
Abstract
Abstract
Objective:
Laparoscopic anorectoplasty (LARRP) for the treatment of select anorectal malformations has gained popularity due to enhanced visualization of the fistula and the ability to place the rectum within the sphincter complex while minimizing division of muscles and the perineal incision. However, given the technical challenges and reported complications of ligation, a number of techniques have been described, including using clips, suture ligation, endoloops, or division without closure. We aimed to evaluate fistula closure and division for high imperforate anus using a 5-mm stapler (JustRight Surgical, Boulder, CO).
Materials and Methods:
A retrospective chart review was performed on patients who underwent LAARP for imperforate anus between March 2015 and December 2016.
Results:
Four patients underwent LAARP with division of the fistula using the 5-mm stapler. The average age was 3.2 months and average weight was 4.5 kg. The location of the fistula was rectoprostatic in 3 cases and rectobladder neck in 1 case. There were no complications.
Conclusion:
Division of a fistula at or above the level of the prostate can safely and effectively be performed with the 5-mm stapler. The stapler allows for division flush with the urethra or bladder ergonomically and quickly.
Introduction
R
A number of complications have been described following the various types of fistula ligations. Urethral stricture and recurrent fistula have been described after clip ligation. 4 A urethral diverticulum can also form if the fistula is not divided flush, which can be difficult with a bulky distal rectum and/or a broad base of a rectobulbar fistula. 5 In addition, the angles are awkward for placing sutures. We aimed to evaluate fistula closure and division using a 5-mm stapler (JustRight Surgical).
Materials and Methods
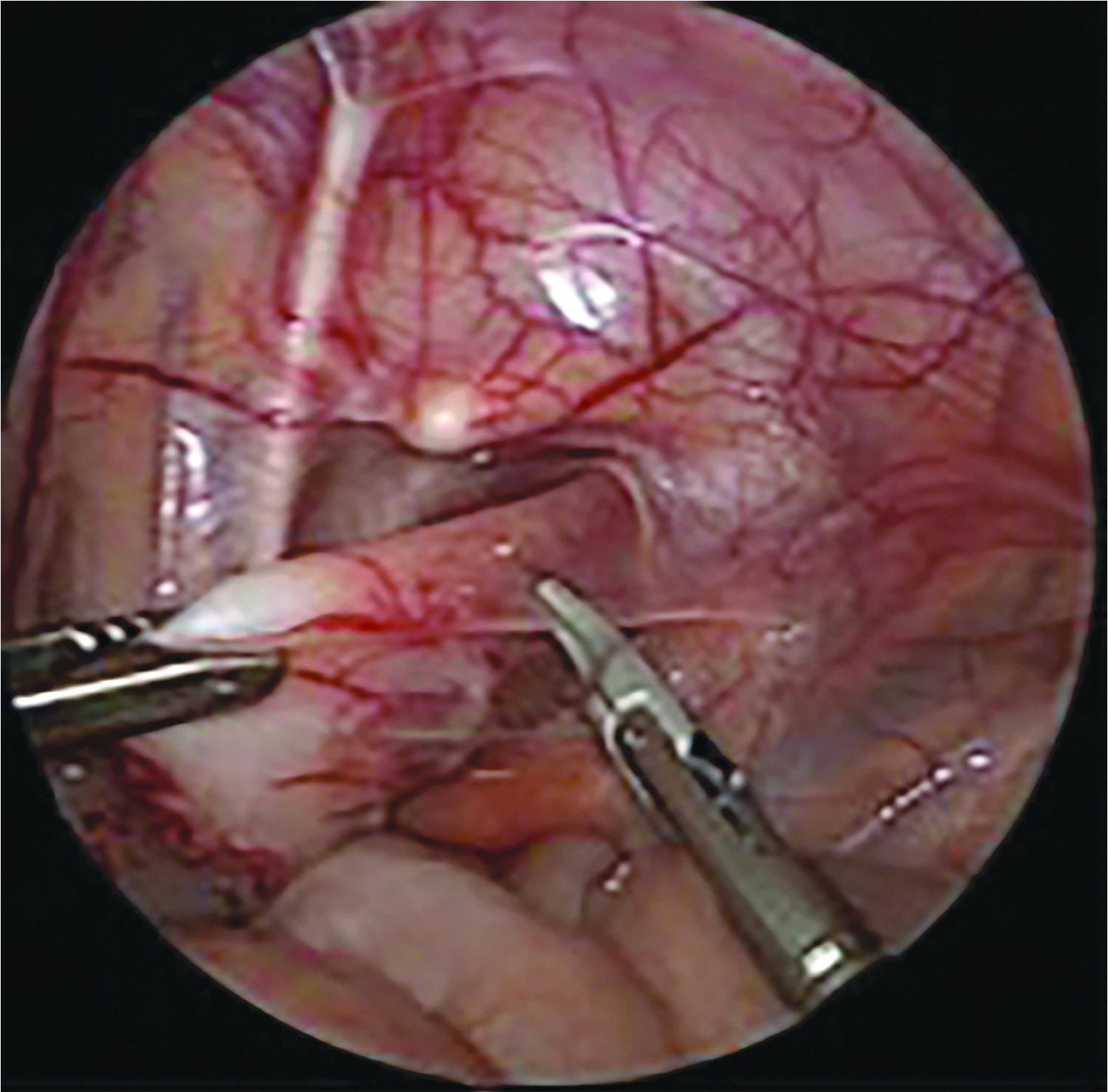
A retrospective chart review was performed on all patients who underwent LAARP for imperforate anus between March 2015 and December 2016 at a single institution. Data collection included age, weight, gender, type of fistula, length of stay, and complications. All patients underwent colostomy at birth and a distal colostogram before anorectoplasty to define the anatomic relationship of the fistula with the genitourinary structures. For the LAARP, a Foley catheter was placed sterilely for bladder decompression. An infraumbilical incision was made at the skin crease and a Veress needle used to insufflate the abdomen. A 4-mm trocar (nondisposable low profile; Karl Storz, CA) was placed for the camera. A 3-mm trocar was placed to the left and a 5-mm trocar (mini Step short 5 mm; Medtronic, Minneapolis, MN) was placed to the right of the abdomen. Rectal dissection was started at the peritoneal reflection using the 3-mm sealer (JustRight Surgical) (Fig. 1). The dissection was continued distally directly along the wall of the colon, preserving the lateral vessels and nearby pelvic structures. As the rectum tapered, the fistula was identified (Fig. 2) and divided at the insertion on either the bladder neck or posterior urethra with a 5-mm stapler (Fig. 3). Attention was then turned to the perineum, and the nerve stimulator (Pena Muscle Stimulator; Integra, Plainsboro, NJ) was used to mark the external sphincter complex. An ∼1-cm incision was made in the perineum and sharp dissection was used to divide the external sphincter in the midline. The intersphincteric plane was then developed bluntly through the center of the levator muscles. A Veress needle with sheath was then passed under direct laparoscopic vision through the center of the muscle complex behind the urethra. A series of radially expanding trocars were used to dilate the tract to 10 mm. The previously mobilized colon was then grasped and brought down through the trocar and out through the neoanus. After division of the staple line, anoplasty was then performed in the standard manner.
Dissection of the distal rectum starting at the peritoneal reflection.

Identification and dissection of the fistula.
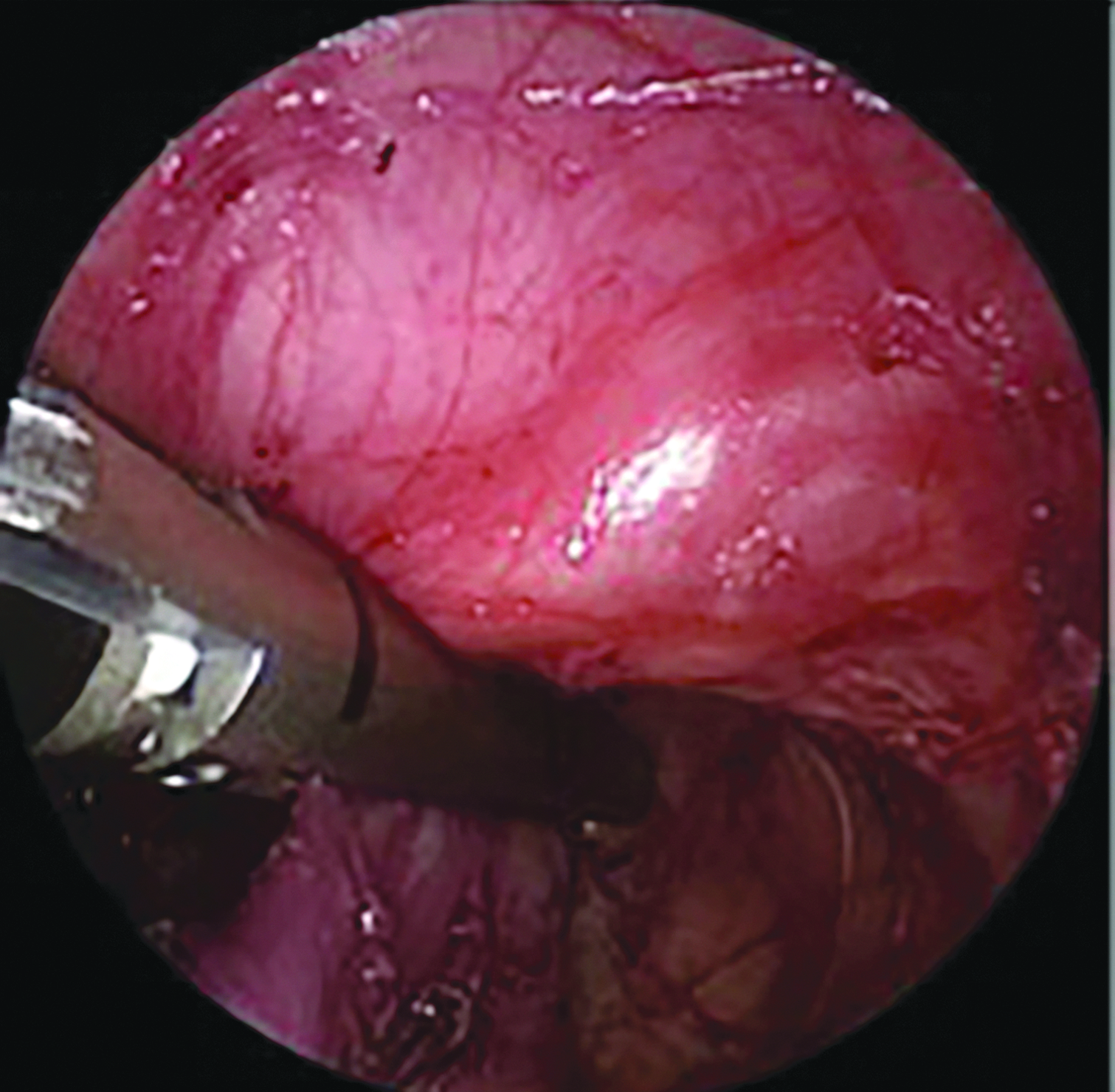
Division of the fistula with the 5-mm stapler flush with the bladder.
Results
Four patients underwent LAARP with division of the fistula using the endoscopic 5-mm stapler during the study period. The average age was 3.2 months (range 2–5 months) and average weight was 4.5 kg (range 3.5–5.6 kg). Three patients were male and 1 was female. The location of the fistula was rectoprostatic in 3 cases and rectobladder neck in 1 case. Patient characteristics are summarized in Table 1. All patients had a Foley catheter for 2 days postoperatively, and then it was removed. The duration of follow-up ranged from 1 to 15 months. There were no complications. Three of the 4 patients have undergone colostomy closure and are having regular bowel movements and feeding well.
ASD, atrial septal defect; CLD, chronic lung disease; GERD, gastroesophageal reflux disease; TEF, tracheoesophageal fistula; TOF, tetralogy of Fallot; VACTERL, vertebral, anorectal, cardiac, tracheo-esophageal fistula, renal, and limb; VUR, vesicoureteral reflux.
Patient 1 is ∼14 months old with a number of vertebral, anorectal, cardiac, tracheo-esophageal fistula, renal, and limb (VACTERL)-associated anomalies. A cystogram was performed at 1 year of age with no evidence of diverticulum or staples inside the urinary system (Fig. 4). He has bowel movements every day and good anal tone on digital rectal examination, but is too young to fully evaluate for continence. A cystogram was also performed on patient 3 by urology with Deflux instillation for vesicoureteral reflux when the patient was about 15 months old. There was also no evidence of staples, diverticulum, or any additional pathology.

Cystoscopy view with no evidence of diverticulum or staples.
Discussion
Anorectal malformations encompass a range of congenital defects that vary in regard to the technical difficulty of repair and functional outcome. The higher variants, including rectobladder neck and rectoprostatic urethra fistulas, are commonly associated with other malformations and have the worst prognosis for bowel control. In 2000, Georgeson et al. reported on a laparoscopically assisted technique (LAARP) for patients with these fistula types to minimize dividing the muscle complex from a perineal incision. 2 Advantages of this approach include enhanced pelvic visualization of the fistula and puborectalis muscles, decreased pain with avoidance of an open abdominal incision, and potentially fewer perineal wound complications.
In Georgeson's report, the fistula was clipped and sharply divided. A number of other techniques have been described subsequently to assure flush division of the fistula and reduce complications such as stricture and diverticulum, including suture ligation, use of endoloops, transperitoneal ligation, and division without ligation.3,4,6 However, many of these techniques are challenging, can result in slipping or migration of the tie or clip, and can be problematic to achieve a flush ligation especially with a thick or bulky fistula.
Division of the fistula with a 5-mm stapler was successful in our preliminary experience with this technique with no complications. The magnification and visualization afforded by the laparoscope allowed for complete dissection and identification of the fistula. Using the stapler on the fistula permits flush division. In addition, the rectum is closed following division of the fistula, possibly preventing any contamination during the remainder of the procedure. Although these patients had all been diverted with a colostomy, it is possible for there still to be some rectal contents present, distally allowing some spillage if left open. Longer term follow-up of bowel function is necessary to determine the functional outcome.
Concerns have been raised in the urologic literature regarding the development of urolithiasis after the use of staplers on the urinary system. There have been studies demonstrating that exposed metal in direct contact with urine may serve as a nidus for stone formation. 7 However, using a stapler on a fistula between the rectum and bladder neck or prostatic urethra is different than using it for urinary reconstructions or resections and less likely to be a nidus for urinary stones for a number of reasons. First, there may be other factors leading to urolithiasis in the urologic population, including anatomic factors, underlying urinary disorders, or other patient risk factors. In addition, in the case of division of a fistula, the staples would not be in direct contact with urine. The staples should either be outside of the urinary system or in the adventitial layer, as opposed to being in the mucosa. Finally, more recent studies have shown successful use of staples in urinary surgery without the formation of stones. 8 One study concluded that although the risk of stone formation is an ongoing concern in reconstructive urologic surgery, it has yet to materialize. 9 In the 2 patients that cystoscopy was performed on in follow-up, there was no evidence of diverticulum or outpouching of the urethra as well as no evidence of staples inside the bladder or urethra. Additional follow-up will be helpful to assure that urinary stones do not develop in the future.
Division of a fistula at or above the level of the prostate can safely and effectively be performed with the 5-mm stapler. The stapler allows for division flush with the urethra or bladder, is ergonomic and straightforward, and potentially minimizes spillage of rectal contents.
Footnotes
Disclosure Statement
Dr. Rothenberg, one of the coauthors of this article, is a founder and consultant for JustRight Surgical, the company that makes the 5-mm stapler used in this article for division of the fistula. JustRight Surgical has not had (and will not have) any impact on research conduct and manuscript preparation. For all other authors, no competing financial interests exist.