
Abstract
Abstract
Introduction:
Nontechnical skills (NTS) such as teamwork and communication play an important role in preventing adverse outcomes in the operating room (OR). Simulation-based OR team training focused on these skills provides an environment where team members can learn with and from one another. We sought to conduct a systematic review to identify simulation-based approaches to NTS training for surgical teams.
Materials and Methods:
We conducted a systematic search of PubMed, ERIC, and the Cochrane Database using keywords and MeSH terms for studies describing simulation-based training for OR teams, including members from surgery, anesthesia, and nursing in September 2016. Information on the simulations, participants, and NTS assessments were abstracted from the articles meeting our search criteria.
Results:
We identified 10 published articles describing simulation-based OR team-training programs focused on NTS. The primary focus of these programs was on communication, teamwork, leadership, and situation awareness. Only four of the programs used a validated instrument to assess the NTS of the individuals or teams participating in the simulations.
Discussion:
Simulation-based OR team-training programs provide opportunities for NTS development and reflection by participants. Future programs could benefit from involving the full range of disciplines and professions that compose an OR team, as well as increased use of validated assessment instruments.
Introduction
N
Simulation-based training has been widely adopted by medical and health professional programs for teaching technical skills. 4 By providing an environment that can be used for training NTS, it provides a safe place where clinicians are able to receive instruction and develop their skills without risk to patients. Many disciplines, including anesthesia 5 and obstetrics, 6 have used simulation-based training programs to teach communication and teamwork skills to create safer care and reduce malpractice claims. Participants in these programs frequently come from a single discipline or profession, with the other roles being played by actors in confederate roles.
Teams that work together have been called upon by the US Institute of Medicine to train together to fully understand the strengths and weakness of each member's discipline and training. 7 While simulation-based training for a single discipline may provide opportunities for education and development, interprofessional simulation-based team training allows learners from all involved disciplines to engage in the deliberate practice of team and communication skills with individuals from the professions that they work with on a day-to-day basis in the OR. 8
Previous reviews of OR team-training programs have focused either on the acceptability of such programs 8 or have included studies that did not include all three major disciplines involved in surgery. 9 To determine the current state of surgical team training in NTS, we conducted a systematic review of the literature regarding interprofessional OR team simulation training programs that include members of all three major professional groups (surgeons, anesthesiologists, and nurses). We also sought to identify the assessment tools used in these programs.
Materials and Methods
Search strategy
We searched PubMed, ERIC, and Cochrane for all original research studies describing simulation-based NTS team training for OR teams published between January 1, 2000 and September 1, 2016. The search was performed using the following relevant keywords and MeSH terms: interprofessional, interdisciplinary, NTS, communication, surgery, OR, surgical team, teamwork, and simulation. The reference lists of identified articles were hand-searched for additional publications that might have been missed in the search.
Titles and abstracts of all identified articles were read to determine whether the article fit the objectives of the review. Full text of articles that appeared to be relevant was reviewed to determine whether the articles met the inclusion criteria.
Inclusion and exclusion criteria
Articles were included if they were written or translated into English, published in a peer-reviewed journal or other peer-reviewed periodical, contained a simulation component, had activities or assessments related to NTS, and included at least one team member from surgery, anesthesia, and nursing as part of the training team. Surgery participants could include students, residents, fellows, or attending surgeons. Anesthesia participants could include either physician anesthesiologists or nurse anesthetists at the student, trainee, or practitioner level. Nursing participants could include circulating nurses or scrub technician at either the student or practitioner level.
Articles were excluded if they did not include a member from each of the disciplines, if a discipline was only included in a planned confederate (actor) role, or if the training focused solely on technical skills.
Data extraction
Two independent reviewers assessed and abstracted information from each of the articles using a predefined data abstraction form. Data regarding the following factors were obtained from each of the articles: first author, publication date, study method, participant characteristic, assessment methods, and major findings. Any points of disagreement were discussed until a consensus was reached. A third reviewer was available if any discrepancies in data extraction could not be reconciled.
Results
A total of 232 studies were identified during the initial search. After abstract review, 19 studies were included as potentially being relevant to the questions. After final review, abstraction, and consensus, nine articles met the inclusion criteria. One additional article was found by hand-searching the reference lists of full-text articles. Thus, a total of 10 studies were identified for inclusion in the review (Fig. 1).10–19
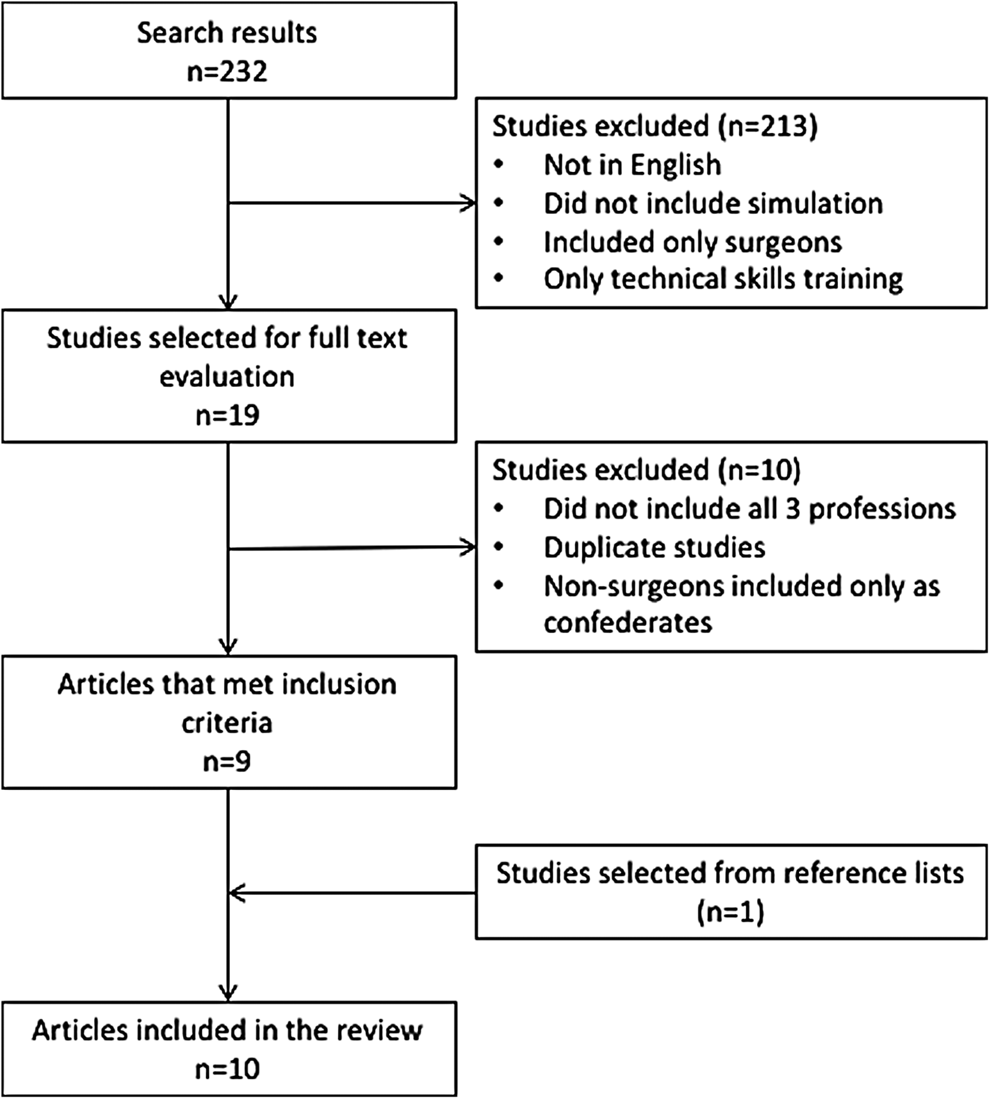
Review process flow and article inclusion and exclusion.
Setting
Single-institutional programs comprised nine10–18 of the ten included studies, with the other 19 conducted at four different sites. Four studies utilized simulation centers for the training,13–15,18 three studies used in situ simulation10,12,16 and one study used a combination of both in situ and simulation center-based training. 17 The study 19 that occurred at multiple sites had three sites that utilized simulation centers and one that utilized in situ simulation. In one 11 study, the location of the training was unclear (Table 1).
CRNAs, certified registered nurse anesthetists; HCA, healthcare assistant; ODP, operating department practitioner; OR, operating room.
Eight studies were in general surgery. 19 Two studies were in surgical subspecialties, one each in cardiac surgery 13 and otolaryngology. 10
Participant characteristics
Surgery
Of the 10 programs included in this review, seven10–12,14,15,17,18 were designed specifically for surgical trainees. Two described programs that involved both surgical trainees and attending surgeons.16,19 A single study included only attending surgeons. 13
Surgical trainees were described as being senior level residents and fellows in four programs.10,14–16 One study focused on junior surgical residents. 17 In three of the studies, the level of the participating residents was not noted.11,12,18
Anesthesia
Participants from anesthesiology varied among physician anesthesiologists at the resident, fellow, and attending level and certified registered nurse anesthetists (CRNAs) at the practitioner and student level. Five studies11,12,14,17,18 involved physician anesthesia trainees at the resident and/or fellow level. A single study 10 used both physician anesthesia trainees and CRNAs as the participants. One study15,16 used only practicing CRNAs, and another study 15 used both practicing and student CRNAs. Attending anesthesiologists were the sole participants in a single study. 13 A final study involved both attending anesthesiologists and practicing CRNAs. 19 Two studies involved attending physician anesthesiologists, one in conjunction with CRNAs. In addition to the main anesthesia role, two studies13,18 also included specific anesthesia nurses as participants.
Nursing
Three studies12,16,19 included both circulating nurses and scrub practitioners in the scenarios. Four studies included11,13,14,18 had scrub practitioners as the only nursing participants in the scenario, and three studies10,15,17 had circulating nurses as the only nurse participants in the scenario. A single study 17 utilized both practicing and student nurses as participants in the scenarios.
Other OR team members
Five11,13,14,17,19 of the identified studies included additional members of the OR team. One study 13 included perfusionists as additional members of the surgical team during the scenarios. Another study 17 included team members from pharmacy, critical care, emergency medicine, respiratory therapy, and cardiology as part of a larger simulation with surgical residents that took place across several simulated locations, including the OR. Two studies11,14 included operating department practitioners (ODPs), and one study 11 also included healthcare assistants (HCAs) in the simulation. One study 19 included surgical physician assistants, biomedical engineers, and other nonidentified team members.
Curricula
The described programs included between one and four scenarios for each of the OR teams. Four of the programs12,14,15,17 used one training scenario, one program 13 used two training scenarios, three programs10,11,19 used three training scenarios, and one program 18 used four training scenarios. In one program, 16 the number of training scenarios varied by OR team. In addition to the scenarios and debriefing, four of the team-training programs10,11,13,19 also included a didactic teaching component.
Nine10–17,19 of the included articles described the focus of the postscenario debriefing. Communication,10,11,15,17,19 teamwork,11,13,15–17 leadership,10,11 and situational awareness11,15,17 were most common themes among the targeted behaviors for debriefing. Fixation, 10 reflective practice, 16 speaking up,10,19 problem solving, 17 decision-making, 11 use of the surgical checklist, 19 and transfer of knowledge to clinical practice 16 were also mentioned as the focus of the debriefing sessions, although less frequently.
The OR team-training programs ranged from a 3-hour course to a full-day training session. Four10,13,14,19 were half-day training programs, and two11,18 were full-day courses. Another two programs15,16 were 3 hours in length. In two programs,12,17 the description did not include the length of the training.
Evaluation and assessment
NTS assessment
Six10,13,15,16,18,19 of the ten included programs did not use any NTS assessment for the teams or participants. Four11,12,14,17 studies used a validated instrument for assessing the NTS of participants. In three11,14,17 of these studies the programs used a modified version of NOTECHS 20 (Table 2). A single study 12 used separate rating scales for the participating scrub practitioners (SPLINTS), 21 anesthesiologists, (ANTS) 22 and surgeons (NOTSS) 23 as well as an overall teamwork assessment scale (OTAS). 24
NTS, nontechnical skills; PETQ, Participant Evaluation of Training Questionnaire.
Technical skill assessment
In addition to the NTS focus during the training sessions, two studies12,14 also included assessments of technical skills. Specifically, one study 12 used a checklist with the steps for managing malignant hyperthermia, and another 14 used several validated instruments for assessing the technical skills of the surgeons (OSATS) and nurses (ICATS-N), as well as detailed notes of the technical skills of anesthesiologists and ODPs for feedback and coaching.
Course evaluation
Nine10,11,13–19 of the ten included studies described the use of a course evaluation completed by participants on the content, structure, and overall impact of the material. In one of these studies, 14 the program used a modified version of the validated Participant Evaluation of Training Questionnaire (PETQ) 25 at the end of the session. Several of the studies also included other measures of success as part of the training program. One course 11 measured attitudes and learning related to the course, both immediately following the training session at 6 months after training. Another course 13 conducted an OR teamwork climate survey both before and 6 months after their team-training intervention to assess the impact of the program on the OR climate. Two studies16,18 measured pre- and post-training self-efficacy related to used NTS in the OR.
Discussion
This systematic review identified 10 unique reports of simulation-based OR team-training programs focused on the NTS of surgeons, anesthesiologists, and nurses. Overall, the educational programs described in these articles focused heavily on the teamwork and communication between members of the different disciplines participating in the simulation trainings.
Given the popularity of simulation-based training, one might expect more reports of interdisciplinary surgical team training. There are many more reports in the literature of single disciplines or two disciplines working together. This is not an uncommon training model as there are fewer barriers to include only two of the disciplines, including cost, time, and departmental buy-in. While these programs provide an important training opportunity for individuals from different disciplines or professions to work together, they leave other essential team members. Whole-team communication failures can lead to errors and threats to patient safety; therefore, whole surgical team simulations targeting NTS, as well as change OR culture around communication and teamwork, may improve patient care and assist teams in creating shared mental models with the OR.
While several validated instruments exist for objectively measuring the NTS of individuals21–23 as well as OR teams, 20 only four11,12,14,17 of the programs included in this review made use of these instruments for assessment of participants. These tools can be helpful for guiding discussions and debriefing, coaching participants toward improvement, and tracking improvements of participants over time.
As reporting of outcomes from these studies is not standardized and is largely based on responses to postcourse evaluations or various assessments conducted by the facilitators, it was not possible to perform a meta-analysis. To gain a better understanding of the variability and extent of the simulation-based OR team-training programs being conducted, we chose to include all reports, regardless of the quality of the research or reporting. Possible future research into the development of standardized instruments for assessing OR team training would be beneficial to enable comparison of different educational programs. Presumably, a number of groups are running similar programs but have not published their educational program.
To our knowledge, this is the first review to look at NTSs in interprofessional OR team training where all three disciplines were represented. Given the continued rise of such programs, it is likely that other programs will continue to develop. While many similarities between the training programs exist, each of the developed programs has unique elements that may influence the resulting knowledge and ultimately behavior changes that occur as a result of the training. Standardized outcomes would allow for comparison between programs and identification of the hallmarks of a successful OR team-training program that can be shared and adopted by departments and centers looking to create a program to increase communication and teamwork among OR teams and improve patient safety.
Footnotes
Disclosure Statement
No competing financial interests exist.