
Abstract
Abstract
The endoscopic management of Barrett's esophagus (BE) has changed with the emergence of novel endoscopic technologies and new data informing the care of dysplastic BE and early adenocarcinoma. These changes include an expanded use of endoscopic ablative therapy as well new recommendations for surveillance intervals. For most patients with BE and high-grade dysplasia (HGD), endoscopic ablative therapy is the preferred treatment strategy. Ablation has consistently been shown to be effective, with less morbidity compared with surgery. The best approach to treatment of adenocarcinoma with submucosal invasion is not clear as relevant data are conflicting. Traditionally, submucosal invasion was a contradiction to endoscopic therapy of esophageal adenocarcinoma, but recent data suggest that both endoscopic resection with ablation and esophagectomy may be acceptable treatment options in some settings. At present, surveillance for patients with baseline HGD or intramucosal carcinoma is suggested every 3 months in the first year following complete eradication of intestinal metaplasia, every 6 months in the second year, and annually thereafter.
Introduction
B
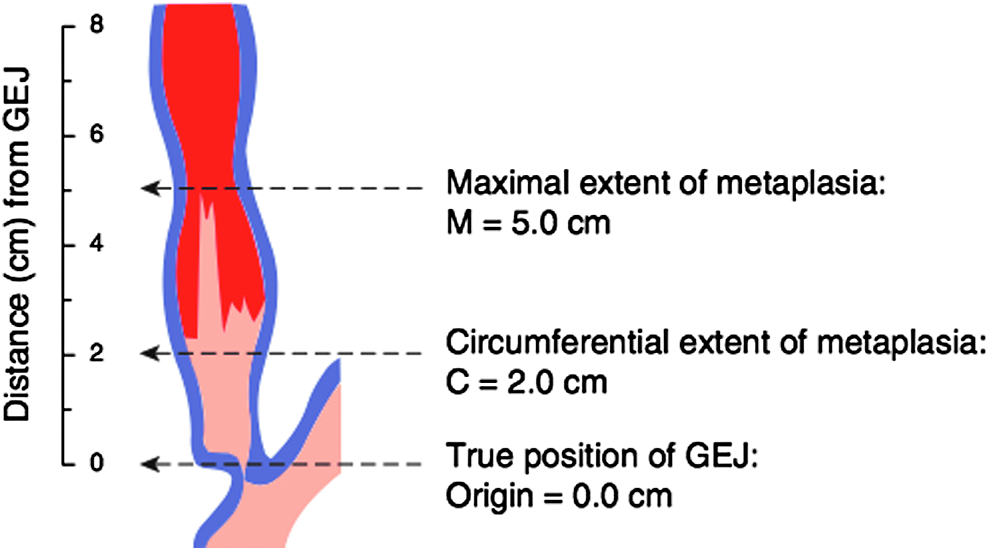
Illustration of Prague Classification for BE. Reproduced with permission. BE, Barrett's esophagus.
A meta-analysis of 19 studies with 7930 patients followed for 33,022 patient years reported mortality rates of patients with BE. 4 There were a total of 1359 deaths of which esophageal adenocarcinoma (EAC) accounted for 88. Of the articles reporting cause-specific mortality, the most common causes of death included heart disease (35%), pulmonary disease (20%), and other cancers (16%). 3 While EAC is an uncommon cause of death in patients with BE, the diagnosis of EAC with regional or distal metastases portends a dismal prognosis. Patients with EAC and regional or distant metastases have < 20% survival at 5 years. 5 As EAC is felt to follow a metaplasia–dysplasia–carcinoma sequence, endoscopic surveillance and intervention may disrupt this pattern and reduce the incidence of EAC. This review will discuss the diagnosis and endoscopic management of dysplastic BE and superficial EAC.
Diagnosis
Evaluation begins with close inspection of the esophageal mucosa during high-resolution endoscopy. Samples from areas of the distal esophagus suspicious for BE are submitted for histologic interpretation after cold biopsy. Biopsies every 2 cm of segment length, or at least eight biopsies if the segment is < 2 cm, are recommended for the initial examination. The mucosa is concurrently scrutinized for nodularity, ulceration, or irregular mucosal contours, which should be sampled separately by biopsy or endoscopic mucosal resection (EMR). The adjunctive application of narrow light spectrum technology, which includes white light endoscopy and narrow band imaging, may increase the accuracy of detection of intramucosal carcinoma (IMC) or high-grade dysplasia (HGD) within irregular mucosal surfaces. 6 EMR or endoscopic submucosal dissection (ESD) should be employed for diagnosis and therapy if nodularity is found during inspection.7,8 EMR is generally adequate to provide the depth of invasion, which drives further clinical decisions. ESD is more technically demanding and should be employed by clinicians with expertise in this technique. This procedure, however, allows for better characterization of the lateral margins of a lesion.
The best surrogate marker for cancer risk in patients with BE remains dysplasia. Thus, an accurate diagnosis of dysplasia is essential. Significant interobserver variability exists in the interpretation of dysplasia, although there is greater agreement among GI pathologists for the extremes of dysplasia, including intestinal metaplasia (IM) without dysplasia and HGD/EAC. 9 As such, available evidence supports the importance of confirming all readings of dysplasia by a second pathologist experienced with histological interpretation of such specimens.10,11
Management
The histologic interpretation of initial endoscopic biopsies and/or mucosal resection informs further management. Surveillance endoscopy is appropriate for nondysplastic BE. Indeterminate lesions should be reassessed by an additional endoscopy. Endoscopic intervention should be considered for patients with dysplastic BE or superficial EAC (Fig. 2).
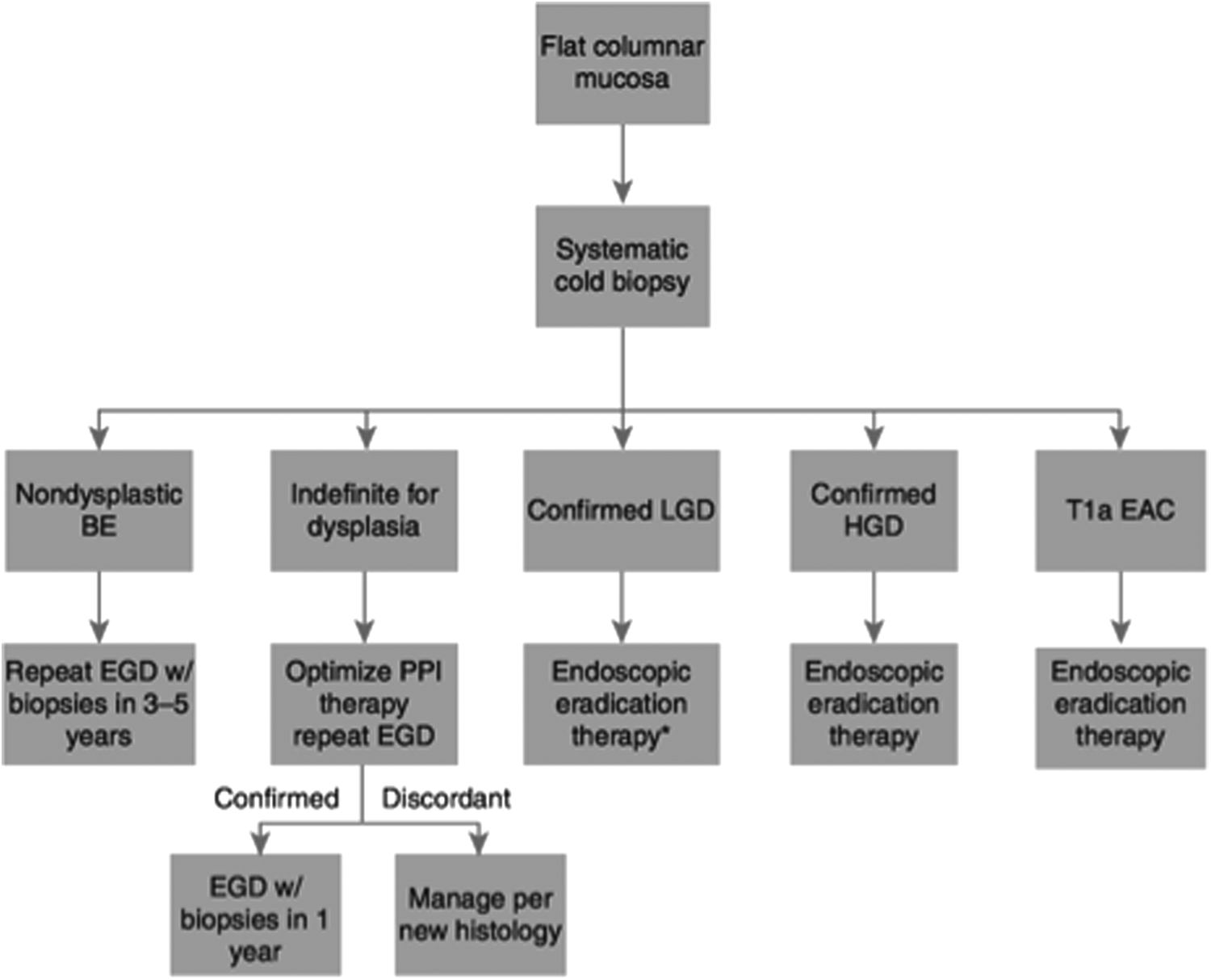
Management of nodular BE. Although endoscopic eradication therapy is associated with a decreased rate of progression, surveillance upper endoscopy at 1-year intervals is an acceptable alternative. The above schema assumes that the T1a EAC displays favorable characteristics for endoscopic therapy, including well-differentiated histology and lack of lymphovascular invasion. EAC, esophageal adenocarcinoma; EGD, esophagogastroduodenoscopy; HGD, high-grade dysplasia; LGD, low-grade dysplasia; PPI, proton pump inhibitor. Reproduced with permission from ACG Clinical Guideline: Diagnosis and Management of Barrett's Esophagus. BE, Barrett's esophagus.
The goal of therapy for patients with low-grade dysplasia (LGD) or HGD is complete eradication of not just the dysplastic tissue but also complete eradication of intestinal metaplasia (CEIM), which decreases the likelihood of recurrent dysplasia. Management of EAC is more nuanced and considers the degree of tumor differentiation, depth of tumor invasion, and lymphatic involvement. When present, nodular lesions should first be completely resected before utilizing endoscopic ablative therapy.
The best studied endoscopic modalities utilized in the treatment of dysplastic BE include photodynamic therapy, radiofrequency ablation (RFA), and cryotherapy. Photodynamic therapy was shown to produce complete eradication of HGD when compared with untreated controls with BE and HGD (77% vs. 39%, P < 0.0001) and to decrease the occurrence of adenocarcinoma (13% vs. 28%, P < .006). 12 However, the expense of the procedure, along with the relatively high incidence of densely fibrotic strictures, has limited its use. In a study of 127 patients randomized to receive RFA or a sham procedure, complete eradication of HGD was documented in 81% of those in the ablation group versus 19% of those in the control group (P < .001). When including patients with LGD and HGD, patients in the ablation groups had fewer cancers versus the sham procedure (1.2% vs. 9.3%, P = .045). In this study, 2.4% of the treated patients with HGD progressed to EAC compared with 19.0% of the sham arm. Adverse events were limited and included three serious events possibly or probably associated with the procedure in the RFA arm compared with zero in the control group (P = .55). No procedure-related deaths were recorded. 13 Retrospective cohort studies of cryotherapy have demonstrated high rates of CEIM and neoplasia with minimal side effects.14,15 Given the current state of the literature, the well-documented efficacy and side effect profile of RFA make this the preferred modality for most patients.
For most patients with BE and HGD, endoscopic ablative therapy will be the preferred treatment strategy. Ablation has proven to be effective with less morbidity compared with surgery. Long-term survival of endoscopically treated patients with HGD has also been shown to be similar to that of esophagectomy patients. Over a 5-year follow-up period, 11/129 (9%) patients treated with photodynamic therapy for HGD versus 6/70 (8.5%) of patients treated with esophagectomy for HGD were deceased. 16
In contrast to BE with HGD, the management of superficial adenocarcinoma requires consideration of multiple factors. Determining the depth of invasion of EAC is paramount in understanding the curative potential of endoscopic therapy. Lesions confined to the mucosa (T1a) may generally be treated with mucosal resection (i.e., EMR/ESD), followed by ablative therapy for eradication of remaining BE. 7 This is due to the relatively low rate of lymph node metastases in such patients. 17 EMR as a stand-alone treatment for T1a lesions or those invading the submucosa (T1b) EAC is not adequate. Patients with complete resection of a T1a EAC as well as endoscopically treated T1b lesions should undergo subsequent ablation of the entire BE segment. A prospective case series reported that ∼1 in 3 patients with complete resection of the tumor after EMR will later develop recurrent HGD or EAC 7 without ablative therapy. Other factors also influence the decision of endoscopic versus surgical treatment of T1a adenocarcinoma. Specifically, moderate or poor differentiation, as well as the presence of lymphatic or vascular invasion, has been suggested as an indicator of worse prognosis with endoscopic therapy.
Data are conflicting regarding the optimal approach to treatment of adenocarcinoma with submucosal invasion. While submucosal invasion has traditionally been suggested as a contraindication to endoscopic therapy of EAC, recent data suggest that both endoscopic resection with ablation and esophagectomy may be viable modalities. The utilization of endoscopic resection in this regard may be best reserved to highly selected patients with low-risk lesions, as defined below.
A prospective study of 66 patients with low-risk EAC with superficial submucosal invasion (also known as sm1 invasion) analyzed outcomes of endoscopic therapy. Low-risk lesions were defined as sm1 EACs that were macroscopically polypoid or flat, with a differentiation grade of G1–2, as well as no tumor invasion in lymphatic vessels (L0), or blood vessels (V0). In their cohort, 87% of the patients had complete eradication of neoplastic tissue. The response rate was found to be 97% in lesions of 2 cm or less in diameter. Over the course of their study, metachronous neoplasms were found in 10 patients. However, 9 of 10 patients returned to remission with repeat endoscopic therapy. A lymph node metastasis was found in 1 patient during the follow-up interval. Long-term remission was defined as patients who achieved primary complete endoscopic remission, any metachronous neoplasia had curative endoscopic therapy, and if no extraesophageal signs of tumor were diagnosed in the follow-up period. This was obtained in 84% of patients with a mean follow-up period of ∼4 years; this was increased to 90% in patients with a lesion of 2 cm or less. A 5-year survival rate was calculated at 84% with no deaths associated with the tumor. Major complications of endoscopic resection were 1.5%, and there were no deaths attributed to therapy. 8
Clearly, the efficacy of endoscopic therapy for EAC with submucosal invasion is limited by its inability to assess or treat lymph node metastases. Therefore, regardless of how good the endoscopic technique becomes, endoscopic approaches will be ineffective in patients with high likelihood lymph of node involvement. A retrospective study analyzing 54 T1 EACs from 258 esophagectomy samples showed that nodal metastases were present in 21% (3/14) of sm1, 36% (4/11) of sm2, and 50% (2/4) of sm3 tumors; sm1, sm2, and sm3 corresponding to superficial, mid, and deep invasion of the submucosa, respectively. 18 Rates of nodal metastases have differed somewhat in other analyses,18,17 with some studies showing lower risks of lymph node involvement in sm1 disease. Consistently, however, T1b sm2–3 lesions show high frequencies of lymphatic involvement. As such, T1a or T1b EAC with poor differentiation, lymphatic involvement, or invasion into the mid or deep submucosa should be considered for esophagectomy either alone or in conjunction with other modalities (chemotherapy +/− radiation). Whether T1b EAC with superficial submucosal invasion (sm1) and other favorable characteristics is best treated with endoscopic or surgical approaches remains an open question, although early data reporting endoscopic outcomes in this patient group are promising.
The goal of endoscopic therapy is the complete eradication of dysplasia and IM within the esophagus. While most studies have defined this as a single endoscopy demonstrating endoscopic and histologic eradication of intestinal metaplasia in the tubular esophagus, some authorities have defined this endpoint as two disease-free endoscopic sessions given the sampling error inherent in endoscopic biopsies. 19 Likewise, the number of sessions of endoscopic therapy necessary before a patient is deemed a failure of endoscopic therapy for neoplastic BE is also not well defined. Cohort study data demonstrate that even among patients who had undergone four sessions of RFA without CEIM, >50% eventually attained CEIM with further endoscopic therapy. 20 Thus, in a subset of patients, multiple endoscopies may be necessary for complete treatment, and a concrete cutoff number defining endoscopic failure thus cannot be provided.
Follow-up
Available cohort data underscore the importance of close endoscopic surveillance following CEIM. Rates of recurrence of BE following initially successful RFA exceed 20% in most studies.19,21,22 Fortunately, most of these recurrences involve scant amounts of tissue and are nondysplastic in nature. 22 However, up to one in four recurrences may either be dysplastic or harbor adenocarcinoma.19,23 Data from several case series have also documented the occurrence of dysplasia in the gastric cardia following CEIM. 24 Whether this represents de novo development of dysplasia, as opposed to pre-existing cardia dysplasia not diagnosed due to sampling error, is unclear. However, endoscopic surveillance with routine biopsies of the GEJ and cardia should follow CEIM to help detect recurrent disease. It is recommended that biopsies from unique anatomical loci be placed in separate bottles to help localize the site of recurrence. Expert opinion alone informs the interval for follow-up examinations: surveillance for patients with baseline HGD or IMC is suggested every 3 months in the first year following CEIM, every 6 months in the second year, and annually thereafter. For patients with LGD, surveillance is recommended every 6 months in the first year and annually thereafter. 1 Given the diminished likelihood of developing EAC following successful RFA,20,25 these intervals may be too conservative, and current work using cohort data to create evidence-based surveillance intervals is underway.
Recurrent metaplasia and dysplasia after therapy are usually amenable to further EMR and ablation26–28 utilizing similar strategies as those employed for a new diagnosis. However, a few cases of invasive carcinoma have been reported requiring esophagectomy. 29 Of note, the finding of subsquamous BE after endoscopic therapy has been a concern for providers. Reported rates of subsquamous intestinal metaplasia are variable after ablation ranging from 0.9% after RFA to 14.2% after photodynamic therapy.28–30 Studies using novel imaging techniques suggest that this rate might be substantially higher, and the majority of patients might in fact harbor residual subsquamous BE. Buried disease was found with a prevalence of 63% when evaluated with three-dimensional optical coherence tomography after RFA. 31 Some studies suggest that surveillance biopsies following ablation may be too superficial to detect subsquamous BE, 32 although this has not been confirmed. 33 Regardless of the rate of residual buried intestinal metaplasia, it must be a low-risk lesion for progression to EAC given the thousands of patient-years of follow-up reported following ablative therapy, with very few subsquamous EACs.
Conclusions
The endoscopic management of BE has changed with the emergence of novel endoscopic technologies and new data informing the care of dysplastic BE and early adenocarcinoma. These changes include an expanded use of endoscopic ablative therapy as well new recommendations for surveillance intervals. This review summarized these changes and discussed the diagnosis and endoscopic management of dysplastic BE and superficial EAC.
For most patients with BE and HGD, endoscopic ablative therapy is the preferred treatment strategy. Ablation has consistently been shown to be effective, with less morbidity compared with surgery. The best approach to treatment of adenocarcinoma with submucosal invasion is not clear as relevant data are conflicting. Traditionally, submucosal invasion was a contradiction to endoscopic therapy of EAC, but recent data suggest that both endoscopic resection with ablation and esophagectomy may be acceptable treatment options in some settings. At present, surveillance for patients with baseline HGD or IMC is suggested every 3 months in the first year following CEIM, every 6 months in the second year, and annually thereafter.
Guidelines for the management of BE will continue to evolve with the development of new technologies. This will likely include the advent of less invasive and less expensive screening modalities for BE. As such, it is probable that recommendations will continue to change with time.
Footnotes
Acknowledgments
Dr. Shaheen receives research funding from Medtronic, CSA Medical, Interpace Diagnostics, and CDx Medical. The other authors received research funding from Medtronic for this study. This research was funded by T32 DK07634 from the National Institutes of Health and Medtronic.
Disclosure Statement
No competing financial interests exist.