
Abstract
Abstract
Introduction:
Implanting a magnetic lower esophageal sphincter augmentation device (LINX, Torax Medical) has become an increasingly common option in the surgical management of gastroesophageal reflux disease. As the enthusiasm for placing this device increases, experience in the management of device-related complications—including erosion—is necessary.
Methods:
We report a staged approach to LINX removal in a 64-year-old female with symptoms of odynophagia secondary to partial erosion of a LINX device into the esophagus.
Results:
The patient had a 12-bead LINX device placed in 2011 at an outside, international facility. In late 2013, she began experiencing symptoms of odynophagia. An esophagogastroduodenoscopy at our institution in October 2015 demonstrated two metallic beads eroding through the distal esophageal lumen. An elective endoscopic removal of the two visible beads was performed. A postoperative esophagram confirmed that there was no resulting esophageal perforation. The patient noted mild improvement in her symptoms. After a 12-week period to allow for complete healing, the remaining 10 beads of the LINX device were explanted laparoscopically without complication. No further procedures were undertaken. At 2 months' follow-up, the patient noted complete resolution of her symptoms.
Conclusion:
Transmural erosion of the LINX device into the esophageal lumen is a rare occurrence, with only five such complications reported in the published literature. We present the first account of LINX explantation for esophageal erosion in the United States. We demonstrated that a staged laparoendoscopic approach to LINX removal in these cases is feasible with minimal morbidity.
Introduction
G
The magnetic lower esophageal sphincter augmentation device (LINX, Torax Medical) emerged in 2008 as an alternative to conventional laparoscopic fundoplication for GERD. After initial feasibility studies demonstrated promising results, 7 the LINX device became FDA approved for the surgical treatment of GERD in 2012.
Multiple studies have reported comparable long-term efficacy compared with conventional surgical management for the LINX device in both symptom resolution and complication rates. At 5 years' follow-up, the initial feasibility study has reported an improvement in reflux-related quality of life in 94% of patients, with 88% of patients no longer requiring medical therapy and no major device-related complications. 8 Since that study, additional authors have reported similar excellent outcomes, with success in both prospective multicenter trials 9 and matched analyses. 10 Additional long-term studies have demonstrated that device-related complications are rare.11–13
However, as with any intervention, complications may occur and dysphagia requiring device explantation has been reported.14–16 Severe complications such as device erosion necessitating removal have been exceedingly rare, and the management of this complication has only been reported in a few reports in the international literature.14,17 As a result, little is known of the optimal management of a device that has eroded into the esophageal lumen.
We present our staged approach to the management of a case of device erosion at 4 years after LINX placement.
Case Report
We present the case of a 64-year-old female who initially presented to our institution in 2011 with symptoms of longstanding hoarseness, throat pain, and odynophonia. She also noted periodic atypical chest pain. She underwent multiple 24-hour pH testing to confirm the presence of GERD, but this study was within normal limits (nine episodes of reflux, none lasting >5 minutes, DeMeester score 11.5), and demonstrated little correlation between her symptoms and reflux. It was recommended that she not undergo surgical antireflux surgery. She sought a second opinion and in the spring of 2011 she subsequently underwent placement of a 12-bead LINX device at an outside facility. Her hospital course was complicated by persistent dysphagia, requiring prolonged parenteral nutrition for several weeks. After the procedure, however, she did note subjective improvement in her symptoms with normalization of her voice and resolution of throat pain.
In July 2013, she began to have recurrent odynophonia and subsequently she represented to the gastrointestinal service with complaints of pain with swallowing in December 2013. After a trial of conservative management, she underwent an esophagogastroduodenoscopy (EGD) in October 2015. In this study, two beads were identified in the distal esophageal lumen, consistent with partial device erosion.
Therapeutic Approach
Given the rarity of the complication and the lack of meaningful clinical experience with LINX erosion, we contacted the device manufacturer, who recommended a staged laparoendoscopic approach to device removal. A second EGD was performed 1 week later to extract the intraluminal portion of the device. Under general anesthesia, the patient was placed in a left lateral decubitus position and her cervical esophagus was easily intubated. The two beads were identified in the left lateral position at the lower esophageal sphincter (Fig. 1). The communicating wires on the outer ends of the beads were transected using a PolyLoop cutter (Olympus Corporation, Center Valley, PA). Magnets were placed into a Roth net (U.S. Endoscopy, Mentor, OH) and extracted (Fig. 2). Subsequent evaluation of the erosion site did not reveal any large full-thickness injury (Fig. 3). Nevertheless, the patient was admitted for observation and underwent an esophagram postprocedure to exclude occult perforation.
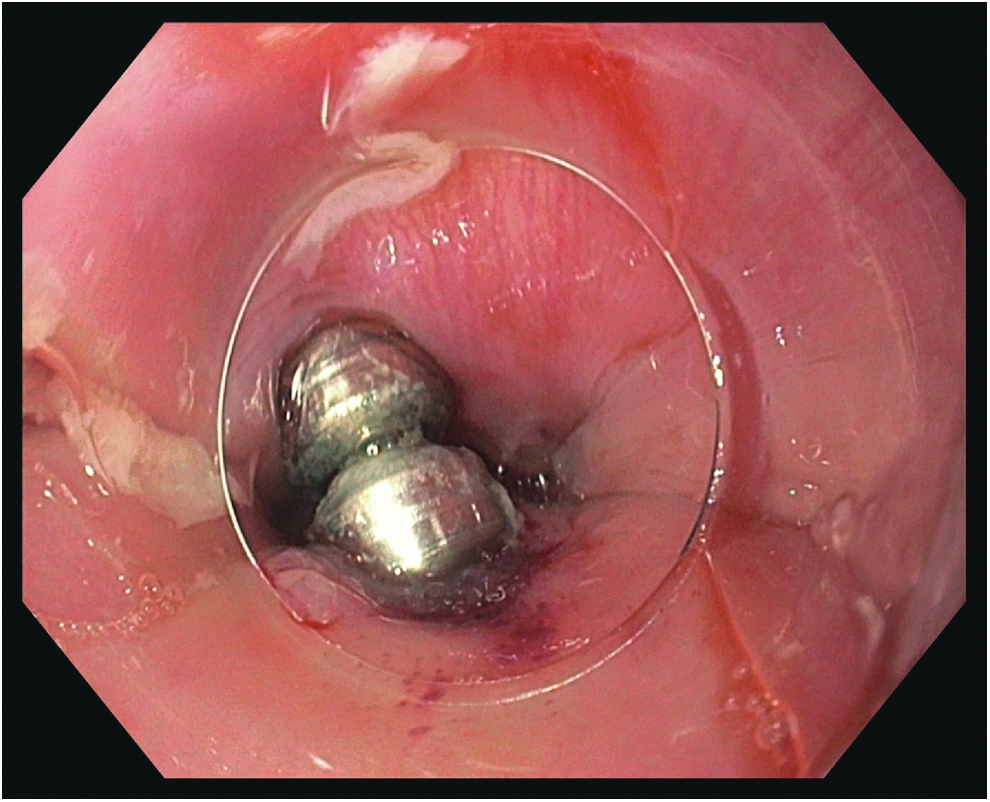
Endoscopic appearance of two magnetic beads of LINX device in the esophageal lumen.
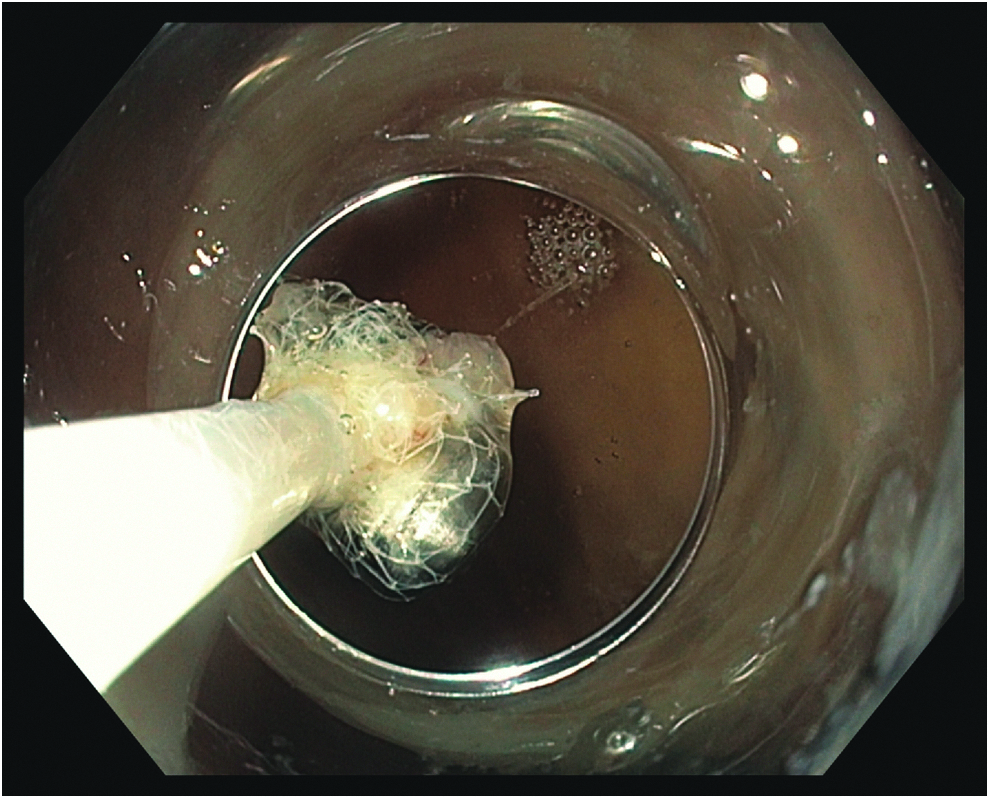
The magnetic beads were removed using a PolyLoop Cutter and placed in a Roth Net for extraction.

Postprocedure appearance of the esophageal mucosa.
After a 3-month period of recovery, the patient underwent laparoscopy to remove the remainder of the device. Under general anesthesia, she was placed in a modified lithotomy position and peritoneal access was gained using a Veress needle. Under direct observation, four additional 5 mm trocars were placed in a standard manner, and through a fifth port the liver was retracted to expose the gastroesophageal junction.
There were few dense adhesions along a capsule surrounding the device, which were transected using endoscopic scissor dissection and Bovie electrocautery. Once a portion of the device was seen, the 10 remaining beads were grasped and easily extracted out of its fibrous capsule en bloc. To ensure no perforation, a leak test was performed in a standard manner using saline and intraluminal insufflation. Next, the fibrous capsule surrounding the device was reapproximated using interrupted Vicryl sutures (Figs. 4a–d). A 10-French flat Jackson–Pratt drain was placed over the site of extraction. The next day the patient underwent a final esophagram, which once again confirmed no leak (Fig. 5).

Sequential operative steps of laparoscopic removal of the LINX device. First, the fibrous capsule surrounding the device was lysed

Postprocedure esophagram demonstrating no evidence for leak.
At 2 months' follow-up, the patient denied any symptoms of odynophagia nor any complaints of subjective reflux. She denied any difficulty swallowing or ongoing symptoms of reflux.
Discussion
As the LINX device becomes more broadly utilized, it is imperative to understand the optimal approach to management of rare but potentially devastating long-term complications such as esophageal erosion. We present the first published account of the management of LINX erosion in the United States. In our case, we elected to manage device erosion by first removing the visible endoluminal beads endoscopically and waiting 3 months before definitive removal. We heavily employed imaging studies to ensure no free esophageal perforation.
The optimal management of device erosion has not been standardized. In the initial experience with erosion, staged laparoendoscopic removal has been reported with excellent results. Lipham et al. in the earliest and largest assessment of 1000 cases identified partial device erosion in only 1 patient (0.1%). 13 In this case, the patient began experiencing dysphagia 20 months after implantation. An EGD subsequently demonstrated partial erosion into the esophageal lumen, and as in our case, the visible beads were initially removed endoscopically. After a 90-day healing period, the remainder of the device was removed laparoscopically.
Another German study suggested that a single endoscopic approach to device erosion might be feasible. 17 In that case report, a 59-year-old female began experiencing symptoms of odynophagia after device placement, and subsequent EGD demonstrated, as in our case, two-bead erosion into the lumen. However, instead of pursuing a staged approach, the patient was managed with biweekly serial endoscopies, at which point additional beads were noted to erode into the lumen. After 1 month of such management and four visible beads intraluminally, the patient was unable to tolerate further medical management. She underwent a totally endoscopic explantation of the device without complication.
Finally, a totally laparoscopic approach to device explantation for esophageal erosion has also been described. Asti et al. published their experience of 164 cases of LINX device placement, documenting 2 cases of device erosion (1.2%). 14 Both patients (both with endoscopic evidence for three-bead erosion) were managed with a single-stage laparoscopic operation. The patients progressed well without complications.
Our case typifies previous reports that regardless of approach—totally endoscopic, totally laparoscopic, or staged—the management of LINX device erosion can be performed with minimal morbidity and mortality rates. Remarkably, none of the patients in these published reports of device erosion suffered significant sequelae from this complication, likely because of the thick fibrous capsule that develops once the device is implanted. Although this may be subject to publication bias, these cases are instructive that regardless of approach, a high index of suspicion for free perforation must be maintained, and a low threshold for imaging studies should be employed. In addition, our study highlights the need to improve education on potential device-related complications. Finally, we present specific technical details that can be applied by practitioners to explant a device in the future.
The LINX device has the revolutionary potential to minimize the morbidity and mortality rates of surgical therapy for reflux disease. However, as the application for these devices expands, knowledge on the optimal management of device-related complications must be disseminated. Our study adds to the existing literature on the technique and outcomes of device removal by presenting the second successful staged removal of an eroded LINX device. Practitioners may use the information presented here to approach this incredibly rare, but potentially devastating, complication.
Footnotes
Disclosure Statement
No competing financial interests exist.