
Abstract
Abstract
Background:
Since the development of the uniportal video-assisted thoracoscopic surgery (VATS) technique, the use of uniportal VATS has become increasingly popular for the surgical resection of non-small cell lung cancer (NSCLC). The objective of this study is to introduce a novel modularly designed surgical pattern for uniportal VATS for lung cancer resection and to investigate the safety, feasibility, and efficacy of this novel method.
Materials and Methods:
The clinical data of NSCLC patients who underwent a curative uniportal VATS lobectomy between March 2015 and April 2016, including via the modular pattern (MP) and the conventional pattern (CP), were retrospectively collected and analyzed. Perioperative and postoperative parameters, including the operation duration, estimated intraoperative blood loss, rate of conversion to thoracotomy, lymph node dissection number, and postoperative complications, were compared between the two groups.
Results:
A total of 321 patients were identified, among whom 221 underwent MP uniportal VATS lobectomy and 100 were treated via CP uniportal VATS lobectomy. Patients in the MP group experienced a shorter operation duration (135.58 ± 47.16 minutes versus 148.86 ± 42.53 minutes, P = .017) and less estimated intraoperative blood loss (75.20 ± 37.99 mL versus 89.50 ± 41.11 mL, P = .003) than patients in the CP group. No significant difference was observed in the intraoperative conversion rate (2.7% versus 5.0%, P = .477), total number of lymph nodes dissected (24.67 ± 7.73 versus 25.34 ± 7.62, P = .471), postoperative drainage duration (4.86 ± 1.96 days versus 4.78 ± 2.10 days, P = .755), length of stay (9.60 ± 2.93 days versus 9.97 ± 2.80 days, P = .286), or incidence of postoperative complications between the two groups. No postoperative deaths occurred.
Conclusions:
MP uniportal VATS lobectomy combined with mediastinal lymphadenectomy appears to be a safe and feasible technique for the treatment of NSCLC. The use of this technique can reduce the operation duration and intraoperative blood loss.
Introduction
D
Materials and Methods
This study was approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. All clinical data were retrieved from NSCLC patients who underwent a curative uniportal VATS lobectomy in the Department of Thoracic Surgery, Tongji Hospital, between March 2015 and April 2016. The surgeries were performed by three senior surgeons who were experienced in uniportal VATS.
The demographic characteristics and preoperative data, including smoking history, comorbidities, pulmonary function results, and clinical staging information, were reviewed. In all cases, preoperative assessments included a physical examination, blood assay, electrocardiography, pulmonary function tests, a computed tomography (CT) scan of the chest and upper abdomen, a magnetic resonance imaging scan of the brain, and a whole-body bone scan. Whole-body positron emission tomography-CT was applied, if necessary. CT-guided biopsy or endobronchial ultrasound transbronchial needle aspiration was performed to obtain the preoperative histologic diagnosis, when indicated.
The inclusion criteria were as follows: (1) primary NSCLC patients with a solitary pulmonary lesion, (2) surgical procedures including lobectomy and systematic lymph node dissection, and (3) an American Society of Anesthesiologist score of I–II.
The exclusion criteria were as follows: (1) patients with a history of cancer or neo-adjuvant therapy, (2) patients with a history of trauma or chest surgery, or (3) extensive pleural adhesions explored during the operation.
Surgical technique
All patients received combined general intravenous and inhalation anesthesia and were intubated with a dual lumen endotracheal tube to accomplish single-lung ventilation. The vital signs of patients were monitored during the operation. Patients were placed in a full lateral decubitus position with a folding knife flexion, which allowed for a widening of the intercostal space. The operator and the assistant stood on the abdominal side of the patient, and the camera holder stood on the dorsal side. A 3.0-cm incision was made at the fifth intercostal space on the anterior axillary line, except for right middle lobectomy cases. In the case of middle lobe resection, an incision was made at the sixth intercostal space to obtain a better angle to pass the staples through the vessels.
In the case of patients without preoperative definitive evidence of malignancy, after an initial exploration, if wedge resection of the lesion was possible, a wedge resection was performed followed by an intraoperative frozen section examination to determine the pathological diagnosis. If the lesion could not be removed by wedge resection, a frozen section examination was performed after the target lobe was retrieved. Systemic lymph node dissection was performed on all patients with a diagnosis of malignant tumor. Anatomic dissection was mainly performed in a sharp manner with an endoscopic electrocautery hook throughout the surgery rather than in a blunt manner. The vessels and bronchus were stapled with endoscopic staplers with a flexible tip. At the end of the operation, two chest tubes (16F) were inserted through the incision and placed along the anterior and posterior mediastinal plane, respectively. After the confirmation of lung re-expansion with a postoperative chest X-ray, the tubes were removed if no air leakage was observed and the drainage volume was <150 mL per 24 hour.
Conventional uniportal VATS for lung cancer is a classic technique, as described by Murakawa et al., 10 and has been our standard approach since 2014. A lobectomy is first performed and followed by systemic mediastinal lymph node dissection. During the period from March to September 2015, all patients underwent CP uniportal VATS in our department. Since October 2015, the conventional technique was changed to the MP uniportal VATS technique, which performed the dissection of the mediastinal lymph nodes first, and then lobectomy. The entire procedure was decomposed into five consecutive modules. The bilateral thoracic cavity exhibits asymmetrical anatomical characteristics; the modules of left- and right-sided surgery are shown in Figure 1 and described in detail as follows.
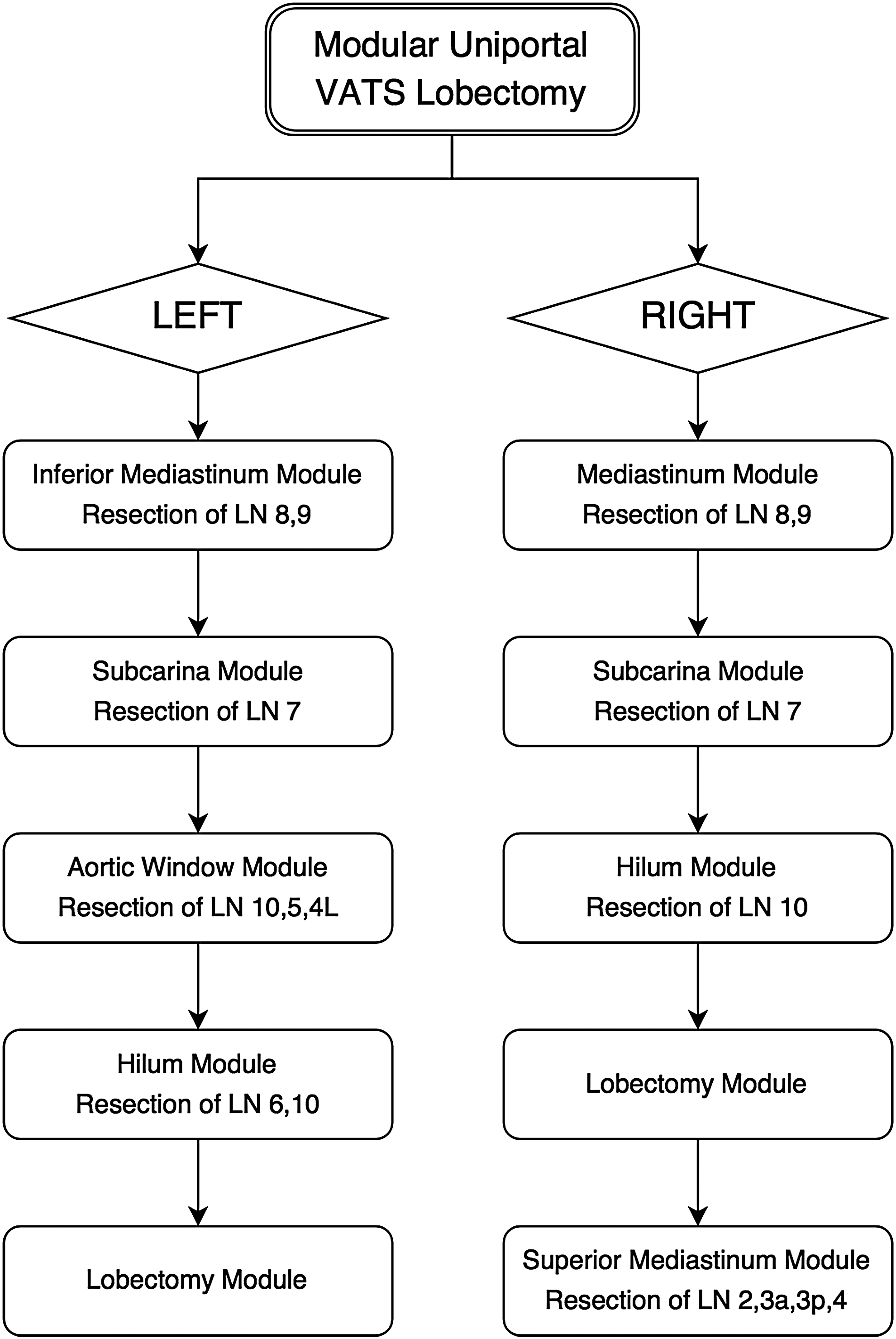
Modules of bilateral modular uniportal VATS for lung cancer. LN, lymph node; VATS, video-assisted thoracoscopic surgery.
MP of left-sided surgery: (1) The lower lobe is retracted in a cephalad direction, and the inferior pulmonary ligament is divided; the No. 8 and 9 lymph nodes are excised; (2) the dorsal segment is retracted anteriorly, and the operation bed is rotated anteriorly; the vagus nerve is dissected along the stem to expose the esophagus, pericardium, and bilateral main bronchus; then, the subcarinal lymph nodes are excised; (3) the apico-posterior segment of the upper lobe is grasped and moved toward the anterior-inferior direction; dissection is performed along the vagus nerve stem to the aortic arch; the left recurrent laryngeal nerve (RLN) is exposed; then the posterior hilar lymph nodes and the No. 5 and 4L lymph nodes are excised successively; (4) the anterior segment is retracted posteriorly while rotating the bed backward, and after the phrenic nerve and anterior hilum are clearly exposed, the anterior hilar lymph nodes and the No. 6 lymph nodes are excised; and (5) an anatomical lobectomy is performed.
MP of right-sided surgery: (1) The inferior pulmonary ligament is dissected; the No. 8 and 9 lymph nodes are excised; (2) the dorsal segments are retracted anteriorly, and the operation bed is rotated anteriorly; the vagus nerve stem is dissected to expose the esophagus, pericardium, and bilateral main bronchus; the subcarinal lymph nodes are excised; (3) the posterior and anterior hilar lymph nodes are excised; (4) an anatomical lobectomy is performed; and (5) the head of the bed is elevated to ∼30° in Fowler's position. The lobe is retracted caudally, and the 3a and 3p lymph nodes are resected; the 2R and 4R lymph nodes are resected en bloc with the attached adipose tissue, which is located in a triangular area among the superior vena cava, the arch of the azygos vein, and the trachea.
Statistical analysis
The statistical analysis was performed with SPSS 19.0 (IBM Corp., Armonk, NY). Continuous variables are presented as means ± standard deviation. A two-sample t test or Fisher's exact test was used to compare the variables between the two groups. Categorical variables were compared by Pearson's χ2 test. P values of <.05 indicate statistically significant differences throughout the study.
Results
A total of 321 NSCLC patients who underwent curative uniportal VATS lobectomy in Tongji Hospital from March 2015 to April 2016 were identified. Among these patients, 221 received an MP uniportal VATS lobectomy (68.8%), and 100 received a CP uniportal VATS lobectomy (31.2%). The comparisons of patient demographics and clinical tumor characteristics of the two groups are shown in Table 1. Among the two groups, no differences in age (P = .121), gender distribution (P = .578), body mass index (BMI) (P = .971), smoking history (P = .286), forced expiratory volume in 1 second (FEV1) (P = .205), comorbidities, location (P = .361), or size (P = .276) of the tumor were observed.
Continuous variables are presented as the means ± standard deviation, and categorical variables are presented as numbers (%).
BMI, body mass index; COPD, chronic obstructive pulmonary disease; CP, conventional pattern; FEV1, forced expiratory volume in 1 second; MP, modular pattern.
The perioperative outcomes of the two groups are shown in Table 2. All anatomical lobectomies were performed with a similar distribution between the two groups. The operation duration was shorter in the MP group than in the CP group (135.58 ± 47.16 minutes versus 148.86 ± 42.53 minutes, P = .017), and the estimated intraoperative blood loss was significantly lower in the MP group than in the CP group (75.20 ± 37.99 mL versus 89.50 ± 41.11 mL, P = .003). We also analyzed the effect of several clinical variables, including age, gender, BMI, FEV1, laterality, tumor size, and N-stage, on the operative time and blood loss volume between the two groups (Table 3). Both operative time and intraoperative blood loss were significantly lower in the MP group among patients who were younger than 60 years old (P = .008, P = .027), had a BMI of < 25 (P = .027, P = .000), or had an FEV1 of >2.0 (P = .017, P = .002). Moreover, compared with the CP group, the intraoperative blood loss in the MP group was much lower in the following subgroups of patients: patients who were older than 60 years (P = .047), female patients (P = .006), patients who received a right-sided lobectomy (P = .001), patients with a tumor size of ≤3.0 cm (P = .002), or patients with negative lymph nodes (P = .003). In contrast, no difference in operative time was found between the two groups for the subgroups of the variables listed earlier.
Continuous variables are presented as the means ± standard deviation, and categorical variables are presented as numbers (%).
CP, conventional pattern; LLL, left lower lobectomy; LOS, length of stay; LUL, left upper lobectomy; ML, middle lobectomy; MP, modular pattern; RLL, right lower lobectomy; RLN, recurrent laryngeal nerve; RUL, right upper lobectomy.
Continuous variables are presented as the means ± standard deviation.
BMI, body mass index; CP, conventional pattern; FEV1, forced expiratory volume in 1 second; MP, modular pattern.
Six patients (2.7%) were converted to thoracotomy in the MP group: 2 conversions were caused by intraoperative hemorrhage, 3 conversions were due to the presence of a calcified lymph node with dense adhesions to the pulmonary artery, and 1 conversion occurred because oxygenation could not be maintained by single-lung ventilation. Among the CP group, 5 patients (5.0%) were converted to open thoracotomy, 3 were converted due to intraoperative hemorrhage, and the other 2 were converted because the calcified lymph nodes had adhered to the artery. The conversion rate in the CP group was higher than in the MP group, but the rates were not significantly different (P = .477). RLN injury was regarded as a critical secondary injury due to intraoperative manipulation. In the cohort, RLN injury was exclusively observed in patients who underwent left-sided lobectomy and lymphadenectomy. The MP uniportal VATS group exhibited a slightly lower incidence of RLN injury than the CP group, but no significant difference was detected (6.0% versus 8.9%, P = .794). Moreover, the total number of dissected lymph nodes (24.67 ± 7.73 versus 25.34 ± 7.62, P = .471), postoperative drainage duration (4.86 ± 1.96 days versus 4.78 ± 2.10 days, P = .755), length of stay (9.60 ± 2.93 days versus 9.97 ± 2.80 days, P = .286), and incidence of complications between the two groups were similar, and no significant difference was observed. No deaths occurred in either group.
Adenocarcinoma was the most common histologic type in both groups. However, no significant differences were observed in the distribution of histologic type (P = .489). The pathologic stages, including the T-stage (P = .154), N-stage (P = .631), and tumor, node and metastasis (TNM)-stage (P = .623), were similar between the two groups, with no significant differences (Table 4).
Categorical variables are presented as numbers (%).
CP, conventional pattern; MP, modular pattern; TNM, tumor, node and metastasis.
Discussion
In 2011, Gonzalez et al. first reported their experiences with uniportal VATS lobectomy;11,12 this technique rapidly became popular and has been performed worldwide during the past 5 years.8,13,14 Uniportal VATS has been shown to be associated with advantages, including equivalent safety, 14 less postoperative pain,15,16 and better cosmetic outcome than multiport VATS, which has attracted surgeons as well as patients.17,18 Many clinics have begun using this emerging technique, but varying outcomes have been reported among different centers.19–22 This suggests that the uniportal VATS technique is challenging, especially for the low-volume operation centers.
In terms of National Comprehensive Cancer Network guidelines, the radical resection of lung cancer comprises anatomic lobectomy and systemic lymphadenectomy. 23 In the CP group, lobectomy was performed before lymphadenectomy; this method has been widely described in published reports24,25 and was adopted during the initial phase of uniportal VATS lobectomy practice in our department. As the number of operations increased, two factors motivated us to modify the procedure. The first factor was the perception that the excision of the lymph nodes was actually performing the dissection of pulmonary vessels and bronchus. After the removal of the lymph nodes, the anatomy of the lung structures became clearer, facilitating the lobectomy. The other factor was that several adverse influences associated with the CP were observed, which are described as follows.
Due to the deep location, especially in the left thoracic cavity, subcarinal lymph node dissection with uniportal thoracoscopy is a challenging procedure. To obtain better exposure, we always retracted the dorsal segments anteriorly; traction tension can be applied through the lower lobe bronchus to move the carina toward the operated side. We also rotated the operation bed anteriorly to facilitate exposure. Therefore, once the lower lobe had been removed, it became difficult to achieve satisfying exposure in the absence of tension along the bronchus to the carina, which was also described by Feng et al. 13 In addition, the stumps of the lower pulmonary vein and bronchus would obstruct the camera view and interfere with the manipulation, which would force the surgeon to push or press the stumps with instruments such as a suction tip. Repeated scrapes of the vessel and bronchus stumps might cause injury, bleeding, or potential bronchopleural fistula.
Second, the dissection of subaortic lymph nodes was considered. Left RLN injury is a major complication during subaortic lymph node dissection. The primary means of prevention is to clearly expose the lymph node boundaries and the nerve, which can be achieved by retracting the upper lobe toward the anterior-inferior direction to fully expose the aortic-pulmonary window. If the upper lobe is resected, the pulmonary artery trunk and upper lobe artery stumps will rise and obstruct the view of the aortic-pulmonary window. The performance of the operation will become more difficult, especially for the dissection of lymph nodes that have adhered to the artery trunk. Consequently, the risk of injuring the RLN might be increased due to a poor exposure.
Third, the dissection of hilar lymph nodes was evaluated. Optimal visualization for the dissection of hilar lymph nodes includes moving the lobe to maintain tension along the vessels and bronchus, which facilitates the en bloc resection of the lymph nodes from the vascular sheath. After the removal of the lobe, the corresponding vessels and bronchus will shrink, and the anatomic layer tends to become indistinct.
In addition to the aforementioned technical factors, a potential challenge to the psychological state of the surgeon also exists. In the situation of the lobectomy procedure having consumed much time, it is more demanding for the surgeon who has suffered from fatigue to maintain consistent patience and carefulness to implement the following systematic lymphadenectomy; otherwise, the quality of lymph node dissection will be compromised.
In this study, the operation duration was significantly shortened and the intraoperative blood loss was reduced considerably by MP uniportal VATS compared with the CP. Although no significant difference was observed, the incidence of RLN injury in the MP group exhibited a decreasing trend compared with the CP group. We presume that the reductions in the operation duration, intraoperative blood loss, and secondary injury were due to the optimization of the operation procedure, which confirmed the principle that the highest extent of dissection and excision should be performed in each exposure view to eliminate repeated turnover and traction of the lung.
In terms of the length of the incision, which varied among different surgeons, a 4–6 cm incision was reported most often.8,9,26 In this study, we accomplished the operations through a 3 cm incision (except for the 11 conversions to thoracotomy). We once attempted to perform a lobectomy through a 2 cm incision, but it was difficult to pass the endoscopic stapler through the limited opening. Therefore, we mostly utilized such a small incision for bullae resection, sympathectomy, and some other cases with minor complexity. We believe that the 3 cm incision is more reasonable and feasible for the treatment of lung cancer with the current surgical instruments.
Conclusions
In summary, the MP of uniportal VATS lobectomy transformed the complicated operation into programmed modules that are easier to manipulate, especially for beginners and unskilled operators. In our hands, it appeared to be a superior technique to the conventional approach in terms of improving the efficacy and reducing intraoperative blood loss. We suggest that MP uniportal VATS should be an alternative to curative surgery for lung cancer. However, there are limitations of this study, including its retrospective nature and the lack of oncological results. As the number of uniportal VATS procedures is increasing, further studies based on higher evidence levels are required to confirm additional findings, including surgical and oncological findings.
Footnotes
Acknowledgment
This work was supported by the Innovation Research Funding of Huazhong University of Science and Technology (Grant No. 2015TS140).
Disclosure Statement
No competing financial interests exist.