
Abstract
Abstract
Background:
Laparoscopic local gastric resection has become the standard form of surgery for gastric submucosal tumors (SMTs) and is currently being actively selected for these cases. However, total gastrectomy or proximal gastrectomy is performed when tumors are adjacent to the cardia of stomach. Unfortunately, these procedures are highly invasive and can cause marked decreases in activities of daily living. We perform a single-incision laparoscopic intragastric surgery (sLIGS), which are both minimally invasive and offers improved cosmetic outcomes, to treat SMT located adjacent to the esophagogastric junction (EGJ).
Methods:
In this procedure, resection is performed from the gastric lumen side to completely eradicate the cancer while preserving the function of the cardiac sphincter. A 3-cm longitudinal skin incision and gastrotomy are made in the umbilical region, which are protected with a mini-size wound-protecting device. A dedicated wound sealer for single incision surgery is assembled on the wound-protecting device, and three 5 mm surgical ports are placed. Two 5 mm ports are replaced with one 12 mm port to introduce surgical stapling device. The tumor is then staple-transected under countertraction provided by an ultrathin loop retracting device.
Results:
sLIGS has been performed in 4 patients, and none needed to be converted to open surgery. The median operative time was 149 (range 116–170) minutes and blood loss 30 (0–43) mL. No major perioperative complication was observed except for one case which was postoperative bleeding.
Conclusion:
sLIGS is a safe, realistic, and potentially effective procedure for gastric SMTs adjacent to the EGJ.
Background
L
The SMTs with intragastric growth form, located adjacent to esophagogastric junction (EGJ), are difficult to localize from outside the gastric wall, which poses technical challenges for local resection. Simple laparoscopic wedge resection is often technically difficult, making it necessary to switch to proximal or total gastrectomy in some cases. These may lead to decreased quality of life (QOL) due to severe postoperative reflux and/or weight loss.17,18
We first applied LIGS to gastric SMTs in 1997. 7 The greatest strength of LIGS is the minimized resection margins monitored with simultaneous use of flexible endoscopy. We reported its clinical usefulness for cases with gastric SMTs located adjacent to EGJ in 2012. 11 One weak point of LIGS is the technical difficulty in stabilizing each surgical port between the abdominal wall and the gastric wall. This may happen in any of three surgical ports in original LIGS procedures, resulting in frequent “port escapement.” 9
With continuous technical and instrumental modifications, we have successfully merged LIGS with SILS. This “single incision LIGS” (sLIGS) may preserve all beneficial features of LIGS and further improve cosmetic outcomes. Since all surgical ports are placed through the umbilical access device, the technical concerns related to “port escapement” can be minimized. In this communication we describe our recent clinical experience with sLIGS, as well as its technical details. (See Supplementary Video; Supplementary Data are available online at www.liebertpub.com/lap)
The sLIGS Technique
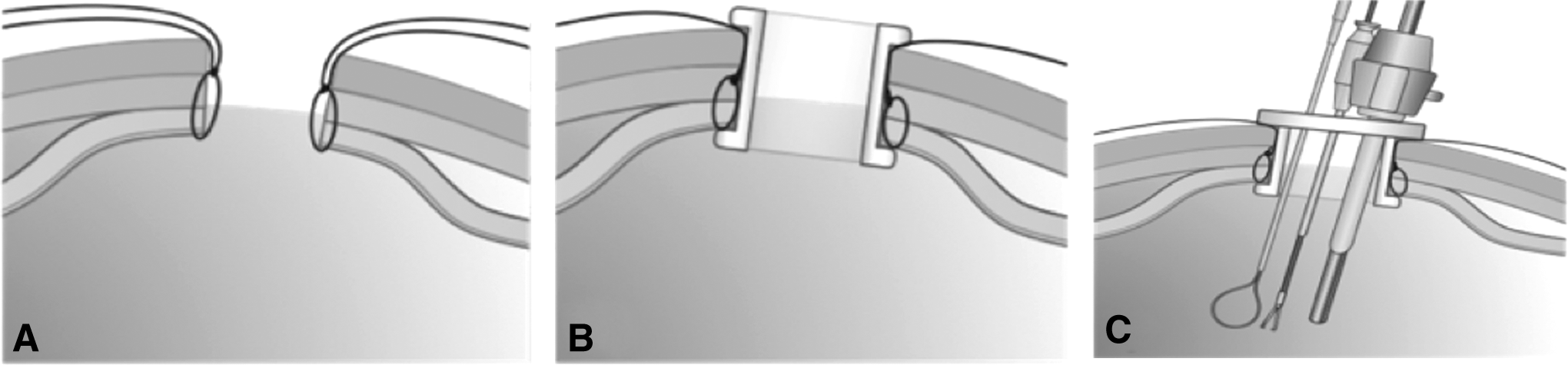
Under general anesthesia in the lithotomy position, a 3 cm longitudinal incision is made in the umbilical region and protected with a mini-size wound-protecting device (Wrap Protector Mini, 29150150; Hakko, Nagano, Japan) (Fig. 1). The initial flexible endoscopy is advanced per orally to identify the gastric lesion and to locate the optimal intragastric access site (Fig. 2). The access site is secured with clamps and exteriorized using the umbilical wound. The gastric wall is then incised under direct vision. A 2.5 cm gastrotomy is fashioned, and the wound-protecting device is advanced into the gastric lumen to secure both abdominal and gastric walls. A dedicated wound sealer for single incision surgery (EZ Access, 29150510; Hakko) is assembled on the wound-protecting device, and three 5 mm surgical ports are placed. One port is used for the laparoscope and the others for the forceps. Figure 3A–C depicts the assembly of wound-protecting device and its sealer for above steps.
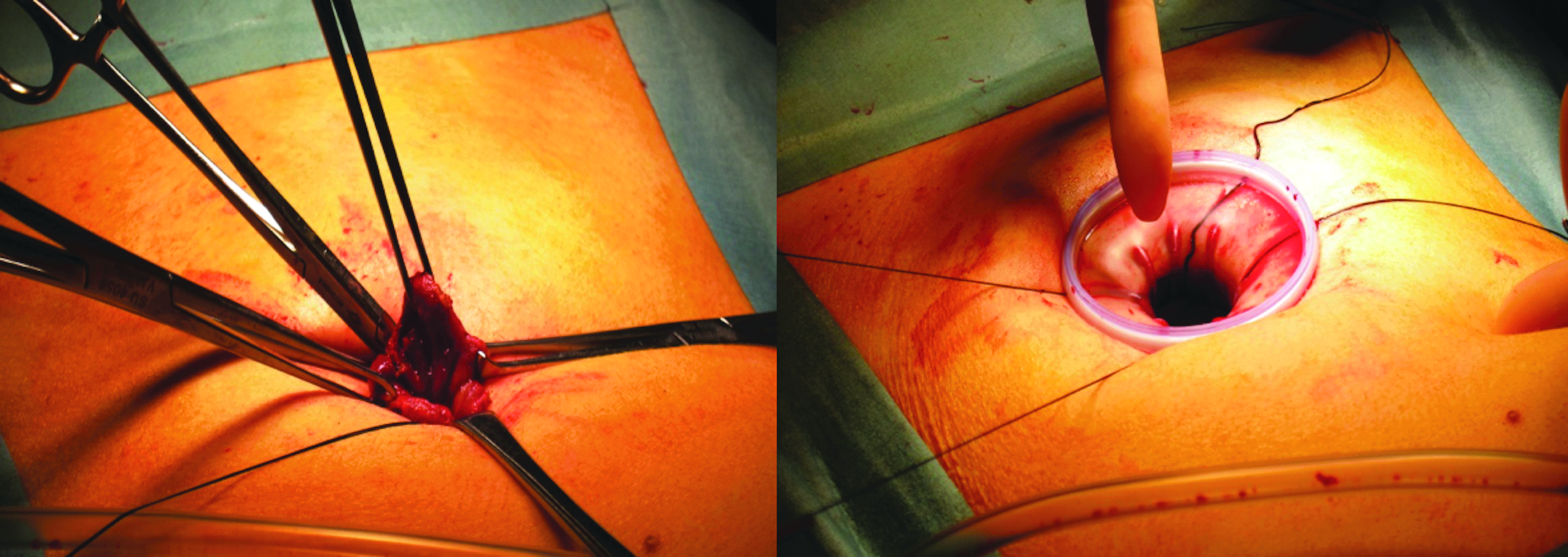
A 3 cm longitudinal incision is made in the umbilical region and protected with a mini-size wound-protecting device (Wrap Protector Mini, 29150150; Hakko, Nagano, Japan).
The initial flexible endoscopy is advanced per orally to identify the gastric lesion and to locate the optimal intragastric access site.
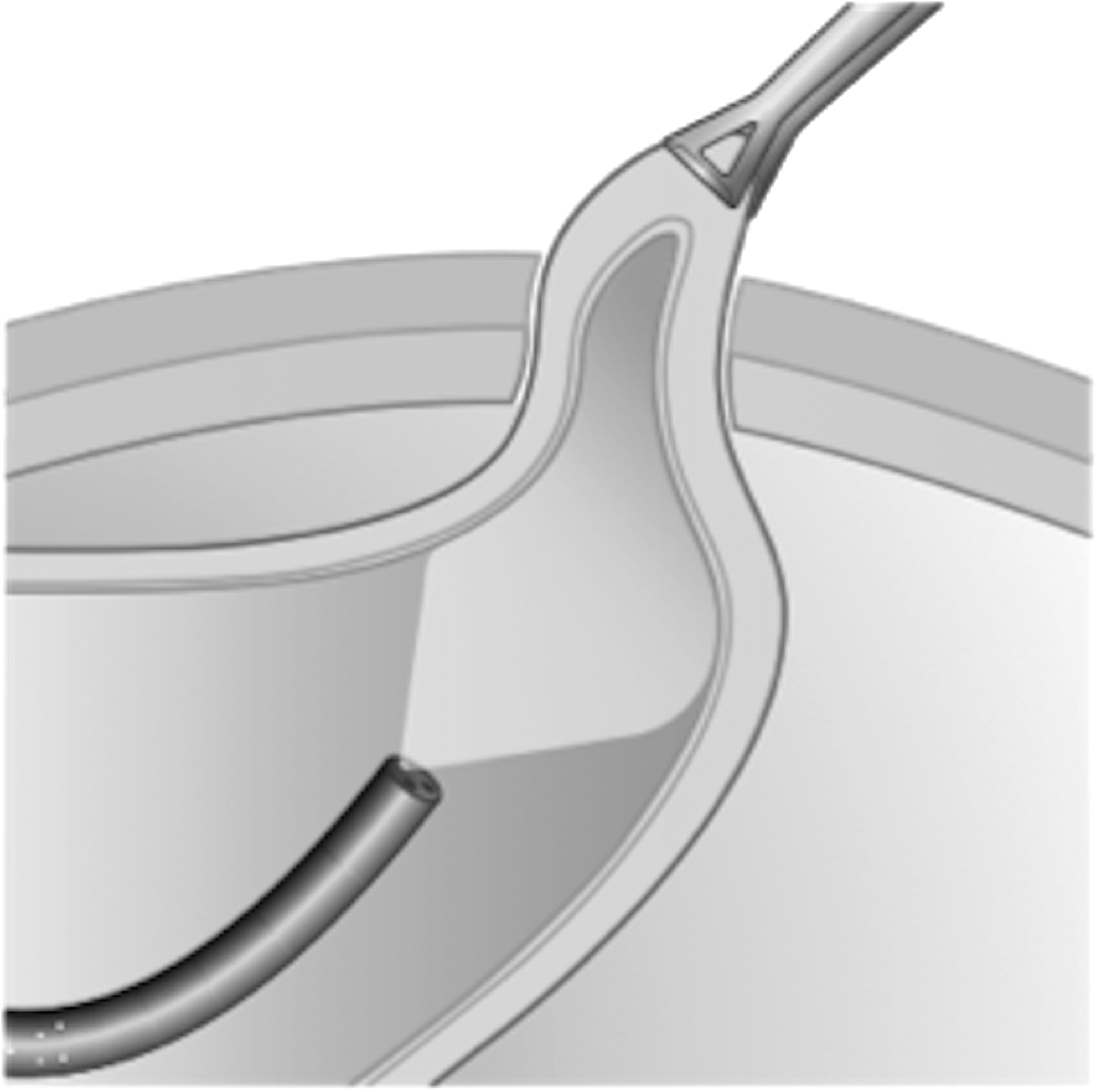
The stomach is insufflated with carbon dioxide using a standard surgical insufflator (UHI-3; Olympus Medical Systems, Tokyo, Japan) up to 8 mmHg to establish pneumogastrium. After evaluating technical feasibility of staple transection with both handed instruments, two 5 mm ports are replaced with one 12 mm port to introduce surgical stapling device with gastrointestinal reload (Endo GIA 45, EGIA45AMT; Medtronic, MN). The tumor is then staple-transected under countertraction provided by an ultrathin loop retracting device (Mini Loop Retractor II, HA0002; Hakko), when indicated. Usually two to three reloads are necessary to complete semi-full thickness gastric resection from the gastric luminal side (Fig. 4). After gastric resection, we do not routinely perform reinforcement of the staple line. In cases with tumors located adjacent to EGJ, resection is initiated from the anal side of the tumor with a stapler, then proceeding toward the oral side close to EGJ. When the stapler is approaching EGJ, a flexible endoscope is used to calibrate the junction, to avoid any damage to EGJ. Before stapling, we ascertain that EGJ is not involved in the stapling site using flexible endoscope.

The tumor is then staple-transected under countertraction provided by an ultrathin loop retracting device (Mini Loop Retractor II, HA0002; Hakko), when indicated. Usually two to three reloads are necessary to complete semi-full thickness gastric resection from the gastric luminal side. The flexible endoscope is passed through the EGJ as calibration, to avoid stenosis due to unexpected involvement of the gastric cardia into the staple line. EGJ, esophagogastric junction.
The resected specimen is isolated into a standard laparoscopic specimen bag (Endo Pouch II, EES-E-043-08; Ethicon-Endo Surgery, OH) and retrieved from the gastrotomy site. The gastrotomy is closed using full-thickness interrupted sutures under direct vision. The conclusion endoscopy and laparoscopy are performed to confirm hemostasis and gastric integrity.
Case Presentation
A 47-year-old man was diagnosed with a gastric SMT in esophagogastroduodenoscopy which revealed a 36 mm tumor with intragastric growth, located 5-mm distal to EGJ. The endoscopic biopsy resulted in poor diagnosis due to small size of the obtained sample. Surgical removal was indicated since gastrointestinal stromal tumor was not ruled out. We offered sLIGS as a surgical alternative. The procedure was performed successfully as described above, and the patient's postoperative course was rapid and uneventful. An immunohistochemical analysis showed positive staining for c-kit, CD34, DOG-1, α-smooth muscle actin (α-SMA), and desmin and negative finding for S-100. The final pathological diagnosis was a leiomyoma, 25 × 15 × 15 mm in diameter, with a mitotic index <20/50 high power fields (HPFs). No recurrence has been noted as of 1 year and 2 months postoperatively (Fig. 5).

A 47-year-old man was diagnosed with a gastric SMT in esophagogastroduodenoscopy and CT revealed a 36 mm tumor with intragastric growth, located 5-mm distal to EGJ. An immunohistochemical analysis showed positive staining for c-kit, CD34, DOG-1, α-SMA, and desmin and negative finding for S-100. The final pathological diagnosis was a leiomyoma, 25 × 15 × 15 mm in diameter, with a mitotic index <20/50 HPFs. CT, computed tomography; EGJ, esophagogastric junction; HPFs, high power fields; α-SMA, α-smooth muscle actin; SMT, submucosal tumor.
Including above case, sLIGS has been performed in 4 patients, and none needed to be converted to open surgery. The median operative time was 149 (range 116–170) minutes and blood loss 30 (0–43) mL. No major perioperative complication was observed except for one case with immediate postoperative bleeding. Emergency flexible endoscopy revealed bleeding on the staple line, which was successfully controlled with endoscopic clips. All cases had no trouble of postoperative wound site (Table 1).
GIST, gastrointestinal stromal tumor.
Discussion
Laparoscopic local resection is the standard surgery for gastric SMTs.1–4 However, the selection of surgical approach depends on tumor size, location, and growth pattern. 5 Especially in cases with SMTs showing intraluminal growth pattern, the identification of the lesion from serosal side is often difficult. As a result, the resection margin might become excessive, resulting in failure of organ integrity preservation. In cases with lesions close to EGJ, local resection might be converted to major surgery such as proximal or total gastrectomy, which can lead to decreased postoperative QOL due to refractory reflux. 17
We first introduced LIGS for cases with early gastric cancer in 1995. 6 As endoscopic submucosal dissection subsequently became widely spread, the clinical significance of LIGS for early gastric cancer has been virtually lost. The authors, however, have reported that LIGS is still a practical surgical option for gastric SMTs, especially cases adjacent to EGJ.7–10 Those lesions could be resected while observing the cardia and lesion from the luminal side, resulting in minimal resection of the gastric wall while preserving the cardia. 11
The original LIGS procedure is “three-port technique,” while this technique has several technical difficulties. One of them is the unstabilized working ports between the abdominal and gastric walls. To prevent this “port escapement” we need to add cumbersome procedure, such as fixing each port by placing sutures and/or using special devices. 6 In sLIGS such port escapement never happens, since all ports are placed through the access device, not through the abdominal/gastric walls. Although this technique is still in a preclinical phase overseas, 19 sLIGS is now clinically performed in Japan by selected institutions with technical modifications. 20
In our technique, we first perform Stamm type gastrostomy. If there is no intra-abdominal adhesion, it is not difficult to lift the gastric wall to the umbilical access port site. And the abdominal and gastric walls were enclosed with a dedicated wound-protecting device. The protecting device is originally designed to protect the abdominal wall, not including the gastric wall. We have not encountered any complications related to the use of this device on the gastric wall, such as mucosal injuries and ischemia. With combined use of wound sealing device, no gas leakage has been experienced in our series.
The optimal traction is another technical issue. In our series we use an ultrathin retracting device to gain countertraction during staple transection. Together with so-called “move-the-ground technique,” we could successfully perform semi-full thickness resection with staplers in all cases. Although careful patient selection is needed, this stapling technique is straightforward and practical for cases with gastric SMTs showing intraluminal growth pattern. There are two technical pointers in this study. First, before the initial stapling, the predetermined staple line is temporarily clamped with bowel graspers, to evaluate whether the stapled resection is indicated for the lesion. Second, unlike laparoscopic local resection, LIGS can be confirmed with the help of intraoperative endoscopy. The tumor is resected in a step-by-step manner under direct vision. This process is further monitored to not to injure the pseudo-capsule of the tumor, not to involve the EGJ, and also to prevent excessive resection. Although surgeons must prepare for manual resection and hand-sewn for difficult cases which are not indicated for stapled resection, 12 the authors believe that sLIGS is a valuable alternative for cases with gastric SMTs adjacent to the EGJ. Further clinical experience is necessary to conclude the true safety and usefulness of this technique.
Conclusions
Single-incision LIGS is a safe, realistic, and potentially effective procedure for gastric SMTs adjacent to the EGJ.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.