
Abstract
Abstract
Background:
Peroral endoscopic myotomy (POEM) has gained acceptance as a treatment for achalasia. The aim of this study was to assess symptomatic, quality of life (QoL), and physiological outcomes of POEM using standardized methods.
Materials and Methods:
Patients who were planned to undergo POEM were evaluated pre- and postoperatively with timed barium esophagogram (TBE), high-resolution manometry (HRM), the achalasia symptom questionnaire (ASQ) (best score 10, worst score 31), and the short form (SF)-36 (best score 100, worst score 0). Nine patients completed postoperative HRM, TBE, and 48 hours esophageal pH monitoring. A P-value of <.05 was considered statistically significant.
Results:
A total of 34 of 37 patients completed the POEM procedure. There was improvement in the ASQ scores and in QoL. HRM integrated relaxation pressures (IRPs) improved from 31.4 ± 10.8 mmHg preoperatively to 12.3 ± 6.7 mmHg postoperatively, and lower esophageal sphincter pressure (LESP) improved from 49.1 ± 16.9 mmHg preoperatively to 23.1 ± 9.4 mmHg postoperatively. Of the 7 patients who were evaluated with 48-hour pH monitoring postoperatively, 5 patients (71%) demonstrated pathological reflux with an average Demeester score of 23.1 ± 19.1. There was a negative linear correlation between LESP change and Demeester scores (r = −0.7, P = .03).
Conclusion:
The POEM procedure significantly improves achalasia-related symptoms and improves social functioning. Physiologically, there is reduction in both IRP and LESP. Postoperative pathological reflux is correlated with LESP reduction.
Introduction
A
More recent data including a meta-analysis of existing POEM studies also show a significant reduction of LESPs and improvement of Eckhardt symptom score in patients who underwent POEM. 4 POEM has also been shown to have similar safety and efficacy outcomes from the gold standard LHM. 5 One of the concerns of POEM is the development of gastroesophageal reflux (GER) postoperatively. 2 The rates of post-POEM symptomatic reflux varies from 0% to 37%. 6 One study reports the incidence of objective reflux on endoscopy or pH study is as high as 64.7%, although only 16% of these patients were symptomatic. 7 We present our experience with patients who underwent a POEM for achalasia who received pre- and postoperative high-resolution manometry (HRM), timed barium esophagogram (TBE), Urbach's “Measure of Achalasia Disease Severity” (ADS) questionnaire, and evaluation of quality-of-life (QoL) scale using short form (SF)-36.
Materials and Methods
All patients referred for surgical treatment of achalasia were evaluated. Evaluation included history and physical examination and review of prior testing to determine suitability for general anesthesia. If necessary, repeated testing to include upper gastrointestinal series and esophagogastroduodenoscopy was completed. All patients underwent preoperative evaluation with TBE and HRM. The height of the water column was measured at 1 and 5 minutes (Fig. 1). A barium tablet was ingested at 10 minutes and passage was noted. Patients also underwent HRM to determine basal LESP, integrated relaxation pressure (IRP), presence of panesophageal pressurization, and achalasia type (Fig. 2).
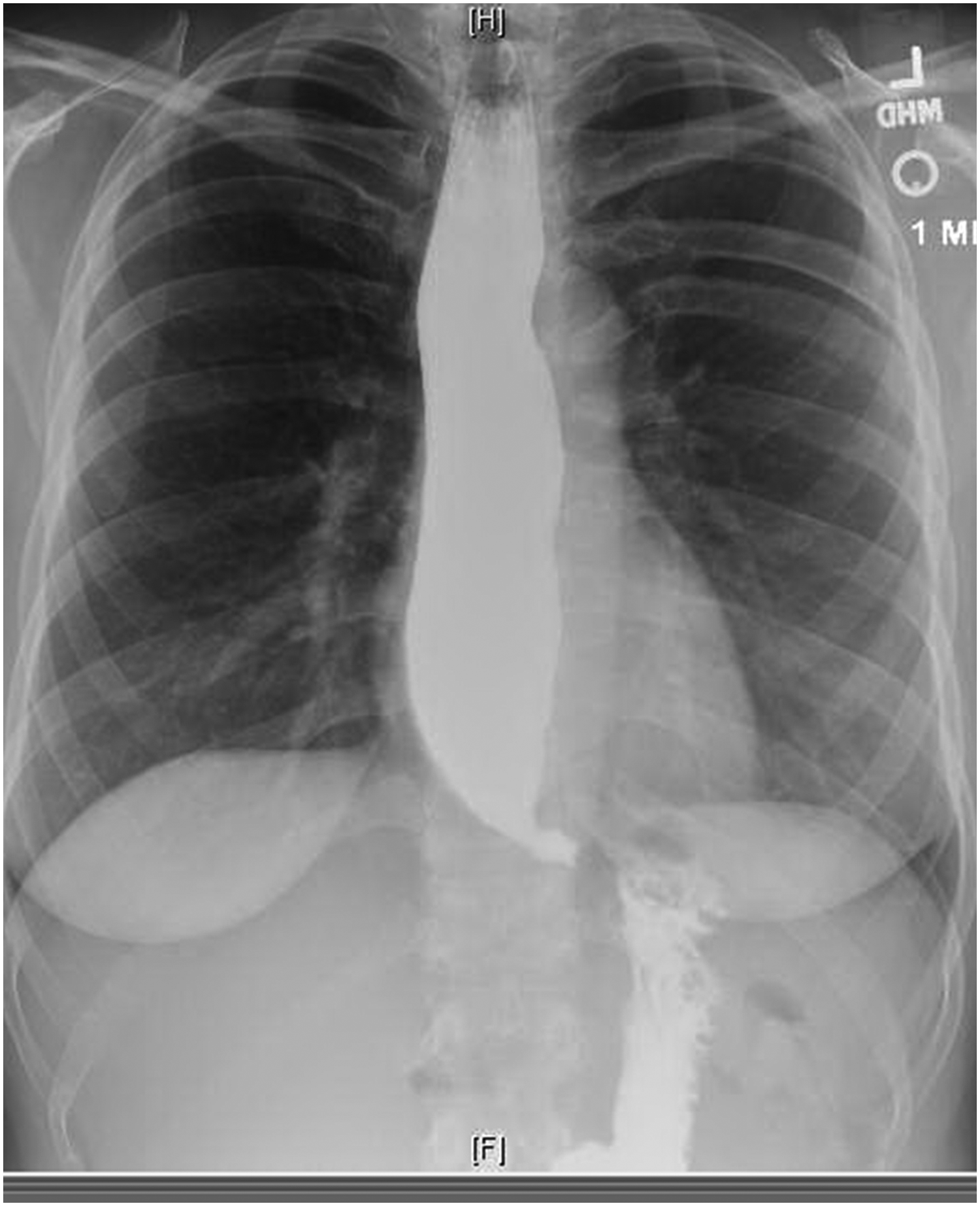
Example of 1 minute preoperative timed barium esophagogram demonstrating a column of barium superior to the clavicles and “bird's beaking” of the gastroesophageal junction.

Example of a preoperative high-resolution esophageal manometry of the same patient as Figure 1 demonstrates type II achalasia.
During initial visit, patients also completed an achalasia symptom severity questionnaire and a generic QoL instrument. The QoL instrument was the SF-36, which measures eight QoL domains. These include physical functioning, physical role functioning, bodily pain, general health, vitality, mental health, social functioning, and emotional role functioning (best score 100, worst score 0). 8 Patients also completed achalasia symptom questionnaire (ASQ). 9 Scores are based on 10 items of disease-specific health-related QoL measures including food tolerance, dysphagia-related behavior modifications, pain, heartburn, distress, lifestyle limitation, and satisfaction (best score 10, worse score is 31).
Patients underwent POEM procedure as follows: patients were placed in a supine position and general endotracheal anesthesia was induced. A bite block was placed and an initial esophagogastroduodenoscopy was done to assess for suitability to proceed with the operation. Causes to abort would include extensive food retention in the esophagus, candidia esophagitis, or esophageal mucosal pathology. After the initial endoscopy, a beveled cap was placed on the endoscope and it was reintroduced into the esophagus. This was taken to the gastroesophageal junction and its distance from the bite block was noted (Fig. 3a). The scope was withdrawn for 10 cm and the submucosal space along the anterior aspect of the esophagus was injected with 10 cc of normal saline with methylene blue and epinephrine. Using the triangle tip endoscopic knife (Olympus, Tokyo, Japan), a mucosotomy was made (Fig. 3b). This was extended sufficiently enough to allow the bevel-capped endoscope to enter the submucosal space (Fig. 3c). The submucosal space was developed along the distal esophagus and extended for at least 3 cm onto the gastric cardia (Fig. 3d). This requires additional injection of methylene blue-colored normal saline without epinephrine. Once the tunnel was completed, the circular muscle fibers of the esophagus were divided with a triangle tip knife starting at least 6 cm from the gastroesophageal junction and extended by dividing the clasp and sling fibers of the gastric cardia for at least 2 cm (Fig. 3e). Once the adequacy of the myotomy was confirmed, the mucosotomy was closed with endoclips (Cook Medical, Inc., Bloomington, IN) (Fig. 3f). A nasogastric tube was placed. The patient underwent a postoperative esophagogram the next day. If no perforation or leak was noted, the nasogastric tube was removed and liquids begun. If the patient tolerated the liquids, he or she was advanced to a soft diet. If the patient tolerated the soft diet, then he or she was discharged home. The patient had a follow-up in about 2 weeks, if he or she was tolerating a soft diet, then the patient was advanced to a regular diet. The final postoperative evaluation and completion of the ASQ and SF-36 were done at that time. After the final postoperative visit, the patient was referred for postoperative TBE, HRM, and 48 hours pH monitoring.
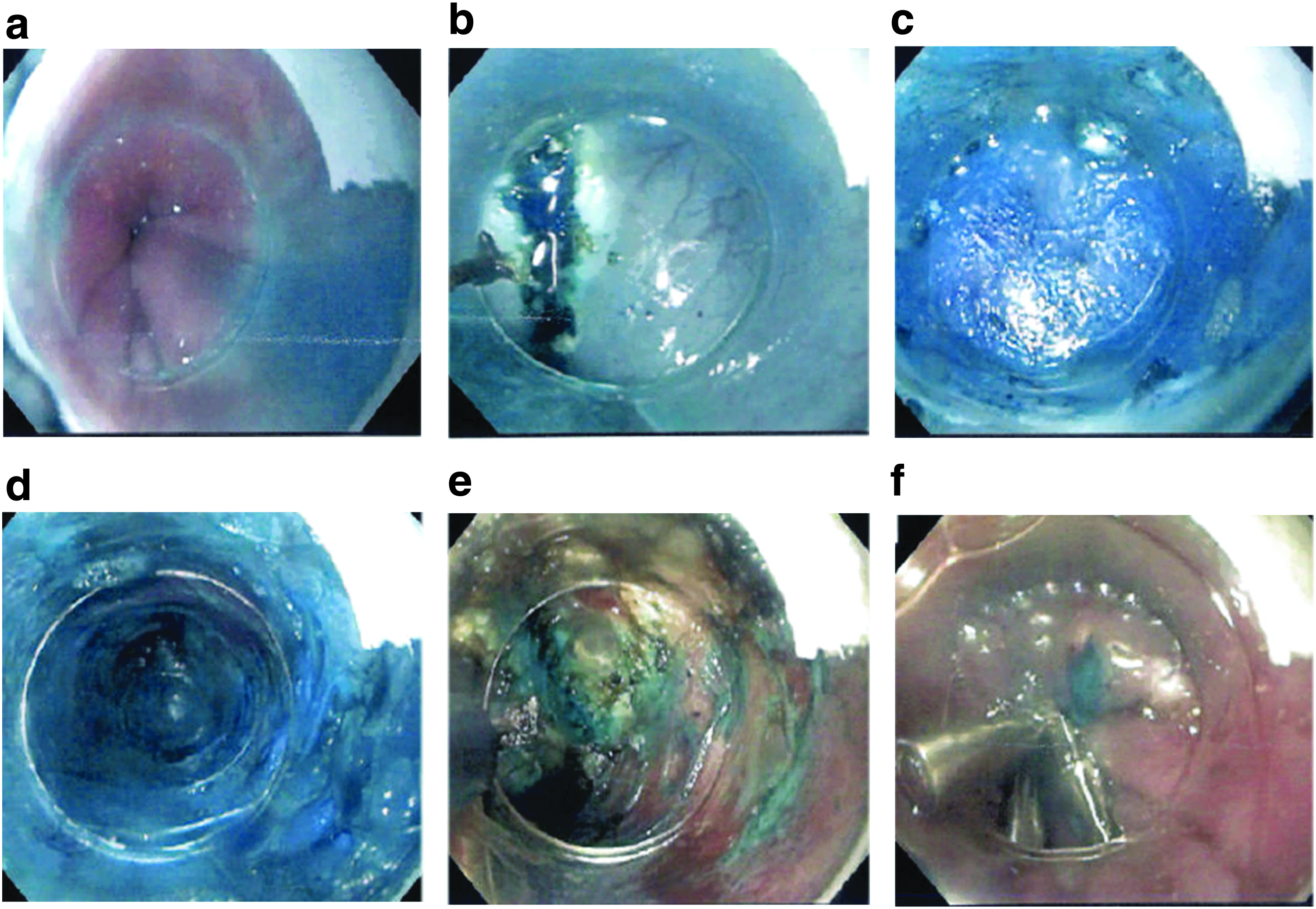
Pictures of the salient steps in the POEM procedure.
Statistical analysis
Continuous data were analyzed using Students' t-test. Correlation was determined using linear regression analysis. A P-value of .05 was considered significant.
Results
Demographics
There were 21 males and 16 females, with a mean age of 58 ± 19 years (range 20–87 years). Of the 37 patients initially attempted, 34 were completed. The reasons for aborting 3 cases were a large vessel in the submucosal space, which was felt to be too large to control with endoscopic electrosurgery, and complete perforation through the esophageal mucosa into the mediastinum, and a misdiagnosis of achalasia in a patient with a submucosal gastroesophageal junction adenocarcinoma. None of these patients suffered an adverse event because of the procedure. All patients were seen at 2 weeks; however, we had 7 patients lost to 6 weeks follow-up. Therefore, there were 27 patients who completed the QoL questionnaires. In addition, 7 patients received ambulatory pH studies. Demeester scores were calculated for these patients. Postoperatively, 9 patients completed the SF-36 questionnaire, whereas 17 patients completed the ASD questionnaire. No severe complications were seen in these patients during their hospital stay.
Quality of life measures
Symptom severity
There was statistically significant improvement in the ADS scores (P < .05). The mean preoperative ADS score was 24.8 ± 2.8 and mean postoperative score was 13.2 ± 3.7.
Quality of life
There was improved score in seven of the eight domains of the SF-36, but there was statistically significant improvement of the social functioning domain of the SF-36 (P < .05) (Table 1).
For achalasia symptom questionnaire, best score is 10, worst score is 31.
For SF-36, best score is 100, worst score is 0.
SF, short form.
Physiological outcomes
TBE improved in most patients (Fig. 4). HRM IRPs showed significant improvement from a preoperative average of 31.4 ± 10.8 and a postoperative average of 12.3 ± 6.7 (P < .05) and basal LESP also showed significant improvement with an average preoperative value of 49.1 ± 16.9 mmHg and a postoperative value of 23.1 ± 9.4 mmHg (P < .05) (Fig. 5). Of the 7 patients who received postoperative 48-hour pH monitoring, 5 patients (71%) demonstrated pathological reflux with an average Demeester score of 23.1 ± 19.1. Of the 5 patients with abnormal pH monitoring, only 2 had “occasional” heartburn symptoms, whereas the other 3 were completely asymptomatic. There was a statistically significant negative linear correlation between LESP change and Demeester scores (r = −0.7, P = .03) (Fig. 6). One patient who had persistent symptoms of dysphagia and physiological testing suggestive of persistent achalasia was found to have an incomplete myotomy at laparoscopic Heller myotomy (Fig. 7).
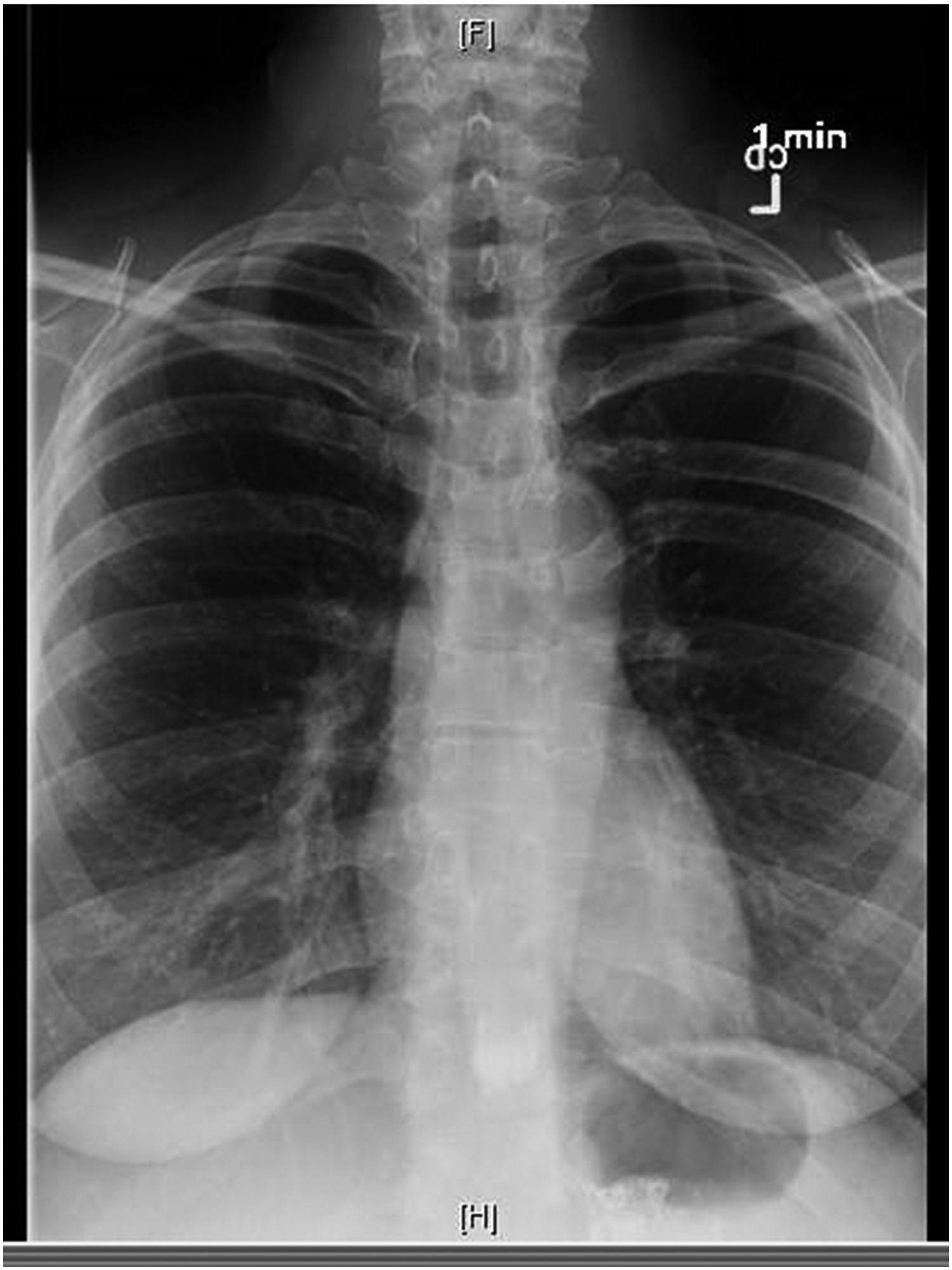
Post-POEM timed barium esophagogram of the same patient as shown in Figure 1. Note that there is complete clearance of barium after 1 minute. POEM, peroral endoscopic myotomy.

Example of a post-POEM high-resolution esophageal manometry of the same patient as shown in Figure 1. Note the resolution of the panesophageal pressurization and relaxation of the lower esophageal sphincter. POEM, peroral endoscopic myotomy.
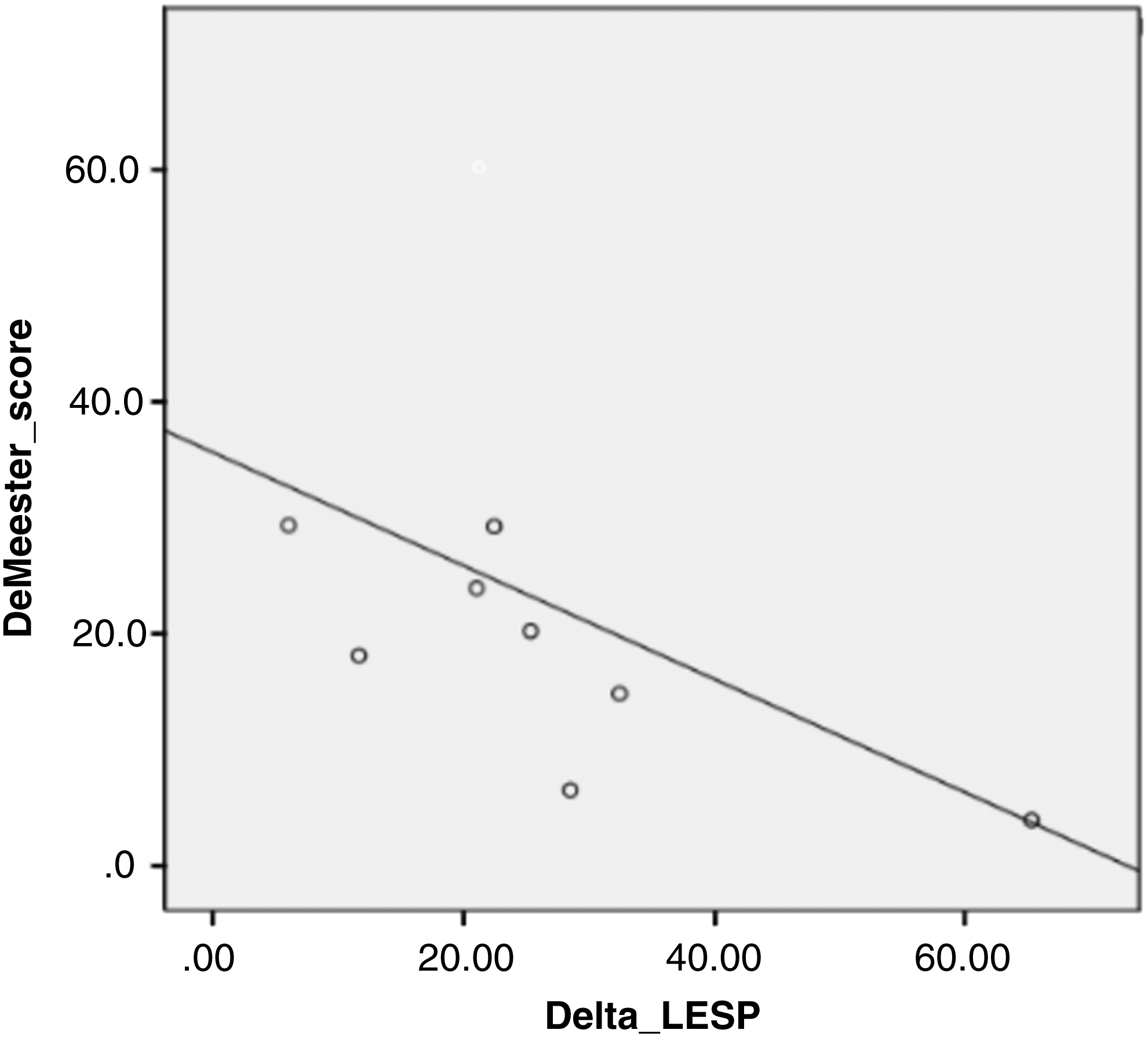
Linear regression analysis comparing post-POEM DeMeester score with LESP. There is a direct relationship between increased DeMeester score and LESP. LESP, lower esophageal sphincter pressure; POEM, peroral endoscopic myotomy.

Example of a post-POEM incomplete myotomy. The suction device points to the lowest extent of the myotomy. POEM, peroral endoscopic myotomy.
Discussion
In our case series of patients who underwent POEM, there was a significant reduction in the IRP and LESP. This is consistent with the published data on POEM procedure short-term physiological outcomes.2,4,10 ADS scores were significantly decreased, indicating symptomatic improvement for patients as well. 11 Inoue et al. published data on 500 POEM patients showed symptomatic improvement of 88% 3 years postoperatively. 7 This suggests that long-term efficacy of POEM procedure may be consistent with short-term outcomes but more long-term data are needed to make any conclusion.
QoL improvement remains an important factor for patients with achalasia. Our data suggest improvement in all but one domain of QoL as well as statistically significant improvement in the social functioning domain. Liu et al. showed similar QoL improvements with patients undergoing POEM. 12 The gold standard LHM also shows improvement in all QoL domains on SF-36. 13 This suggests that with regard to the patient experience, the postoperative QoL changes are similar between the LHM and POEM.
Although the efficacy of POEM has been well established, the long-term complications of this study remain unclear. The risk of GER remains a concern for POEM patients as more recent studies have shown more significant reflux than previously described.2,6,7 In the largest case series study, the incidence of gastroesophageal reflux disease was found to be 21.3% at 3 years follow-up. Esophagitis was seen in 56.3% of patients on endoscopic evaluation in the same study. 7 We found pathological reflux in 5 of our patients on ambulatory pH studies. Interestingly, the HRM and pH studies show a negative linear correlation between the Demeester score and LESP. This brings to light the possible limitation of POEM. The gold standard LHM offers a partial fundoplication, which helps regain some LESP to reduce reflux. The POEM procedure effectively reduces LESPs but has no anti reflux counterpart. Our data suggest that as we reduce the LESpressure, we are also increasing the risk for reflux in a linear manner. We have changed our practice over time. We initially only treated symptomatic patients with proton pump inhibitors, but now we prophylactically place all POEM patients on proton pump inhibitors. Although our study was limited by follow-up and population size, these data help us understand the nature of reflux in postprocedure achalasia patients. Larger size, long-term follow-up studies are needed to strengthen our understanding of the relationship between LESP and acid reflux in POEM patients.
Footnotes
Disclosure Statement
No competing financial interests exist.