
Abstract
Abstract
Purpose:
Conventional laparoscopic appendectomy (CLA) has been considered the standard for the treatment of acute appendicitis. Recently, single incision laparoscopic appendectomy (SILA) has become an alternative option. There are few reports on the results of SILA performed by residents during the training period. The present study, we report our residents' experience.
Materials and Methods:
We reviewed clinical characteristics and outcomes of 1005 patients who underwent appendectomy between October 2013 and April 2016. Every operation was performed by only residents. Clinical characteristics and operative outcomes between SILA and CLA group were reviewed after propensity score matching.
Results:
SILA was used more frequently in younger patients (23.3 versus 36.4 years, P = .000), women (66.4% versus 45.9%, P = .000), and patients with lower body mass index (20.2 versus 22.9 kg/m2, P = .043). After propensity score matching, the rate of complicated appendicitis was lower (12.9% versus 15.5%, P = .573), and the mean operative time was slightly shorter in the SILA group than in the CLA group (56.68 versus 59.09 minutes, P = .068), although these differences were not statistically significant. There were no significant differences between the two groups in hospitalization period (2.7 versus 2.9 days, P = .380), the use of analgesics (2.0 versus 2.1 times, P = .128), and wound complication rate (10.3% versus 14.6%, P = .333).
Conclusion:
It is a safe and relatively easy procedure with an acceptable postoperative cosmetic outcome that can be incorporated into the routine surgical training.
Introduction
O
Several randomized clinical trials comparing the outcomes of SILA and CLA have been performed to date. However, a consensus regarding the objective benefits of SILA has not been reached. Furthermore, there are few reports on the results of SILA performed by residents during the training period despite the fact that appendectomy is the first skill learned during training. Therefore, whether SILA can be performed safely as an alternative procedure for a resident is debatable. The present study compared the clinical outcomes of SILA and CLA to assess the feasibility of SILA performed by surgery residents.
Materials and Methods
The present retrospective study was approved by the Institutional Review Board of Ulsan University Hospital (Ulsan, South Korea). The clinical characteristics and outcomes of 2104 patients who underwent appendectomy between October 2013 and April 2016 were reviewed. Appendicitis was diagnosed based on physical findings and ultrasonography and computed tomography results. Patients who underwent open appendectomy and incidental appendectomy were excluded. Among the included patients, 116 underwent SILA and 889 underwent CLA. Patients were then assigned to SILA or CLA after propensity matching (Fig. 1).

Flowchart illustrating the study group. CLA, conventional laparoscopic appendectomy; SILA, single incision laparoscopic appendectomy.
During the study period, all operations were performed exclusively by residents. All patients with a clinical diagnosis of acute appendicitis were given the option of SILA or CLA. The severity of the disease ranged from simple acute appendicitis to complicated appendicitis defined as an appendiceal perforation or abscess. 4 In Korea, surgical residency training begins at the postgraduate year 2 level or later and ends after 4 years. Resident participation in laparoscopic surgery as the primary surgeon is part of the training system, and appendectomy is one of the basic steps of the curriculum. In our hospital, residents that complete the prescribed preparative program (education by senior residents or board-certified surgeons assisting in several procedures) are permitted to act as the primary surgeon in the operating room under the supervision of a senior resident or attending surgeon until they complete more than 10 CLA. SILA was performed by residents with expertise in the CLA procedure.
For all operations performed by residents, gender, age, and body mass index (BMI) were compared between the two groups (SILA versus CLA). The rate of complicated appendicitis and clinical outcomes, including operative time, need for additional ports, postoperative length of stay, frequency of conversion to open surgery, and rate of postoperative wound complications, was compared after propensity score matching. Propensity score matching was performed using a binary logistic regression model to account for and limit selection biases, as well as confusion between the two groups. The following three independent pretransplant factors that had likelihood of having SILA were included in the binary logistic regression model to calculate the propensity score: gender, age, and BMI. To analyze the learning curve of CLA, patients were consecutively assigned to four groups at the end of the training period: group A (the first year of training), group B (the second year of training), group C (the third year of training), and group D (the fourth year of training). Mean operative time and rate of wound complications were analyzed. Statistical analyses were performed with IBM SPSS 21 for Windows (IBM, Armonk, NY). Results were compared using the t-test, ANOVA test, and correlation test. P values of <.05 were considered statistically significant.
SILA surgical technique
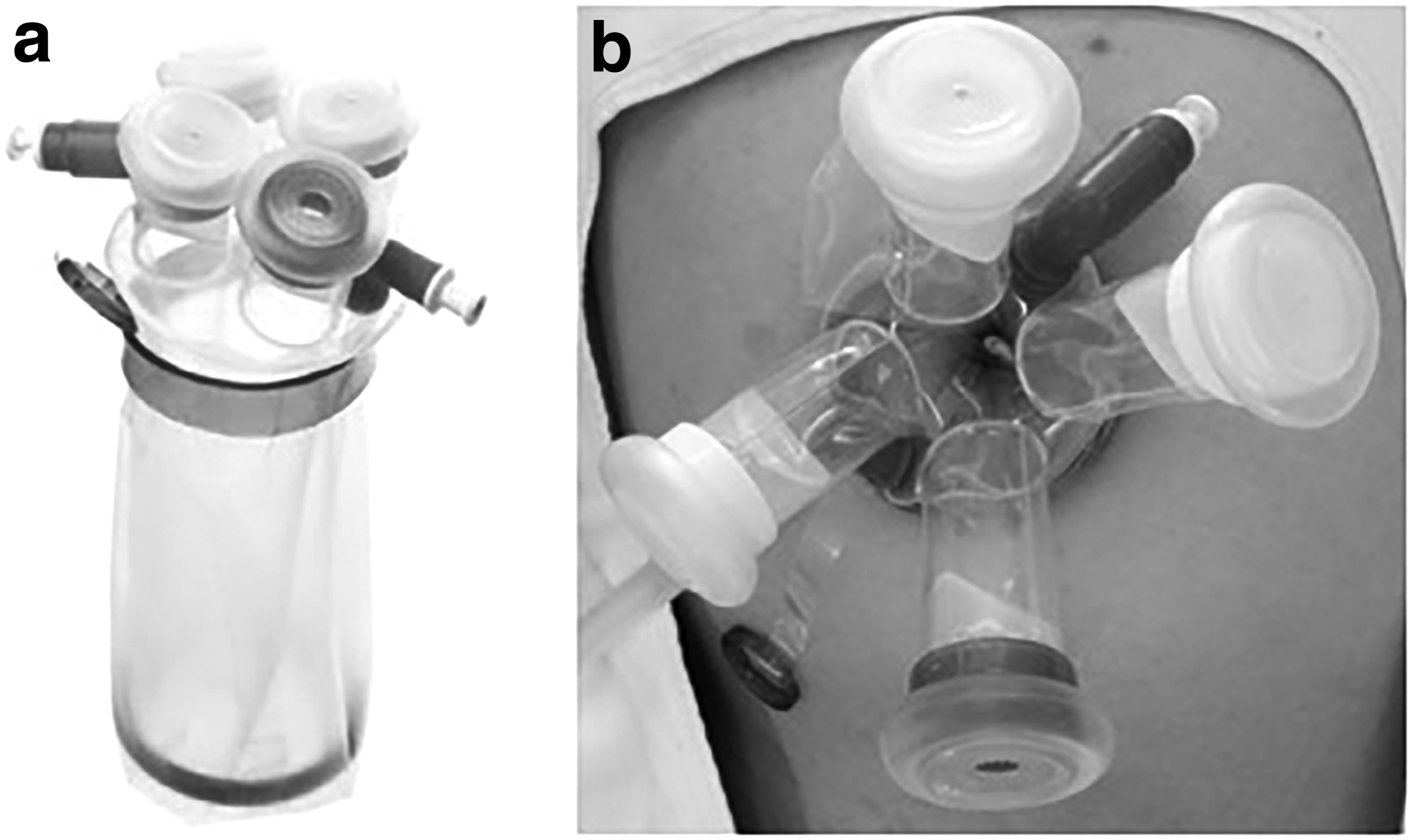
A 2.0 cm transumbilical vertical skin incision was used for single-site access. After the skin incision was made, a wider, ∼3.0 cm, incision was made in the umbilical fascia. A Glove port (NELIS, Bucheon, Korea) (Fig. 2), which has three trocar channels, was then inserted into the access site incision. After achieving pneumoperitoneum, a rigid 30° 10 mm telescope was placed into the peritoneal cavity. Two laparoscopic instruments were then introduced into the peritoneal cavity. Only straight-type instruments were used. Under direct visualization, an energy device (Harmonic Scalpel; Ethicon Endo-Surgery, Inc., Cincinnati, OH or LigaSure; Covidien, Mansfield, MA) was used to dissect the mesoappendix and appendiceal artery. The appendiceal base was then ligated using an endoloop absorbable thread (Ethicon, Somerville, NJ) or Hem-o-lok clip (Weck Closure Systems, Research Triangle Park, NC) and divided using an energy device. Extraction of the appendix was performed using the Glove port pouch. The cross section of the appendiceal base was coagulated by electrocautery, and the abdominal cavity was irrigated. At the conclusion of the procedure, the fascia and subcutaneous layer were closed using an interrupted 3-0 absorbable suture (Vicryl; Ethicon), and the skin incision was closed using a skin stapler device or leave it if skin gathered naturally.
CLA surgical technique
CLA required the introduction of a 30° 10 mm rigid scope through a 1 cm infraumbilical incision or 1 cm incision at the lower umbilicus. Two additional incisions were made for the insertion of additional ports. A 5 mm trocar was inserted in the suprapubic region to the right lower quadrant, and another 5 or 12 mm trocar was inserted in the left lower quadrant. The intra-abdominal appendectomy procedure was performed through these three ports as described for the SILA procedure. Appendix specimens were retracted using a specimen retrieval bag and removed through the umbilical incision. The umbilical fascia was closed using an interrupted 3-0 absorbable suture. Skin incisions were closed using a skin stapler device.
Postoperative care
Patients received routine intravenous administration of second generation cephalosporin from the time of diagnosis until postoperative day 1. In cases of complicated appendicitis, third generation cephalosporin was used and metronidazole was added until the fever was controlled. Diet was started on the day after surgery. Nonsteroidal anti-inflammatory drugs were injected upon patient request. Opioids were administered according to the surgeon's judgment if pain was severe. The wounds were cured every 2 days for 1 week. Patients were discharged when they were able to tolerate a regular diet and no other specific symptoms were present. Patients returned for regular follow-up at 1 week after discharge.
Results
The records of 1005 patients with acute appendicitis who underwent laparoscopic appendectomy were reviewed. Among these patients, 116 underwent SILA and 889 underwent CLA. Patient characteristics differed significantly between the two groups. SILA was used more frequently in younger patients (23.3 versus 36.4 years, P = .000), women (66.4% versus 45.9%, P = .000), and patients with lower BMI (20.2 versus 22.9 kg/m2, P = .043) (Table 1).
BMI, body mass index; CLA, conventional laparoscopic appendectomy; F, female; M, male; SILA, single incision laparoscopic appendectomy.
After propensity score matching, the rate of complicated appendicitis was lower (12.9% versus 15.5%, P = .573), and the mean operative time was slightly shorter in the SILA group than in the CLA group (56.68 versus 59.09 minutes, P = .068), although these differences were not statistically significant (Table 2). There were no cases of conversion from SILA to CLA or from CLA to open appendectomy. There were no significant differences between the two groups in hospitalization period (2.7 versus 2.9 days, P = .380) and the use of analgesics (2.0 versus 2.1 times, P = .128). In the SILA group, wound complications, including seroma and discharge at the umbilical port site, developed in 12 patients (10.3%). In those patients, daily wound dressing was needed until complete recovery. Wound problems developed in 17 patients (14.6%) in the CLA group, with no statistically significant differences between the two groups (10.3% versus 14.6%, P = .333).
BMI, body mass index; CLA, conventional laparoscopic appendectomy; F, female; M, male; SILA, single incision laparoscopic appendectomy.
Mean operative time decreased yearly in all groups except the SILA group (P = .000) (Fig. 3). In particular, mean operative time decreased significantly between the second and third years in the CLA group for simple appendicitis (83.77 versus 69.36 minutes, P = .016) and in the entire group (68.46 versus 59.45, P = .001) (Table 3). There was no significant decline in the rate of wound complications in all groups (Fig. 4).

Changes in operative time according to training period.
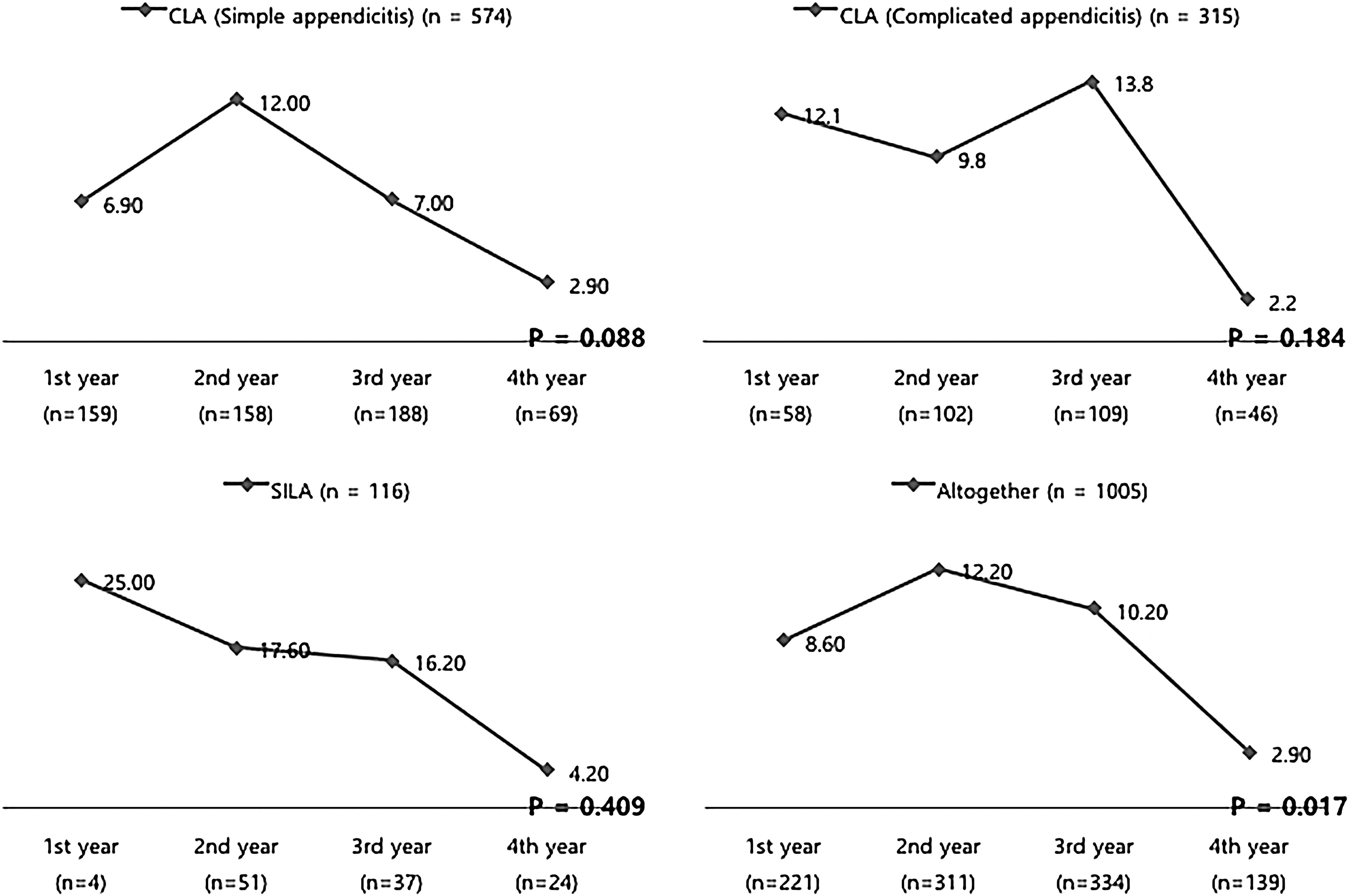
Changes in the rate of wound complications according to training period.
CLA, conventional laparoscopic appendectomy; CLA 1, simple appendicitis group; CLA 2, complicated appendicitis group; SILA, single incision laparoscopic appendectomy.
Discussion
Single incision laparoscopic surgery has become increasingly popular, and SILA is one of the most basic single incision laparoscopic surgery procedures. An early theoretical concern regarding single incision laparoscopic surgery was that the reduced surgical access and visualization might compromise patient safety. 5 Reports suggested that SILA might be associated with a higher incidence of wound infection 6 or increased pain. 7 However, recent advances in laparoscopic instruments and optical systems have facilitated the SILA procedure. St Peter et al. 8 reported the results of a prospective randomized trial and showed the clinical relevance of SILA. Other studies reported that SILA improves cosmetic outcomes and is a valid and safe procedure in uncomplicated cases.5,9 Studies assessing the results of laparoscopic appendectomies performed by residents10,11 showed that CLA is a feasible procedure for residents. In addition, the feasibility and safety of SILA performed by residents were reported in other studies.12,13 In the present study, the surgical outcomes of SILA performed by residents were not significantly different from those of CLA. The appendectomy wound (acute appendicitis) is classified in the contaminated group, and its infection rate is 20%–25%. 14 The rates of wound complications after appendectomy in our center are lower than those of other complicated surgeries. In addition, the mean operative time was shorter than that reported in other studies.
There are currently no clear data on the minimum number of laparoscopic appendectomies required to achieve proficiency. 15 The European Association for Endoscopic Surgeons consensus statement (1995) recommends a minimum of 20 cases for accreditation in general surgery. 16 In our center, residents perform more than 30 appendectomies in 1 year. In the present study, patients were divided into four groups and differences in outcomes were assessed during the initial learning curve. Although the patients assigned to senior residents included more cases of complicated appendicitis, the mean operative time after 1 year was shorter for senior than for junior residents. There were no significant differences between the first year and second year groups. However, the mean operative time decreased significantly each year. This suggested that the first year of training is sufficient for residents to learn the CLA procedure, and after 2 years of training, the resident becomes nearly expert. There are two learning curves. In the first learning curve, the operators require supervision and the operative time is longer compared with experts. In the second learning curve, the operators acquire their own skills and reduce surgery time. In the present study, the two learning curves were completed during the 2 years of training. In the SILA group, only four cases were performed by junior residents and all were performed at 11 months after the start of training. Therefore, all SILA cases were performed after the residents completed the first learning curve of CLA. These data indicate that SILA and CLA may achieve similar surgical outcomes by residents with limited experience and suggest that surgeons can achieve surgical skills for SILA after 2 years of training.
In our center, all residents perform more than 100 appendectomies during the training period and are trained to perform SILA at 1 year after the start of their training. However, in Korea, most appendectomies are performed in small centers, and a small number of appendectomy cases are treated in training centers. In contrast with our center, many residents cannot overcome the learning curve during the training period. Additional multicenter studies are needed to further assess the feasibility of the procedure. Furthermore, there is no standardized training system for laparoscopic surgery in Korea. Some studies introduce basic skills using a training box and live animals at the beginning of residency. 11 Since the use of laparoscopic techniques is increasing, the training of residents and the implementation of standardized training models have become increasingly important.
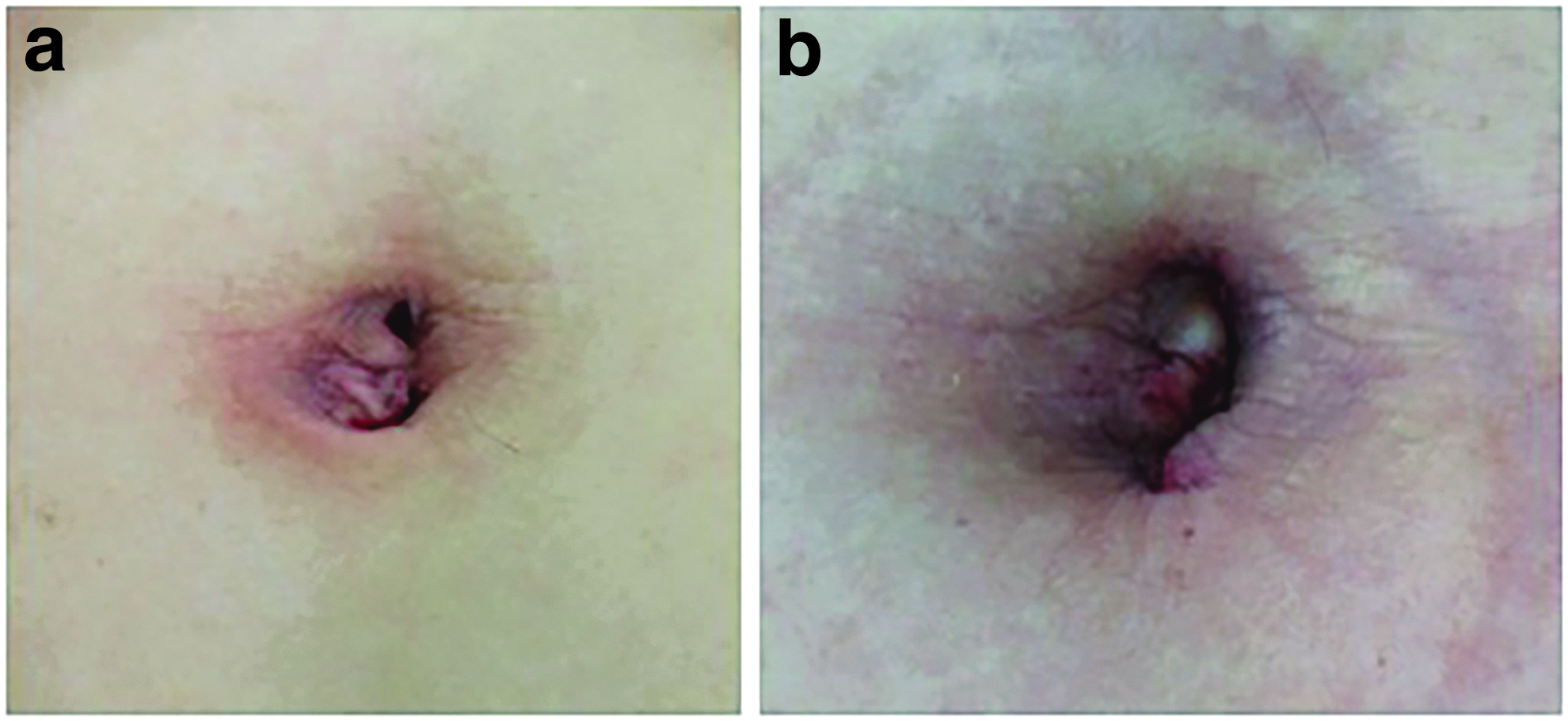
Because of the retrospective design of the present study, the clinical characteristics of the patients were not homogenous. Compared with the CLA group, the SILA population was younger and had a lower BMI, and the percentage of women was higher. Because young slim women want few wound sites or an invisible surgical wound, we compared surgical outcomes between the two groups after matching, which reduced the selection bias. However, propensity score matching may not be able to account for all potential confounders. There may have been other considerations such as prior abdominal operation that made SILA not feasible and were also related to the difficulty of the surgery. This can be a source of residual selection bias. In the National Nosocomial Infections Surveillance System, the risk of wound infection is stratified according to three important factors: wound classification, longer duration of operation, and the medical characteristics of the patients. 14 However we excluded the medical history, previous abdominal surgical history, and presence of pregnancy from the analysis, which limit the evaluation of risk factor of complicated wounds. Patients were followed up only at 1 week after discharge if they had no wound complications. Since evaluation was limited to the immediate postoperative status of the wound, satisfaction with the long-term results was not determined (Fig. 5). Long-term follow-up of operative wounds is necessary, and the cosmesis of the wound should be assessed through a questionnaire or a standard test such as the Vancouver scar scale. 17 Another limitation is that the trial was designed for residents, which may limit the generalization of the results to other practice settings. A comparison of the resident group and the consultant group is needed based on similar patient demographics and surgical techniques.
In the present study, although senior residents performed complicated appendectomies, the operative time was shorter in the senior resident group than in the junior group. In addition, all SILA procedures were performed by senior residents, and the surgical outcomes of SILA did not differ from CLA groups. Even surgeons proficient in SILA require a substantial learning curve to safely perform the SILA technique, and results showed that senior residents overcome their learning curve of SILA during the training period performing CLA. The learning curve of CLA may stabilize after performing 30 operations or fewer. We suggest that SILA is safe and feasible when performed by senior residents who overcome the learning curve of CLA.
In conclusion, SILA is a feasible alternative even for resident level surgeons if they overcome the learning curve. It is a safe and relatively easy procedure with an acceptable postoperative cosmetic outcome that can be incorporated into the routine surgical training.
Footnotes
Acknowledgments
The authors express their sincere thanks to the residents for their efforts.
Disclosure Statement
No competing financial interests exist.