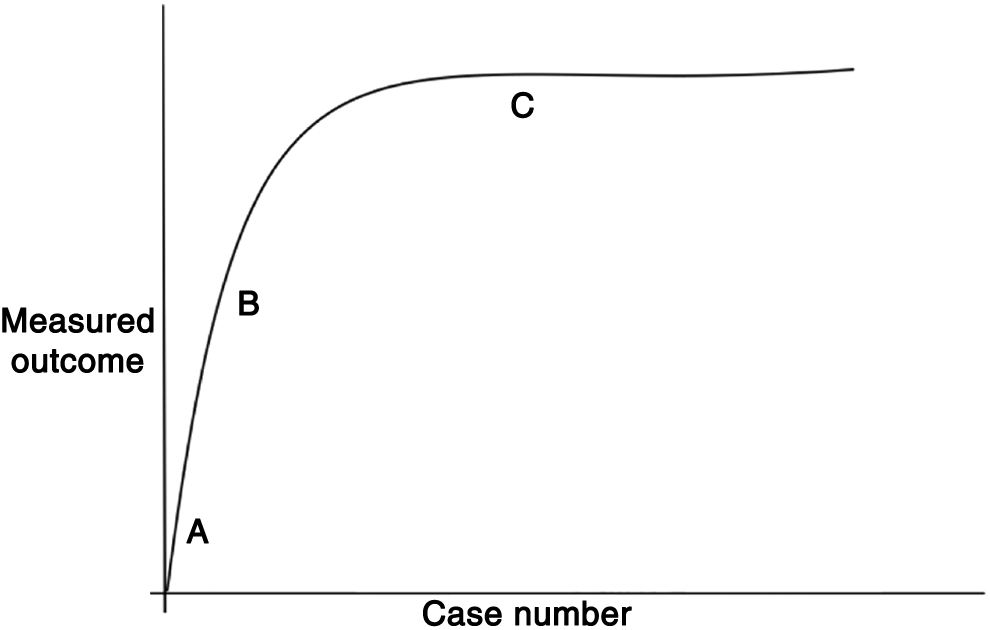
Learning curve.
(1) Starting point: Each person has his or her individual experiences and backgrounds that combine and lead to an initial level of expertise in terms of performing a new procedure.
(2) Slope: How fast a person learns a new task, or the slope of the curve. This slope varies by procedure, by person, and by how many and how often a person has performed a procedure.
(3) Plateau: When the incremental change in the outcome being measured is not significant. This is usually the point at which a person is deemed experienced in a particular task.
A similar idea has been adopted in medicine and surgery. Learning a practical skill becomes easier with time, with an initial period of difficulty, followed by a rate of improvement and stabilization in performance. The LC is a particularly important assessment tool in surgery where a constant stream of new skills must be acquired safely and efficiently.
An important aspect of measuring the LC is choosing the appropriate variables. There are two main types of variables: measuring the surgical process and measuring patient outcomes.7,8 Measures of surgical process include variables such as time to complete the procedure, the success or completion rate of the procedure, and the conversion rate from robotic/laparoscopic to open surgery, and so on.9,10 Measures of patient outcomes include amount of blood loss, length of hospital stay, intraoperative/postoperative complications, mortality, and so on. 11
Some variables are easier to measure than others, but not all variables may be reliable measures of learning. For example, it is easier to measure and statistically analyze data on operating time rather than on patient complications. However, an LC based on operating time alone may not be a useful indictor of good practice. It has been suggested that many variables must be considered to accurately measure an LC and variables should be tailored to the type of procedure. 12 There may be no ideal measure of learning, thus a multivariable approach should be used. As with any variable, confounding factors must be minimized to draw valid conclusions. Organizational factors (facilities, equipment), surgical team (experience, cooperation), and complexity of cases and surgeon's characteristics (previous experience, natural abilities, motivation etc.) can all affect the LC of a procedure. 8 Simulation and inanimate trainers may have a role in minimizing some of these factors (e.g., organizational, case complexity, surgical team, etc.).
Simulation, in particular, is gaining increasing popularity in surgical training. Many types of high- and low-fidelity simulators are now available, including synthetic, animal and cadaveric organ models, as well as mechanical and virtual reality simulators. They allow the trainee to master the LC for complex surgical skills in a controlled environment, without jeopardizing patient safety. Simulators can also act as tools for competency assessment in structured standardized examinations, with the use of checklists and global scoring sheets.
The goal of developing a multivariable and standardized LC is to calculate the number of procedures performed under supervision or in a simulated environment that a surgeon may have to carry out before reaching a safe and competent level of independent performance. Training programs could also use LC data to map progress of trainees. 13 Furthermore, an understanding of the LC is crucial in randomized control trials comparing new procedures with older interventions. 14
Robot-Assisted Surgery in the Context of Open and Laparoscopic Surgery
Robot-assisted surgery evolved from laparoscopy and relies on its basic principles and conduct of operation. Even though some robotic procedures emerged de novo, most require proficiency in laparoscopic conduct of the operation before the skill can be transferred to robotic procedures. Because of this, it is important for trainees to establish proficiency in the conventional surgical approach, whether open or laparoscopic, before learning new robotic techniques. Some trainees could be misled by the relative ease, with which simulated tasks such as peg transfer and camera work can be performed robotically. Yet, real life surgery involves handling live tissue, controlling bleeding, adjusting for bowel peristalsis, respiration, and communication with surgical team away from the operating table. These factors may make approaching operations robotically unfamiliar and an extremely challenging task.
Transfer of skills from open surgery to robotic-assisted surgery
The evidence found in the literature is compelling, but the studies available are not well designed to make generalizations. For example, a surgeon reported transferring open surgical skills to the robotic interface after 8–12 robotic-assisted procedures. 15 Similarly, when Kaul et al. compared the LC of three surgeons of various prior experience levels (a laparoscopic surgeon, an open surgeon, and a fellow), they found that the robot decreased the LC of the open surgeon by case 7. 16 Another study by Johnson and Wood demonstrated that robotic prostatectomy could easily be learned by open surgeons, even those without formal training in laparoscopy, and that a strong mentoring relationship with a colleague with robotic experience enhances the open surgeon's transition to the robotic technique, with equal outcomes. 17 The same transfer of motor skills was also observed in microsurgery. A study of 49 participants demonstrated that surgeons with microsurgery experience had better performance in robotic dry laboratory compared to surgeons without experience. 18
Due to the very small number of participants in these studies, making generalizations is difficult, but we can extrapolate the following conclusions: open surgeons can become proficient in robotic surgery without the need of prior laparoscopic experience; microsurgery training could be an easy training module to familiarize the trainees with the work environment and to acquire sensorimotor skills.
Transfer of skills from laparoscopy to robotic-assisted surgery
Three main aspects differentiate robotic surgery from classic laparoscopy: the fulcrum effect is eliminated, the degree of freedom for the instruments is regained, and a three dimensional view is provided by the system.
As described by Blavier et al., the surgical performance of novices or trainees with lesser surgical experience is enhanced when using the da Vinci robot versus laparoscopic surgery, due to a combination of vision and instrument improvements. 19 In another study, the same authors conclude that novice trainees are the most dependent on the surgery method they train with. After switching the surgical method, low performance scores were measured suggesting that there is no transfer of skills in novice performance. 20 Further, they describe that experts in laparoscopic surgery can readily transfer their motor skills to robotic surgery. In a study by Öbek et al., 21 participants were either trained laparoscopically or robotically for up to 2 hours in knot tying, and then, they had to perform the knot-tying task with the untrained method. Both groups showed transfer of skill. The transfer seems to be better from laparoscopic modality to robotic-assisted than vice versa.
These results support the observation that with increasing laparoscopic experience for specific motor skills, the switch of modalities becomes easier. Overall, the studies show that the level of proficiency of laparoscopic skills corresponds to different needs of the learner for robotic surgery training.
Credentials and Privileges
The final stage in the robotic education process is to obtain credentials and privileges to operate independently. The U.S. Department of Health and Human Services defined credentialing as the process of assessing and confirming the qualifications of a licensed or certified healthcare practitioner. The companion piece to credentialing is privileging, which is the process of authorizing a licensed or certified healthcare practitioner's specific scope of patient care services. Privileges are acquired after the evaluation of an individual's clinical qualifications and performance.
At present, there is no greater governing body mandated credentialing guidelines for robotic surgeons, and the granting of privileges remains institution-based and often includes industry certification, such as the Intuitive Surgical, Inc. certificate. Most requirements vary from hospital to hospital and are not competency based, but rather driven by a fixed number of proctored cases, in which the observer is responsible for an assessment of skills and knowledge. 22 In addition, there are neither standard for proctoring or identifying those who would be qualified to serve as a proctor nor what metrics the proctor should use to determine whether to approve privileges. In general, robotic privileges are not procedure-specific, and once privileged, surgeons can apply robotic technology to other potentially more complex procedures and even procedures that have never been done robotically. From a safety perspective, this is not an ideal process.
Rigorous investigations are needed to find approaches to strengthen hospitals' credentialing of competent surgeons. In addition, ensuring adequate training beyond surgical residency or fellowship is a major challenge for hospitals that want to grant privileges for robotic skills.
Discussion
Robotic platforms such as the daVinci are not just another new tool in the OR. They represent a major evolutionary step that brings remarkable new and complex challenges to the surgeon. Those challenges need to be addressed with well-structured training programs and standardized guidelines. Hereafter, we summarized what we believe to be critical for a successful integration of robotic platform in the normal surgical routine:
Adapting to the robotic platform: first of all, surgeons must become familiar with the new system by making adjustments such as realizing they can longer physically touch the operation site. In surgery, there is always the possibility of an unforeseen situation, and in case of emergency, the detachment from the patient must be overcome by the surgeon's readiness to take action and clearly communicate with the operating team. Adapting to the surgeon's experience: skills gained from laparoscopic or open surgery have been shown to be partly transferrable to robotic surgery, and ideally the training should be tailored to the surgeon's level of experience. Adapting to incoming technologies: Intuitive Surgical, Inc. has introduced several generations of the da Vinci robotic system, and competitors are expected to enter the market in the near future. Robotic training should be regularly updated to support new robot generations and systems. It should also be easily transferable from one robot generation and specification to another.
2
Getting ready for the OR: proficiency in robotic surgery may require the performance of dozens or sometimes hundreds of procedures, which raises the issue of how to obtain the skills. For the sake of patient safety, as much of the LC as possible should be performed outside of the OR. Simulation-based training from low- to high-fidelity simulators is required for that purpose. Surgery simulators are catching up to aviation training standards, but a lot of research is still needed to find the optimal use for simulators in surgery curricula. Credentials and privileges: in the same way that airline pilots need to renew their license every year and demonstrate that they are competent in the skills required to fly an aircraft, surgeons should be required to have some form of licensing for robotic surgery. Clearly, there is a need for standardized guidelines and practices for surgeons to acquire and maintain competency and for institutions to verify credentials and grant privileges. Continuing training: the proficiency level of a surgeon should be reevaluated regularly and from robot generation to robot generation. If the surgeon does not reach the benchmark levels, additional training or remediation should be offered to regain the proficiency.
Conclusions
The transition from open to classical minimally invasive surgery had its fair share of missteps and drawbacks that led to complications and cost human life. We see similar challenges with the wide adoption of robot-assisted surgery. Numerous efforts have been made by surgical societies to define the requisites for robotic surgeons and have focused on creating a standardized curriculum with competency-based assessments and LCs. However, despite these efforts, the responsibility for validating competency and granting privileges still remains in the hands of individual institutions. Therefore, credentials and privileges may vary among providers. Having detailed and standardized credentialing and privileging processes are imperative. Further, there is a need to establish a performance monitoring process to evaluate surgeons' competency over time.
Future developments such as augmented reality, partly automated robots, and evolutionary progress in the robot development seem right around the corner. The competency-based approach is essential to accept new operative technologies and to honor the principle of “above all, do not harm.”
Footnotes
Disclosure Statement
No competing financial interests exist.