
Abstract
Abstract
Laparoscopic cholecystectomy is a common surgical procedure, and remains the gold standard for the management of benign gallbladder and biliary disease. While this procedure can be technically straightforward, it can also represent one of the most challenging operations facing surgeons. This dichotomy of a routine operation performed so commonly that poses such a hidden risk of severe complications, such as bile duct injury, must keep surgeons steadfast in the pursuit of safety. The “difficult gallbladder” requires strict adherence to the Culture of Safety in Cholecystectomy, which promotes safety first and assists surgeons in managing or avoiding difficult operative situations. This review will discuss the management of the difficult gallbladder and propose the use of subtotal fenestrating cholecystectomy as a definitive option during this dangerous situation.
Introduction
C
The “classical” BDI occurs when the common bile duct is mistaken as the cystic duct. Generally occurring in the setting of acute or severe chronic inflammation, the gallbladder may become fused to the lateral wall of the common hepatic duct, and this may predispose the surgeon to misidentify biliary anatomy. This may result in a major BDI in which a segment of the common hepatic and bile duct is removed.7–9 Besides this classical injury, other biliary tree injuries can occur, such as disconnected sectional or segmental ducts of the liver with or without bile leak, bile leakage from the cystic duct stump, late-term strictures from thermal or iatrogenic damage, or combined vasculobiliary injuries. 8
The critical view of safety (CVS), introduced by Strasberg et al. in 1995, is a method of secure ductal (anatomic) identification that serves as a set of criteria to assure adequate identification of appropriate anatomy, which occurs before any ligation of ductal structures. These criteria include separation of the lower end of the gallbladder off of the liver to expose at least the bottom third of the cystic plate, all fibrous and adipose tissues cleared within the hepatocystic triangle, and only two structures are seen to enter the gallbladder.8,10–12 The CVS mimics the secure identification that occurs in traditional open cholecystectomy. 10 While no level 1 data exist to support its use (due to the large sample size required to discriminate between an injury that occurs with a relatively low incidence), there is a body of literature of over 6000 cases where the CVS was achieved without any major BDI.10,11,13–16
While strict adherence to the CVS is important to decrease BDI, it is only one part of the Culture of Safety in Cholecystectomy (COSIC), which mandates safety to be at the forefront. Besides achieving the CVS in cases of total cholecystectomy, COSIC also requires appropriate patient selection and work up, adjustment of surgical technique in the setting of nonroutine cases, use of bailout procedures, and avoidance of complex cases when appropriate experience is not available.10,12,17–19 The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has developed a six-step program to enhance the safety of cholecystectomy that consists of the following: (1) understand the CVS and use it for identification of the cystic duct and artery; (2) consider an intraoperative time out before clipping or cutting any structures; (3) understand aberrant anatomy; (4) liberal use of cholangiography or other means of intraoperative imaging of the biliary tree; (5) recognize when the dissection is approaching a zone of significant risk and finish the operation by a safe method other than cholecystectomy if conditions around the gallbladder are too dangerous; and (6) get help from another surgeon when conditions are difficult. For further details, the reader is referred to www.sages.org/safe-cholecystectomy-program
This review will focus on safely performing LC or an appropriate bailout procedure when difficult situations arise. While the authors generally believe that these procedures can be safely performed through laparoscopy, surgeon experience and comfort must trump method. The general approach and use of bailouts can be performed as an open operation as well.
Preoperative Preparation and Work-Up
Safe performance of cholecystectomy begins with the management, work-up, and selection of appropriate patients. Routine symptomatic cholelithiasis and chronic calculous cholecystitis are common indications for LC. Once a patient appears to be an acceptable surgical risk, specific conditions that suggest a cholecystectomy may be difficult or abnormal need to be investigated (Table 1). Male sex, increased age, and an increased number of “attacks” have been identified as risk factors for severe inflammation and a difficult cholecystectomy. In addition, in the acute setting a marked elevation in white blood cell count (>18,000), suspicion for emphysematous or gangrenous/necrotic cholecystitis, a thickened gallbladder wall, or duration of symptoms lasting more than 72–96 hours typically represent increased operative complexity.20–25
In the chronic setting, a severely contracted or shrunken gallbladder (or a gallbladder than cannot be seen upon cursory exploration) pose significant danger. Morbidly obese or pregnant patients require appropriate adjustments to the surgical technique, port placement, and plan. Patients with cirrhosis or other liver disease may pose difficult and dangerous circumstances. In addition, patients with previous biliary manipulation using transhepatic or endoscopic methods may increase the complexity and difficulty of an otherwise “routine” operation. A high index of suspicion for less common diagnoses such as gallbladder malignancy or Mirizzi syndrome is necessary to appropriately work up and prepare for these unique circumstances. In short, not all cholecystectomies are the same, and the surgeon must be aware of the “nonroutine” to stay one step ahead of danger.
When patients present with confirmed acute calculous cholecystitis, surgeon comfort and timing play a role in the treatment plan. Patients suffering from more than 72–96 hours of symptoms may require nonoperative management due to progression from edematous cholecystitis to fibrous inflammation that may obscure anatomic planes. This nonoperative management may include antibiotics targeted toward normal biliary bacteria, and at times percutaneous cholecystostomy tube placement for gallbladder drainage. In addition, patients presenting with grade 3 severity of acute cholecystitis by the 2013 Tokyo guidelines should preferentially undergo urgent percutaneous decompression if available, with delayed cholecystectomy. 24 Cholecystectomy in patients with grade 2 acute may be difficult and management of these patients should be individualized according to available surgical expertise and the condition of the patient. Management of these patients continues to evolve, as surgeons must balance the risk of BDI and the definitive management of these patients.21,24,26
Operating Room Setup and Preparation
The technical aspects of the operation begin as soon as the patient is scheduled for the operating room. While it is easy to underestimate LC as a basic general surgical procedure, the operation may actually be one of the most difficult challenges unexpectedly facing the general surgeon, and as such, the surgeon should adopt a mindset of “preparing for the worst.” The operation should be performed in a room with an operating table that is capable of fluoroscopic imaging and position changes and in a room large enough to comfortably accommodate a c-arm fluoroscopy unit, even if routine cholangiography is not planned. If routine cholangiography is planned, bringing the c-arm into the operating room as the patient is being prepared avoids issues with having to maneuver such a heavy piece of equipment in a cramped space and minimizes delays and frustration during the operation. In morbidly obese patients, steep reverse Trendelenburg positioning may be necessary to assist in gallbladder visualization, and these patients should be prepared accordingly, potentially utilizing a footboard on a bed capable of extreme positional changes, as well as taking extra care to minimize pressure on extremities.
Access
Standard access for most patients undergoing cholecystectomy is generally done in a periumbilical location. Certain situations call for modifications of this standard technique. In obese patients, the umbilicus will generally migrate to a location lower in the abdomen and placement of the camera trocar at the umbilicus will result in the laparoscopic view being too low and will impair visualization of the gallbladder. The authors generally consider 15 cm caudal from the xiphoid process to be an adequate distance for this camera port. Patients with prior midline laparotomies at the umbilicus are best approached with access at an alternate site such as the left or right upper quadrants. Once access is achieved, lysis of adhesions may be done so as to place working trocars and the camera trocar in a place where the operation may be done comfortably. Correct placement of the additional working trocars will minimize iatrogenic difficulties and should utilize a typical “triangulation” about the gallbladder technique. The placement of additional 5 mm trocars is of little consequence to the patient if it ensures that the surgeon performs the operation comfortably and is not impaired due to poorly placed trocars.
Exposure of the Gallbladder
An angled laparoscope (either 30° or 45°) should be used instead of a straight 0° laparoscope so that the surgeon can better visualize the medial and lateral aspects of the gallbladder dissection, as well as obtain more of a “bird's eye” view of the operative field.
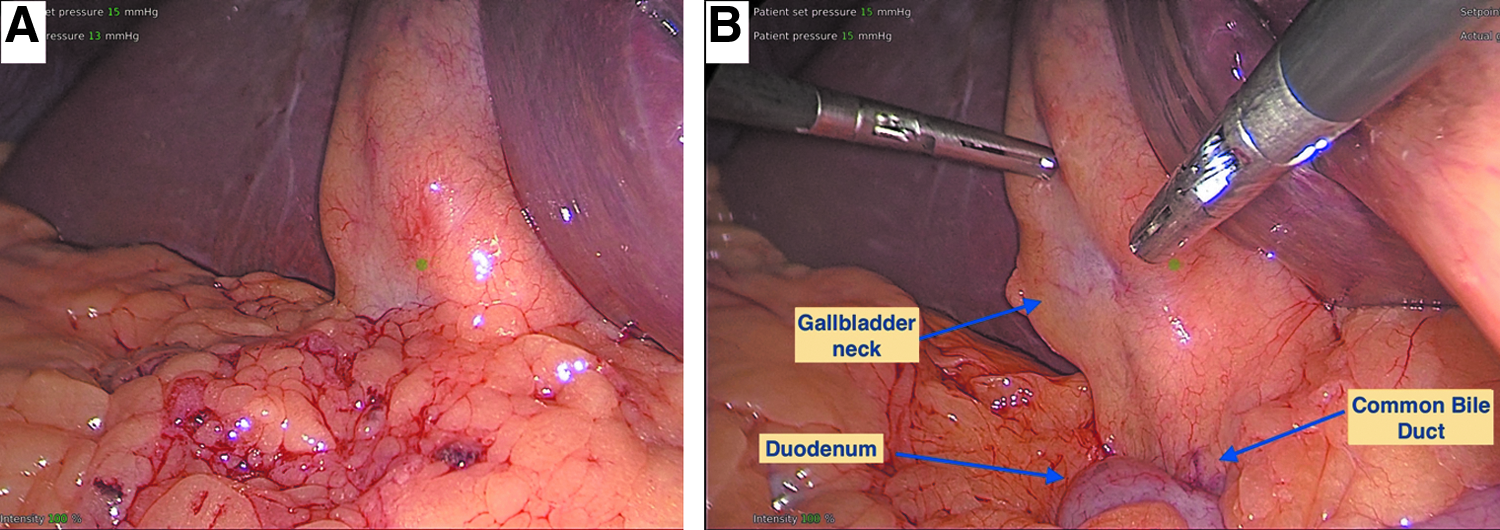
Placement of the patient in a reverse Trendelenburg position with a slight tilt to the patient's left is adequate for exposure of the gallbladder in most patients. However, in patients with significant visceral obesity, the bulk of the greater omentum or transverse colon may sometimes obscure the gallbladder neck and the view of the porta hepatis (Fig. 1). Placing an additional port in the right lower quadrant enables the assistant to help with exposure with another instrument or with a fan-type retractor used to retract the transverse colon and omentum inferiorly (Fig. 1). In cirrhotic patients, or in those with extensive hepatic metastases, the liver may be stiff and may be difficult to retract superiorly, making this additional port useful as well.
Dissection
The technique used for dissection of the gallbladder may seem to be highly variable among surgeons, but must keep common safe principles and be capable of achieving a consistent outcome. In most cases, the initial goal should be achieving the CVS, as this will prevent misidentification injuries.
The dissection begins with taking down any adhesions to the gallbladder with care to avoid injury to the transverse colon or duodenum, which is often in close proximity or adherent to the inflammatory process surrounding the gallbladder. In extreme cases, a cholecystoenteric (either duodenal or colonic) fistula may be present. It is useful to identify the distal stomach or the duodenum at its first portion and follow its course toward the gallbladder to reduce the risk of inadvertently injuring the duodenum. It is during these initial maneuvers that an assessment of the difficulty of the cholecystectomy can be made. Several intraoperative scoring criteria have been described to grade the difficulty of the cholecystectomy. 27
It is worth mentioning that principles of the safe use of surgical energy should be followed during the dissection to reduce the risk of unintentional electrical or thermal injury (www.fusedidactic.org). The electrosurgery (ES) generator should be used with settings according to the size of the patient and according to the task at hand. The potential to create areas of high current density that can lead to unintended injuries should be recognized. This situation can occur, for example, when lysing band-like adhesions between the duodenum and gallbladder using ES. It is also important to note that the common practice of fulguration of the liver bed with ES may place shallow biliary ducts at risk of bile leak postoperatively and should be done judiciously.
Use of advanced energy devices such as an ultrasonic coagulator may help with hemostasis especially in patients with severe acute cholecystitis or cirrhosis, but these devices have their own issues such as thermal spread, which need to be monitored. Careful sharp dissection or blunt dissection with a suction irrigator or Kittner type dissector is encouraged when working around the intestine or bile duct. It is important to note that the CVS will protect against misidentification injuries, but does not protect against unintended electrosurgical or dissection injuries.
The anatomic concept of the hepatocystic triangle is important to remember during dissection. The authors prefer this term to “Calot's triangle,” as the boundaries of this triangle have “changed” over time and the term tends to be less precise than hepatocystic triangle.28,29 The hepatocystic triangle is defined as the triangle formed by the liver bed, the common hepatic duct, and the cystic duct/infundibulum and is where the dissection for the CVS will occur. It is important to retract the gallbladder in a way that causes this triangle to open (Fig. 2), by having the assistant retract the gallbladder fundus superiorly and to the patient's right shoulder, while the surgeon's left hand retracts the infundibulum caudally and laterally. This retraction strategy pulls the lower part of the gallbladder and cystic duct away from the common hepatic duct, opening up the hepatocystic triangle and facilitating dissection of the CVS. In addition, proper retraction minimizes alignment of the common bile duct and cystic duct, minimizing the opportunity for misidentification (Fig. 3).
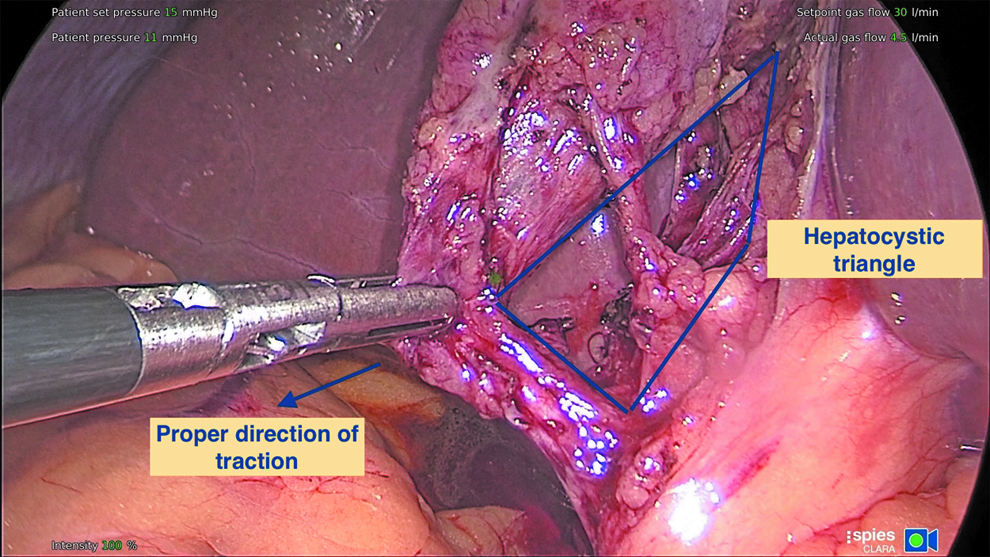
Proper retraction of the gallbladder infundibulum toward the lateral and caudal direction opens the hepatocystic triangle for dissection. Note that the gallbladder has been cleared off the lower third of the cystic plate, and there are only two tubular structures entering the gallbladder (the critical view of safety).
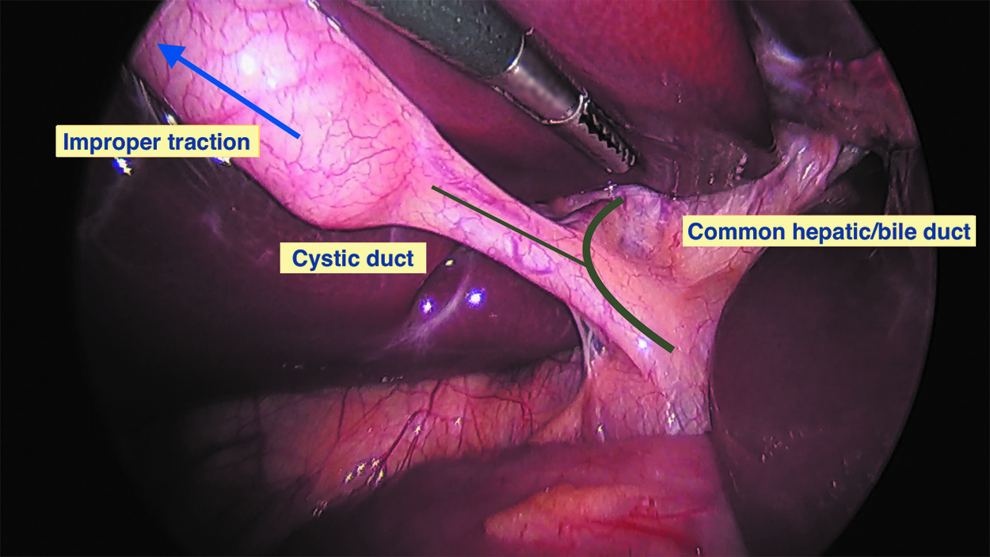
Improper retraction of the gallbladder tents the common hepatic/bile duct upwards, bringing them into alignment with the cystic duct which increases the likelihood of misidentification, especially if dissection occurs “too low.”
As the initial step of the dissection (and a step necessary to achieve the criteria of the CVS), the surgeon should incise the medial and lateral peritoneal attachments of the gallbladder to further open the hepatocystic triangle. This maneuver is effective even in situations where there is severe inflammation of the gallbladder, as it serves to penetrate the tough outer capsule of acute inflammation.
The dissection in the hepatocystic triangle should be done in close proximity to the gallbladder and should also be done anterior (or ventral) to the horizontal plane created by Rouviere's sulcus, a landmark that is frequently encountered as a fissure on the right liver which marks the entry point of the right portal pedicle or its branches 30 (Fig. 4). Staying anterior (or ventral) to the fissure will keep the dissection in a safer location, away from the portal structures.

Dissection in the hepatocystic triangle should be done in close proximity to the gallbladder and anterior (or ventral) to the horizontal plane (dotted line) of Rouviere's sulcus.
The end point of the dissection for a planned total cholecystectomy is achievement of the CVS. It is important to avoid the “infundibular technique” for cystic duct identification, which has been well described as an error trap in situations where the cystic duct has become fused to the common hepatic duct from severe acute inflammation, chronic fibrosis, or an impacted stone in the infundibulum.9,31 In dissecting toward the CVS, the surgeon will gradually isolate tubular structures heading toward the gallbladder, but should resist the temptation to ligate these structures until the full CVS has been achieved or until definitive radiographic confirmation of the anatomy has been made. A frequently neglected component of the CVS is freeing of the lower third of the gallbladder from the cystic plate. 12 This part of the dissection is crucial as it actually facilitates isolation of the cystic duct and artery by further opening up the hepatocystic triangle and is the only way to identify a dangerous anomaly in which the cystic duct drains directly into a variant right hepatic duct (or sectional or segmental duct).
Another frequently mentioned technique for difficult gallbladders is a “top-down” or “dome-down” approach, analogous to open cholecystectomy. While, this may be useful at times, it can make retraction of the liver more difficult as the gallbladder is detached from the liver bed, and also potentially constitutes an error trap, as it may encourage the dissection to drift too close to major biliary and vascular structures as it nears the neck of the gallbladder and porta hepatis. This commonly occurs when the cystic plate contracts and shortens from inflammation and even a short dissection along it can lead the surgeon into the right portal pedicle sheath (which is connected to the cystic plate). This technique has been described in some cases as leading to concurrent vascular and biliary (vasculobiliary) injuries with potentially devastating consequences.31,32
Use of Intraoperative Imaging
Liberal use of intraoperative imaging (cholangiography or ultrasonography), is strongly encouraged to clarify and/or confirm the anatomy in difficult cases before division of the critical structures. There has been significant controversy regarding the utility of routine intraoperative cholangiography (IOC) during LC, with some proponents arguing that it is protective against BDI,33,34 while others have shown no difference in BDI rates.35,36 The best data to help answer this question in the modern era are perhaps from the GallRiks database. 37 Tornqvist et al., in an analysis of 51,041 cholecystectomies from a prospective nationwide database of cholecystectomies in Sweden from 2005 to 2010 analyzed the association of the intention to perform cholecystectomy with rates of BDI. In a multivariate analysis, they found that intention to perform IOC was protective for bile duct injuries in patients with the presence of or a history of previous acute cholecystitis, but not for otherwise routine elective cholecystectomies. In addition to a possible protective effect on the incidence of BDI, these authors also previously have shown that IOC is associated with a higher rate of intraoperative recognition of bile duct injuries, with resultant decreased mortality rates. 38
Performing IOC during difficult cholecystectomies can be challenging, but is often possible with a few technical modifications and is facilitated if the surgeon routinely performs IOC in less difficult cases. When sufficient length on the cystic duct is difficult to achieve, placing a suture tie around the neck of the gallbladder effectively elongates the working length of the cystic duct and allows a ductotomy to be made with enough room to ligate the cystic duct once cholangiography has been completed. Similarly, the surgeon may perform a “cholecystocholangiogram” by placing a needle into the gallbladder lumen and injecting contrast or using the specialized Kumar clamp for this purpose. 39 If the anterior gallbladder wall has been opened, such as during a subtotal “fenestrating” cholecystectomy, a biliary balloon catheter or vessel occlusion balloon catheter can be used to cannulate and occlude the cystic duct orifice from inside the gallbladder while injecting contrast.
A final point on cholangiography is that correct interpretation of the images is as important as the technique used to obtain the images. Failure to properly interpret cholangiography may lead to false reassurance and is an error trap, such as when the surgeon fails to identify lack of filling of right-sided sectional ducts or fails to realize the significance of cholangiography showing only filling of common bile duct. 31 As such, the authors recommend that cholangiography is not considered complete until clear identification of the left hepatic duct, right anterior sectional duct, and right posterior sectional duct (most commonly at risk during LC) is made and may require positioning the patient in Trendelenburg to achieve adequate filling. In addition, visualization of the cystic duct, common hepatic duct, common bile duct, and duodenum is necessary to achieve adequate cholangiography.
Decision-Making and Calling for Help
Surgical decision-making plays the most critical role in cases of the difficult gallbladder and may prove to be the most challenging aspect of the case. 40 The surgeon should be attuned to clues that may indicate difficulty ahead or a current problem. These clues may include: anatomy that appears confusing, lack of progression with dissection, unexplained bleeding or bile leakage, the inability to ligate a tubular structure easily with a standard laparoscopic clip, or the need for an excessive number of clips. 41 The surgeon should not be afraid to call a colleague for help, as this is in fact evidence of good judgment. A colleague can provide an objective external frame of reference, can help the surgeon define the anatomy, can scrub in to provide technical assistance, can make suggestions that may overcome technical challenges, and can help support a decision to convert to an exit strategy rather than proceed with a continued LC if conditions are too unfavorable.
Conversion to open cholecystectomy should always remain a consideration, but should be done for the right reasons. Converting may allow the surgeon to gain better exposure, to control bleeding, to place sutures when doing so laparoscopically would be difficult, and to get a better “feel” for the tissues. However, simply converting to an open operation in difficult situations is often not an adequate “bailout,” as a difficult LC remains a difficult open cholecystectomy. For surgeons without advanced laparoscopic experience, it may be helpful to consult a colleague with advanced laparoscopic training before conversion if possible, as this may decrease overall rates of conversion. 42 If the surgeon nevertheless ends up converting, the help of a colleague with significant open cholecystectomy experience should be sought, as these operations can be extremely challenging and have been shown to be associated with higher rates of BDI than for typical LC. 37
If the surgeon is considering converting to an open procedure due to the perceived inability to achieve the CVS, he/she is recognizing that a dangerous situation exists. This should be commended and is part of the reason the CVS is so effective. And while converting to an open operation is a viable option, other exit strategies exist and should be considered as well.
When and How to Bailout
As stated above, deciding when to halt dissection of the hepatocystic triangle and opt for a “bailout” procedure instead of total cholecystectomy can be challenging. To make this decision before any biliary or vascular injury occurs, the surgeon needs to constantly ask the question “Is it possible to safely achieve the CVS?” When the answer is “No” or “I'm not sure,” we recommend considering a bailout procedure instead. The authors believe early adoption of a bailout procedure will decrease the difficulty of making this decision and prevent inadvertent injury to the biliary tree while trying to dissect in difficult and obliterated planes. It is important to always remember that this operation is done for benign pathology. 40
The authors view three clear surgical options to bailout in the difficult case. The first option is to simply stop the operation. While this option may act in tension to the surgeon's goal of “fixing a problem,” it should be considered and is a viable and safe option to avoid BDI. The patient should be continued on a short course of antibiotics or even sent for percutaneous cholecystostomy tube placement postoperatively. A second attempt at cholecystectomy can be considered in 2–3 months.
Another option when the CVS is not attainable is surgical cholecystostomy tube placement. The gallbladder fundus can be entered after placement of a “purse-string” suture, the contents suctioned, and a drainage catheter brought through the abdomen wall (generally a “mushroom tip” catheter or Foley balloon catheter) is placed into the gallbladder lumen. Again, this method functions as a temporizing measure, as definitive cholecystectomy will likely be required in 2–3 months.
While each of these bailout options are safe alternatives to total cholecystectomy, and a surgeon should be commended for choosing safety before proceeding under dangerous conditions, they generally (although not always) require a second procedure for definitive management. In order for bailout procedures to gain traction, they must be both safe and effective. This is why the authors view the third option, subtotal cholecystectomy (specifically the “fenestrating” subtype), as the most effective bailout for the difficult cholecystectomy.
Subtotal “Fenestrating” Cholecystectomy
Subtotal cholecystectomy has been a surgical option for more than 100 years. Unfortunately during this time, the procedure has not been standardized and even the terminology remained confusing. The now-called subtotal fenestrating cholecystectomy was described, in part, by Estes, Lerner, and McElmoyle and popularized by Bornman and Terblanche for the management of the challenging gallbladder in cirrhotic patients.43–47
In 2016, an attempt at defining subtotal cholecystectomy into two distinct subtypes was made to allow for improved study and dissemination of the technique. In addition, the term “partial cholecystectomy” is discouraged to avoid confusion. The main distinction between the two subtypes of subtotal cholecystectomy hinges on whether a remnant “neo” gallbladder is created as part of the procedure. When a new, smaller gallbladder remnant is created this is termed subtotal “reconstituting” cholecystectomy. When the gallbladder is left open with a portion remaining, this is termed subtotal “fenestrating” cholecystectomy. 44 Recent systematic reviews demonstrated the safety of these procedures.48,49 While it remains unclear which subtype is the best option for the difficult gallbladder, the authors recommend fenestrating subtotal cholecystectomy as the most definitive bailout procedure. In cases where the gallbladder is “reconstituted” there remains a risk for recurrent stone formation and, at times, the need for a second and more difficult “completion cholecystectomy.”
Once the decision is made to proceed with subtotal fenestrating cholecystectomy, the surgeon should consider his/her expertise and whether to convert to an open procedure or continue laparoscopically. We believe this procedure can be safely performed laparoscopically with minimal “advanced” laparoscopic maneuvers; however, it can also be performed easily using an open technique.
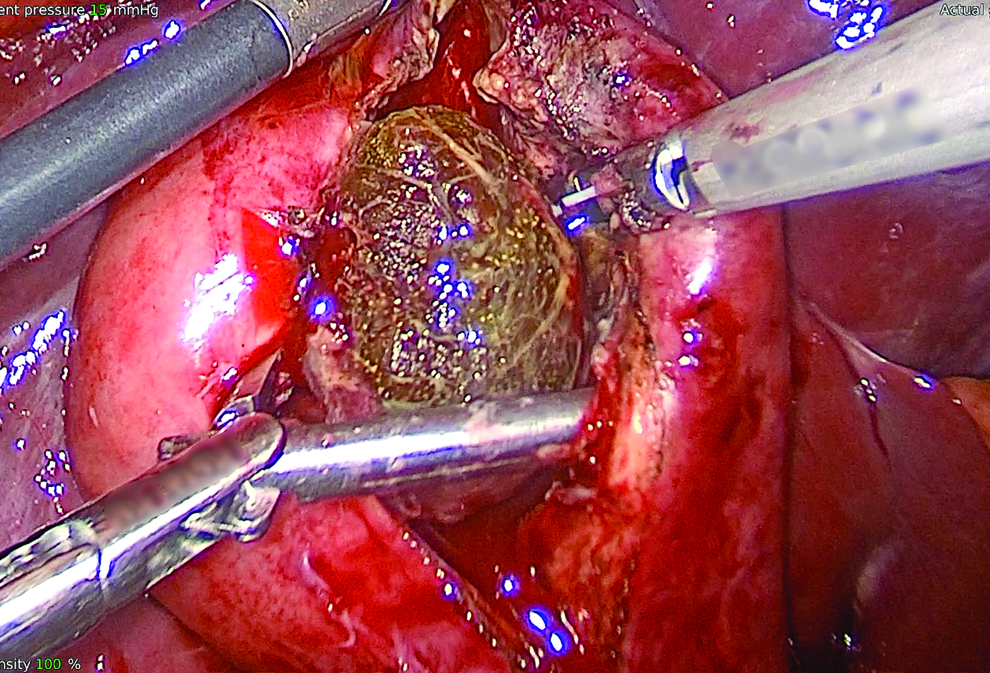
The first step involves incision of the anterior (peritonealized) wall of the gallbladder in the fundus. By leaving the body of the gallbladder intact at first, the contents of the gallbladder can be evacuated more easily. It may be first advisable to place a surgical sponge or “endobag” underneath the gallbladder to facilitate capture of any stones that would be spilled from opening it (Fig. 5). The incision should be continued down toward the infundibulum, removing the majority of the anterior wall of the gallbladder. A very important consideration of this technique involves leaving a portion of the anterior wall of the infundibulum intact to avoid inadvertent entry into the hepatoduodenal ligament (Shield of McElmoyle). 46 Once the majority of the anterior wall is removed and the contents of the gallbladder, including all stones, are evacuated, the inner aspect of the gallbladder can be examined. It is important to identify whether or not there appears to be continuous bilious drainage from the gallbladder (Fig. 6). It is our experience that in the majority of “difficult” gallbladders that require subtotal fenestrating cholecystectomy, the cystic duct is obliterated and does not require formal ligation. However, in the rare instances where the duct is patent and bile continues to drain from it, the internal orifice of the cystic duct should be closed with nonpermanent suture from the internal aspect of the gallbladder. At no point should an attempt at external ligation of the cystic duct occur which could potentially injure the bile duct. A drain should be left in the hepatorenal recess. No drain is necessary within the lumen of the gallbladder. The drain should be monitored for bilious drainage. While generally a rare occurrence, if bile fistula occurs postoperatively, then standard management should proceed. We do not recommend routine postoperative endoscopic sphincterotomy, unless a bile fistula is persistent, as the majority of these are self-limiting.
The initial step of subtotal fenestrating cholecystectomy is to open the anterior wall of the gallbladder and evacuate all stones.
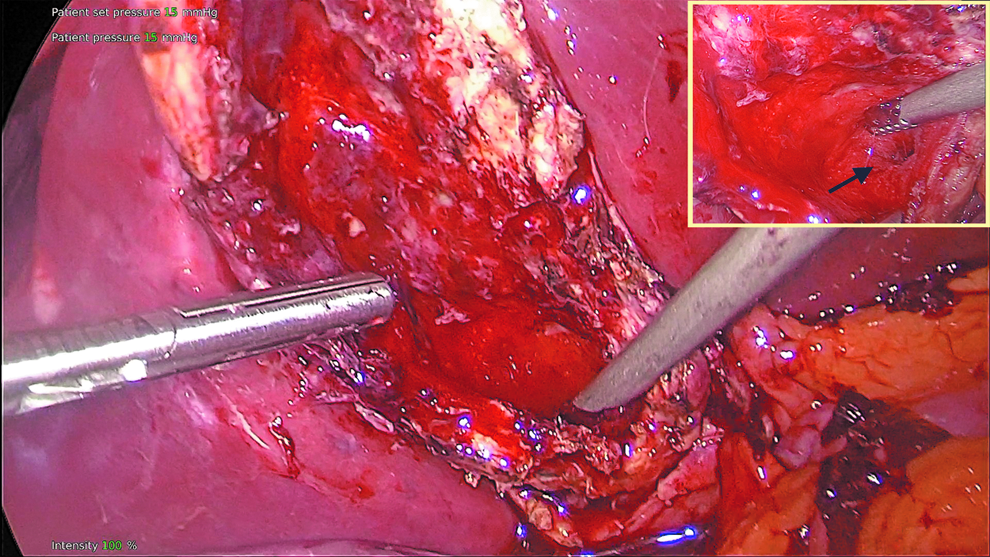
The anterior wall of the gallbladder is excised, leaving the posterior wall intact. The cystic duct orifice (arrow, inset photo) is identified from within the gallbladder and may be sutured closed from inside the gallbladder, if necessary.
Conclusion
The primary goal of LC is “safety first, total cholecystectomy second.” While the majority of laparoscopic cholecystectomies performed will be straightforward, the surgeon should always keep this culture of safety at the forefront and remain vigilant to stay ahead of dangerous situations. The COSIC will help minimize (or eliminate) BDI and will assist the surgeon in managing difficult operative conditions or clinical scenarios. Safe management of the difficult gallbladder is possible with operative adjustments and liberal use of bailout procedures, specifically subtotal fenestrating cholecystectomy.
Footnotes
Acknowledgments
The authors would like to thank the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) for its continued effort to disseminate educational resources to help improve the safety of our patients. In addition, the authors thank the leaders and members of the SAGES Safe Cholecystectomy Task Force for helping to create a Culture of Safety in Cholecystectomy and being champions of patient safety.
Disclosure Statement
No competing financial interests exist.