
Abstract
Abstract
Background:
Idiopathic bulbar urethritis (IBU) is characterized by hematuria ± dysuria without infection. Symptoms result from inflammation of the bulbar urethra, distal to external sphincter. IBU is difficult to manage and there is no recommended therapy.
Objective:
To determine whether instillation of triamcinolone acetonide is a useful treatment of IBU and its associated complications.
Setting and Participants:
Data were prospectively collected, for 22 months, on 14 consecutive patients presenting with terminal hematuria or blood spotting ± dysuria to a pediatric urology unit. Median age was 12 years (range: 10–15). Mean symptom duration was 13 months (range: 8–24). Normal baseline laboratory blood tests, urine cultures, and ultrasound assessments were seen in all; therefore, none were excluded on the basis of a known pathology. Follow-up telephone interviews, to assess symptom persistence and side effects, were performed at 6 weeks postintervention. The mean follow-up period was 15 months (range: 4–20).
Intervention:
Visual confirmation of IBU was obtained cystoscopically and 40 mg of triamcinolone was instilled to the inflamed area under direct vision using an open-ended ureteral catheter.
Outcome Measurements:
Symptoms resolution was the primary outcome. Repeat cystoscopic assessment ± triamcinolone instillation was recorded, as was the occurrence of complications.
Results and Limitations:
Seven patients (50%) required at least one further treatment. Overall complete or partial resolution was reported in 12/14 patients (85.7%). No side effects were reported.
Conclusions:
This small prospective series demonstrates that intraurethral instillation of triamcinolone seems to be a promising treatment option to alleviate inflammatory symptoms in majority of cases of idiopathic urethritis.
Patient Summary:
Fourteen boys with inflammation of the urethra, with no identifiable cause, were treated by topically triamcinolone, directly to the inflamed area. We demonstrate an 85.7% complete/partial resolution of symptoms with no side effects seen.
Introduction
I
The etiology of idiopathic urethritis is unknown and unsurprisingly there are many theories including infective, 6 immunological, 2 and hormonal. 4 More recently dysfunctional elimination syndrome is credited with being associated with IBU, whereby a combination of turbulent flow and abnormal epithelium results in the symptoms seen. 3
Owing to the uncertainty of cause, there remains debate over the most appropriate management strategy. In fact, in the initial IBU case series in 1971, Williams and Mikhael underline the lack of information regarding urethritis in male children. 7 Forty-three years later, a lack of consensus still exists. We hypothesized that a long acting steroid instilled into the area of inflammation would help alleviate the symptoms for a good while facilitating early resolution. This article reports our preliminary experience using urethral triamcinolone instillation in the treatment of IBU.
Patients and Methods
Prospective data were collected for consecutive patients seen by a single surgeon at a tertiary pediatric urology center, presenting with symptoms suggestive of IBU. The period of the study was from August 2012 and June 2014. Exclusion criteria included an alternative cause for their symptoms suggested within the history or confirmed on investigation; thereby by definition not IBU. Information regarding demographics, duration, and nature of symptoms, previous history, and laboratory and radiological investigations were recorded before any procedure. Written parental consent was obtained for the procedure and where appropriate was countersigned by the child.
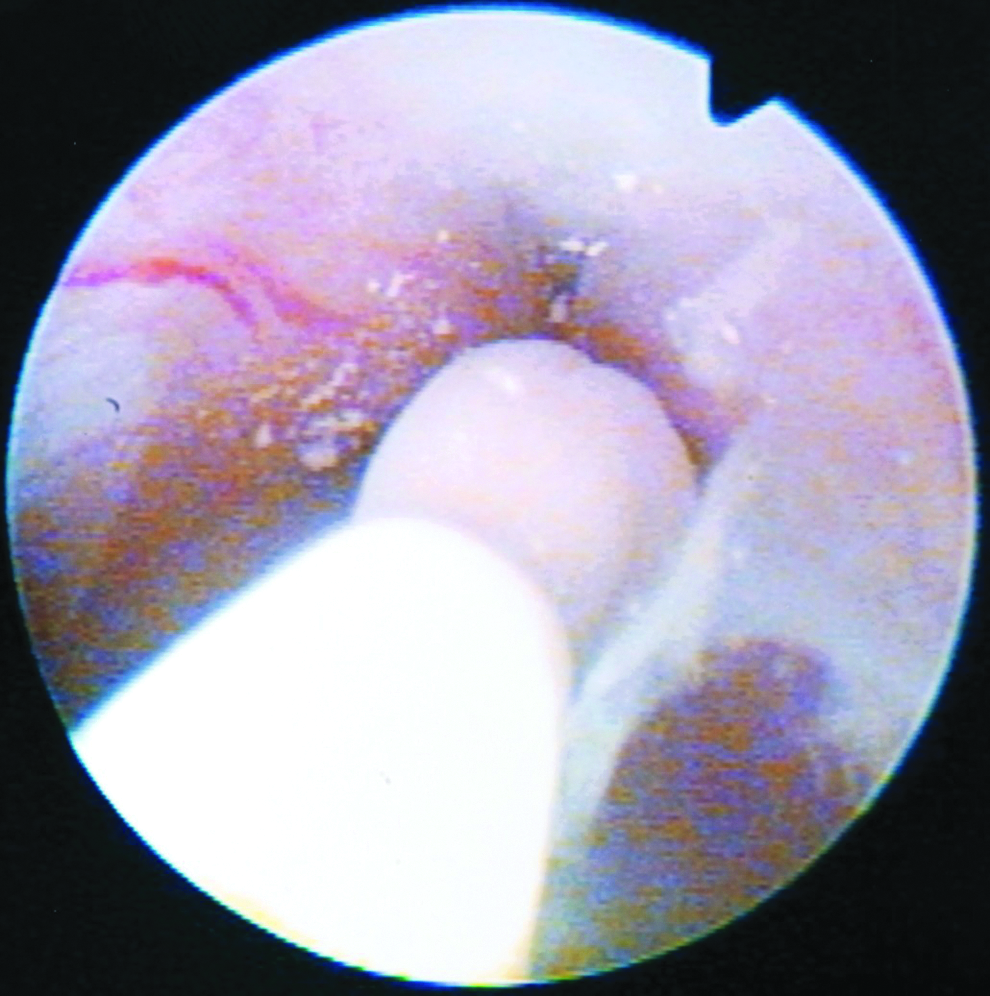
Visual confirmation of IBU was performed using a rigid cystoscope (Fig. 1). Single-dose intravenous gentamycin (2 mg/kg) at induction was given as prophylaxis against infection. Once IBU was identified, triamcinolone acetonide suspension was instilled directly onto the inflamed area under direct cystoscopic vision using an open-ended ureteral catheter (Fig. 2). The initial dose of triamcinolone acetonide was 40 mg and subsequent doses delivered at 80 mg. Residual steroid within the ureteral catheter was successfully delivered by flushing with 0.9% saline (Fig. 3). Postoperatively, no indwelling catheters were left in situ. After recovery, the child was asked to postpone micturition for as long as possible to ensure sufficient exposure of the inflamed area to the treatment. Children went home the same day with oral analgesics and 5 days of oral antibiotics.

Cystoscopic image of inflamed bulbar urethra in a patient with idiopathic urethritis.
Triamcinolone acetonide was instilled directly onto the inflamed area under direct vision using an open-ended ureteral catheter.

Cystoscopic appearance of the bulbar urethra after steroid instillation.
All patients had a telephone consultation at ∼6 weeks after the instillation to reassess symptoms and elucidate possible side effects. Routine review in clinic was only arranged if symptoms recurred or were reported as persisting at the telephone interview. No routine follow-up cystoscopy was arranged in children in whom symptoms had resolved.
Results
Between August 2012 and June 2014, 14 patients presented with symptoms suggestive of IBU and underwent cystoscopic assessment and intraurethral instillation of triamcinolone. The median age at the time of presentation was 12 years (range: 10–15). All 14/14 patients had symptoms of terminal hematuria or blood spotting and 13/14 patients had dysuria. Symptom duration was > 6 months in all 14 children, mean 13 months (range: 8–24). Circumcision had been performed in 9 patients; 8 of whom were for religious reasons. None of our children reported being sexually active. All 14 children had normal full blood count, urea and electrolytes, and serum C-reactive protein. Urine cultures were all negative. Ultrasound scan to rule out anatomical anomalies was performed in 14/14 patients; all scans were reported as normal.
Cystoscopic confirmation of inflammation± hyperemia was seen in all 14 patients within the posterior urethra. All were associated with either a white phlegmonous exudate or mucosal irregularity typical of posterior urethritis (Fig. 1). None of the 14 patients demonstrated stricture. All 14 patients received 40 or 80 mg triamcinolone as per Patients and Methods section. None of the children required an overnight stay in hospital.
All patients underwent the telephone follow-up consultation at ∼6 weeks. Complete resolution was reported in 4 (28.6%) cases, 2 of these have not reported further symptoms at 12 and 18 months, respectively. However, at 6 and 7 months postinitial instillation, the other 2 patients developed recurrent symptoms. Repeat cystoscopic evaluation demonstrated mild inflammation and further triamcinolone instillation was performed using 80 mg, these patients are now symptom free.
A further 6 patients reported partial improvement (42.9%), the majority of benefit (4 in 6 patients) was seen in relation to hematuria. A watch-and-wait policy was adopted in 2 children with very mild persistent symptoms, both in whom the condition has reportedly resolved. The remaining 4 patients underwent cystoscopy; 1 patient had normal findings and 3 patients had evidence of mild inflammation. These 3 received 80 mg of triamcinolone, delivered in the same way as the initial treatment. Two of the 3 patients improved, 1 patient had persistence of symptoms.
Two patients (14.35%) reported no change in symptoms after 6 weeks of the first treatment with mild inflammation seen on repeat cystoscopy. Subsequent instillation of triamcinolone was performed: 1 child at 2 months and the other at 4 months postinitial treatment. After this, 1 child had seen partial improvement with abolition of hematuria and mild dysuria. Persistent symptoms were reported by the other patient, further cystoscopy showed mild urethritis and a third 80 mg of triamcinolone was utilized; however, symptoms still persist in this case.
In summary, overall mean follow-up period was 15 months (range: 4–20); at this point 7 children (50%) had undergone a further cystoscopy and triamcinolone instillation. One of these had required a third procedure. Complete or partial resolution was reported in 12/14 patients (85.7%). No side effects were reported.
Discussion
Idiopathic bulbar urethritis is a problem affecting male children and was first described in 17 patients by Williams and Mikhael. 7 The differential diagnosis may include infectious urethritis, calculus, tumor, stricture, arteriovenous malformation, or fibroepithelial polyp. 8 None of the boys in this series had any identifiable cause for their symptoms. IBU is not uncommon; however, there is little literature on the subject including consensus on etiology and management.
Infection has been thought to play a role in IBU2,6; however, urine culture invariably fails to reveal any organism. To add doubt over the role of infection, treatment with antibiotics has been advocated by some, but no improvement in symptoms has been observed. 2 It is reported that with growing age and attaining maturity, recurrence of symptoms tend to end,2,3 perhaps suggesting a hormonal component, which has led to the assumption that prepubertal hormonal changes are perhaps the most important triggering event of the condition.2–4 Whether these hormonal influences alter the epithelial lining of the urethra, with engorgement of blood vessels and an increased tendency to bleed, remains to be supported with scientific evidence.
Children who exhibit dysfunctional voiding, as part of a dysfunctional elimination syndrome, may be at an increased risk of developing IBU. Herz speculated that it is the narrowing at the external sphincter, due to poor relaxation or dyssynergia that creates turbulent flow and increased voiding pressures. 1 The altered fluid dynamics in these cases diminish flow, irritate engorged blood vessels that cause bleeding, progressive scarring, and stricture formation. Docimo et al. also postulated that bleeding from abnormal epithelium was exacerbated by increased urethral voiding pressures. 4 The possibility of a combination of the mentioned factors may need to be considered.
Intra-articular corticosteroid injection (IACI) is associated with reduction in inflammatory markers such as C-reactive protein and erythrocyte sedimentation rate 9 that start few days after the IACI and could last for months. IACI may not only induce remission in arthritis but also improve extra-articular manifestations. 10 A review article published in 2009 analyzed all articles in the English literature with regard to the systemic effects of IACI in humans 11 ; overall no significant adverse systemic effects were reported.
Various articles have compared the efficacy of different steroid formulations, many in the field of IACIs; several report triamcinolone to have a superior efficacy than other preparations; including methylprednisolone,12,13 whereas others report no difference. 14 Triamcinolone has mainly glucocorticoid activity and acts to limit polymorphonuclear leukocyte migration, prevents increased capillary permeability, thus it reduces inflammation and ultimately may help treat our IBU patients. Considering the limitation of therapeutic modalities available for IBU, we suggested instillation of long-acting steroid in the inflamed urethra.
We are reporting our experience of triamcinolone acetonide instillation for IBU and we believe this is the first prospective case series of its kind managing IBU in prepubertal boys. Steroid administration has been used by Gafni-Kane et al. 15 for bladder pain syndrome/interstitial cystitis with reasonable success. Morita and Ohashi have described the successful application of intravesical steroid instillation to treat women with urethral syndrome and urethritis. 16 Eradi and Ninan 17 presented intravesical administration of steroid for the treatment of IBU. Ninan et al. 18 presented a case report of steroid treatment for recurrent epididymitis secondary to idiopathic urethritis and urethrovasal reflux. The same group in 2014 published a retrospectively collected data series of 16 patients treated with intraurethral instillation of either triamcinolone or methylprednisolone. 19 They report 93.6% complete resolution rate with a mean follow-up of 19.4 months (range: 1–74) and a retreatment rate of 62.5%.
Our method has the advantage of locally delivering corticosteroids through a cystoscope at the time of diagnosis and we believe this reduces the potential for systemic side effects. However, some studies report iatrogenic injury and potential for urethral stricture postcystoscopic examination. One of 19 patients in the series by Harrison and Whitaker 2 developed a urethral stricture postcystoscopic assessment. As a result, watchful waiting and reassurance have been the primary mode of treatment of IBU by the majority. Walker et al. 8 described the natural history of IBU in a retrospective study of 27 boys suggesting expectant management, partly due to its self-limiting nature and lack of treatment even if cystoscopic confirmation of a diagnosis is sought. Our strategy of simultaneous diagnostic cystoscopy and instillation of triamcinolone would hopefully overcome this limitation.
Harrison and Whitaker found cystoscopy an essential tool with characteristic and consistent findings in their selected group. 2 In addition, a small series of 5 children's abnormal cystoscopic findings were reported in all. 4 A further study of 17 patients recorded only 1 negative cystoscopy, the other 16 demonstrated bulbar urethritis or hyperemia. 6 Poch et al. 5 identified that no consensus or selection criteria existed for cystoscopy in IBU patients and reported a 10-year retrospective review of 66 patients. The authors concluded that > 6 months unrelenting symptoms and/or obstructive/abnormal uroflow was a good indication for cystoscopic evaluation. In our series, all cases had symptoms > 6 months before cystoscopy (mean: 12 months, range: 8–24) and 14/14 patients (100%) had abnormal cystoscopic findings consistent with IBU.
Docimo et al. believe that the typical whitish plaque seen in bulbar urethra is consistent with squamous metaplasia, secondary to chronic inflammation or irritation. 4 This inflammation might also explain stricture formation associated with this syndrome. Cohorts are reported that have developed stricture disease in the absence of instrumentation. Dewan and Wilson, in a case series of 7, report 4 cases of stricture, 2 known previously in the absence of prior instrumentation. 20 Walker et al. state that cystoscopy is useful to confirm the diagnosis of IBU if symptoms persist for >2 years. 8 However, as highlighted by Walker et al., the etiology is unknown and some studies suggest that in fact it is the chronicity of untreated IBU that increases the risk of scarring and stricture formation.5,20
None of our 14 cases, who underwent at least one diagnostic ± therapeutic cystoscopy, developed strictures. We, therefore, believe that one possible reason for not seeing stricture in our patients is early intervention with triamcinolone instillation. It is suggested that the anti-inflammatory effect of the steroid may break a vicious cycle of inflammation, dysfunctional flow dynamics, and increased pressures within the urethra. We acknowledge these are early results of a novel intervention, and a large sample size along with long-term follow-up is needed to substantiate our results. However, we believe that intraurethral triamcinolone instillation is an additional treatment option in IBU.
Limitations of this pilot study are clearly the numbers and we hope to conduct a randomized trial in the future on the back of this pilot study. We realize that we should include a symptom score questionnaire for future work to objectively assess the response from this treatment.
Conclusions
Early results in a small prospective series demonstrate that instillation of triamcinolone into the urethra seems to be a promising treatment option to alleviate inflammatory symptoms in majority of cases of idiopathic urethritis. Large series with longer follow-up is required to corroborate the results.
Footnotes
Disclosure Statement
No competing financial interests exist.