
Abstract
Abstract
Background:
Laparoscopic reversal of Hartmann's procedure offers reduced morbidity compared with open surgery while improving reversal rates. However, it is one of the most technically challenging operations in minimally invasive colorectal surgery, with further < 20% of the reversal procedures being attempted laparoscopically. Complications related to late conversion to open surgery may suggest a selective use of the laparoscopic approach for Hartmann's reversal in a subgroup of patients: The aim of this study is to systematically investigate the literature to identify the ideal case for a laparoscopic approach.
Materials and Methods:
Data were extracted from a systematic review of the literature of Medline, Scopus, Web of Science, Embase, and the Cochrane Central Register of controlled trials. Subgroup analysis to identify suitable patients for laparoscopic surgery included age at surgery, body mass index, American Society of Anesthesiologists status, indication for the index Hartmann's procedure (HP), interval time to reversal from the index HP, conversion to open surgery, and temporary ileostomy rate.
Results:
A total of 862 patients were included, with 403 cases performed laparoscopically. Conversion to open surgery occurred in 65 patients (mean 16.1%). The indication for the HP showed a trend toward more benign patients included in the laparoscopic group, and the interval time between the index Hartmann's procedure and its reversal was significantly shorter in the laparoscopic group with a trend toward a higher rate of temporary ileostomy in patients undergoing an open procedure.
Conclusions:
Patients' selection can explain these differences, with more complex disease operated via an open approach. Nevertheless, future studies are needed to demonstrate an increasing number of reversals attempted laparoscopically in high-volume centers.
Introduction
H
Laparoscopic techniques for colorectal surgery have been evolving since the early 1990s, demonstrating benefits over open techniques in terms of shorter hospital length of stay, 8 less pain, and quicker return to full activities, 9 with the first laparoscopic Hartmann's reversal (LHR) being performed in 1993. 10
LHR offers reduced morbidity compared with the conventional open procedure while improving reversal rates as previously demonstrated11,12; however, it is one of the most technically demanding procedures in minimally invasive colorectal surgery, 13 with a further < 20% of the reversal procedures being attempted laparoscopically. 14 In fact, the procedure is also affected by a high conversion rate, which ranges from 0 to 50% (mean 16.1%), with most common reasons for conversion including adhesions, failed identification, or injury of the rectal stump.
Complications related to late conversion to open surgery 15 may suggest a selective use of the laparoscopic approach for HR in a subgroup of patients: The aim of this study is to systematically investigate the literature to identify the criteria to select an ideal case for a laparoscopic approach to this challenging surgical procedure.
Materials and Methods
Data sources and search strategy
Data were extracted from a systematic review of the literature 12 performed after the development of a review protocol in compliance with the meta-analyses of observational studies in Epidemiology guidelines for reporting meta-analysis of observational studies 16 ; a comprehensive literature search of Medline, Scopus, Web of Science, Embase, and the Cochrane Central Register of controlled trials was performed with no language, publication date, or publication status restrictions.
An extensive search was conducted by using the search terms: “Hartmann* or *stoma or ostomy or colostom*” and “mini invasive or mini-invasive or minimally invasive or laparoscop* or keyhole” and “reversal or restoration or closure or continuity or reconstruction.”
The reference list of the retrieved articles was searched to identify additional eligible studies.
Eligibility criteria and study selection
Inclusion criteria were as follows: (1) comparative studies evaluating patients undergoing LHR versus open Hartmann's reversal (OHR), (2) HR performed with standardized and well-described methodology, and (3) intention-to-treat analysis for the laparoscopic group (all procedures that started laparoscopically were included in the LHR group, even if converted). Studies including only hand-assisted, robotic, and single-incision laparoscopic surgery patients were excluded. Reviews were only checked to find further relevant studies, and when the same author and institution published the same case series in different articles, only the most recent paper was evaluated. For studies that reported insufficient data, the corresponding authors were contacted for further information.
Outcome analysis
The primary outcome was 30-day overall morbidity. Secondary outcomes were: 30-day mortality and 30-day complication-specific morbidity.
Subgroup analysis included: age at surgery, body mass index (BMI), American Society of Anesthesiologists (ASA) status, indication for the index Hartmann's procedure (HP), interval time to reversal from the index HP, conversion to open surgery, and temporary ileostomy rate.
Odds ratio (OR) and 95% confidence intervals (95% CIs) were used as summary measures for dichotomous outcomes, whereas Weighted Mean Difference (WMD) and 95% CI were used for continuous outcomes.
Statistical analysis was performed by using STATA 12 statistical software (STATA Corp, College Station, TX).
Results
Patients' characteristics
Thirteen studies17–29 were retrieved, including a total of 862 patients: 403 LHR (46.75%) and 459 OHR (53.25%). Conversion to open surgery occurred in 65 patients (mean 16.1%; range 0%–50%) and was reported in all the studies. Baseline patient populations are shown in Table 1.
Data are expressed as they were reported in the original study as:
Mean ± standard deviation,
Mean (range),
Median (range).
ASA, American Society of Anesthesiologists; ben:mal, benignant:malignant ratio; BMI, body mass index; CR, conversion rate; F, female; id, incomplete data; LHR, laparoscopic Hartmann's reversal; M, male; n, number; NR, not reported; OHR, open Hartmann's reversal; TTR, lag time to reversal.
Primary outcomes
No differences were demonstrated in 30-day mortality between LHR and OHR (OR, 1.13; 95% CI, 0.41 to 3.15). LHR was associated with a reduced overall postoperative 30-day morbidity compared with OHR, as reported in all the included studies (OR, 0.24; 95% CI, 0.17 to 0.34) (Figure 1).
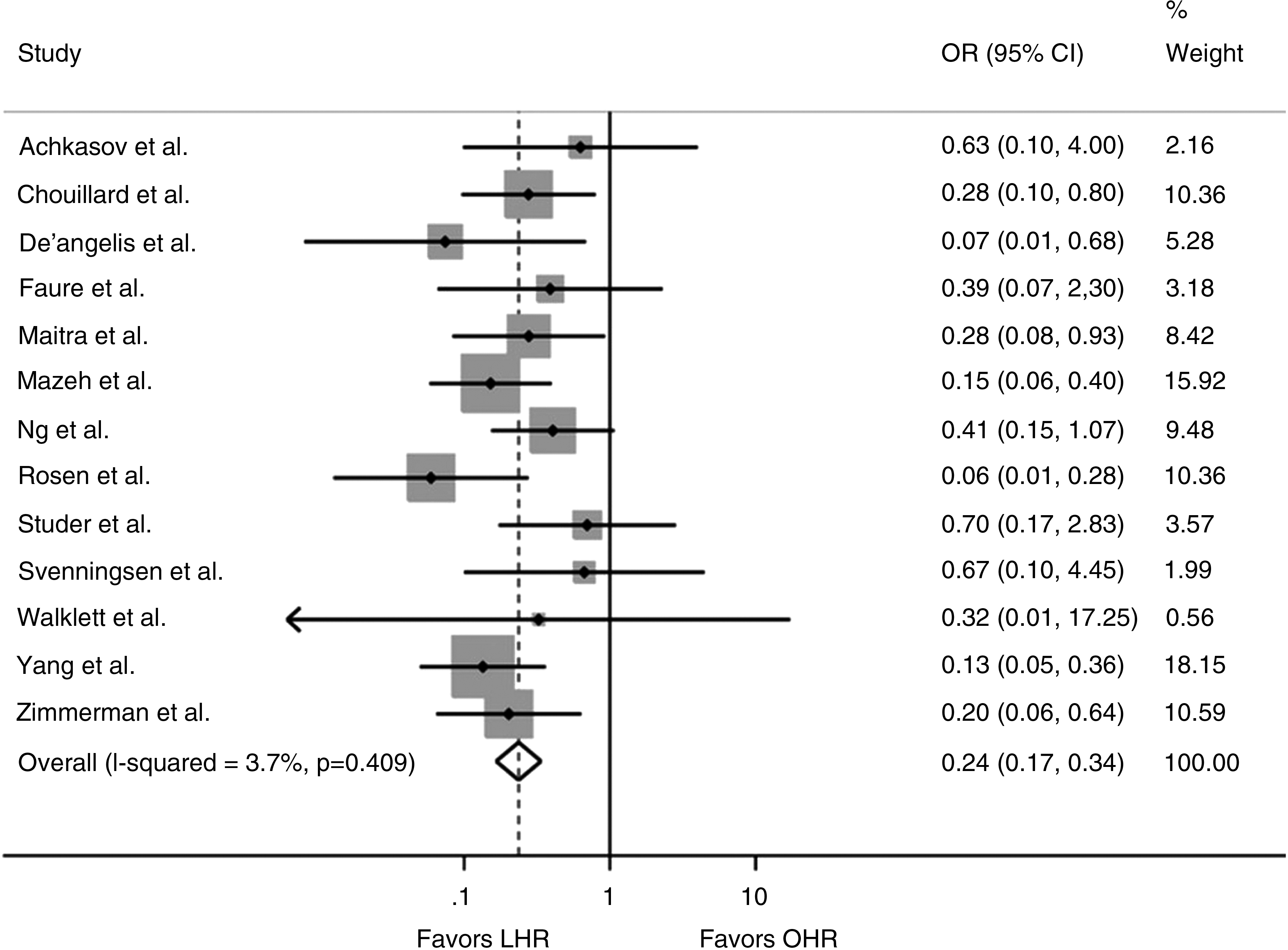
Forest plot comparing 30-day overall morbidity after LHR versus OHR. A fixed-effect model was used for meta-analysis. An OR <1 indicates a lower incidence of morbidity in the LHR group. 95% CI, 95% confidence interval; LHR, laparoscopic Hartmann's reversal; OHR, open Hartmann's reversal; OR, odds ratio.
Wound infection (OR, 0.54; 95% CI, 0.35 to 0.85; Q = 8.82; P = .64) and postoperative ileus (OR, 0.47; 95% CI, 0.25 to 0.87; Q = 6.72; P = .45) were more commonly observed in the open group, and no difference was found in the anastomotic leak rate between the two groups (OR, 0.42; 95% CI, 0.14 to 1.27).
Subgroup analysis and case selection
No difference was found between LHR and OHR populations regarding age (WMD, −0.57; 95% CI, −2.67 to 1.53), sex (OR, 1.15; 95% CI, 0.87 to 1.51), BMI (WMD, −0.41; 95% CI, −1.76 to 0.93), and ASA score ≥3 (OR, 0.85; 95% CI, 0.51 to 1.39). The indication for the HP (benign versus malignant) showed a trend toward more benign patients included in the laparoscopic group, but this did not reach statistical significance between the two groups (OR, 1.37; 95% CI, 0.95 to 1.99).
The interval time (months) between the index HP and its reversal was significantly shorter in the LHR group (WMD, −1.45; 95% CI, −2.45 to −0.45) (Table 2).
ASA, American Society of Anesthesiologists; ben/mal, benign/malignant; BMI, body mass index; NR, not reported; LHR, laparoscopic Hartmann's reversal; OHR, open Hartmann's reversal.
A trend toward a higher rate of temporary ileostomy was found in the OHR compared with LHR, as demonstrated in Table 3.
AL, anastomotic leak; BL, bleeding; IAC, intra-abdominal collection; LHR, laparoscopic Hartmann's reversal; n, number; NR, not reported; OHR, open Hartmann's reversal; Reop, reoperations; Resp, respiratory complications; WI, wound infection.
Discussion
The laparoscopic approach to the HR confirms the benefits of minimally invasive surgery demonstrated for other colorectal procedures.30,31 As previously reported, LHR is associated with reduced short-term morbidity compared with OHR 12 : Wound infections were significantly less commonly observed in the laparoscopic group, as it was postoperative ileus.
A reduced conversion rate has been advocated when the index HP is performed laparoscopically 18 ; however, the heterogeneity in the results across the studies could be attributed to a difference in laparoscopic technical skills among surgeons at different times of the learning curve. 32 As a matter of fact, the reversal is only performed by a minimally invasive approach in a reduced number of cases and not every surgical center has a significant case load. 33
It is important to note that some factors may lead to selecting a patient for a minimally invasive approach rather than a conventional open procedure at the time of reversal. When the index HP is performed for malignant disease, the interval between the HP and the reversal is longer and the procedure tends to be performed via an open approach. Only few studies reported on temporary ileostomy rate after HR; however, there was a clear trend toward performing more covering ileostomies when patients underwent open surgery. Patients' selection clearly explains these differences, with more complex disease attributed to an open approach, which is not unexpected, as HP is one of the most technically demanding procedures in minimally invasive colorectal surgery. Nevertheless, future studies may demonstrate a reduced patients' selection in high-volume centers.
In addition, other factors related to the index HP such as the surgical approach (laparoscopic versus open), the elective or emergency setting, and the Hinchey grade in case of diverticulitis may have influenced the surgical choice for the reversal; nevertheless, the impact of these potential, selection-determining factors on postoperative outcomes has to be demonstrated.
Our findings may lead to an increasing number of reversals being attempted laparoscopically; however, randomized controlled trials, with patients also stratified according to some characteristics of the primary resection (Hinchey grade, type of surgical approach), are mandatory before advising laparoscopic surgery as the gold standard technique for HR.
Conclusions
We advocate a selective approach to HR in dedicated minimally invasive colorectal units. When the index Hartmann's procedure is performed laparoscopically and the indication for surgery is benign disease, the reversal of Hartmann's procedure can be attempted laparoscopically with a high success rate. Randomized clinical trials are advised to confirm these findings.
Footnotes
Disclosure Statement
No competing financial interests exist.