
Abstract
Abstract
Purpose:
Benign masses of the eyebrow and forehead are common in pediatric patients and can result in facial asymmetry, discomfort, or super-infection. Excision is classically conducted via an incision directly over the mass, which can produce sub-optimal cosmesis. Recently, an endoscopic approach using pediatric brow-lift equipment has been adopted. We reviewed our center's experience with endoscopic removal of benign facial lesions and compared these cases with an equivalent series of open cases.
Materials and Methods:
A retrospective chart review was conducted to identify pediatric cases of endoscopic and open removal of benign eyebrow or forehead lesions at our institution from 2009 to 2016. Clinical and cosmetic outcomes were reviewed.
Results:
A total of 40 endoscopic and 25 open cases of excision of benign facial lesions in children were identified. For the patients who underwent endoscopic excision, the majority (85%) presented with a cyst located at the eyebrow. Histologic examination revealed 36 dermoid cysts (90%), 2 epidermal cysts, and 2 pilomatrixomas. Of the 36 cases with post-operative follow-up, 32 patients (89%) had an uncomplicated recovery with good cosmesis. Two patients had an eyebrow droop that resolved without intervention. One patient had localized numbness overlying the site, but no motor deficits. One patient presented with a recurrent dermoid cyst that required open resection. For the patients who underwent open excision, the majority (52%) had dermoid cysts located at the eyebrow. Of the 22 cases with follow-up, 20 of the patients had an uncomplicated recovery (90%). Comparing the rate of complications, there was no statistically significant difference between the two groups (P = 1.0).
Conclusion:
Endoscopic excision of benign forehead and eyebrow lesions in pediatric patients is feasible and yields excellent cosmetic results. When compared with open excision, complication rates are similar between both approaches and a facial scar can be avoided with an endoscopic approach.
Introduction
B
Alternatively, an endoscopic approach to excision, first described in the plastic surgery community by Ramirez for brow-lift and face-lift, has recently been adopted. 5 The first case series describing the application of this endoscopic approach to excision of benign masses of the eyebrow and forehead in children was reported by Dutta et al. in 2006. The authors described 9 cases of successful endoscopic excision, demonstrating that this procedure can be safely and effectively pursued by pediatric general surgeons. 3 This technique has since been pursued, with promising results in both pediatric and adult patients at a number of other institutions across the world. 6 The total number of pediatric cases reported in the literature, however, remains small.
Overall, endoscopic excision of benign facial masses can be successfully conducted in pediatric patients with favorable outcomes. The purpose of this study was to evaluate our institution's ongoing experience using this technique. In this case series, we report our outcomes from endoscopic cases, including complications and patient satisfaction, in comparison with a cohort of patients who underwent open excision.
Materials and Methods
We conducted a retrospective chart review of both endoscopic and equivalent open excisions of benign facial masses in pediatric patients less than 18 years of age from 2009 to 2016. All operations were performed at Lucile Packard Children's Hospital at Stanford by surgeons within the Divisions of Pediatric and/or Plastic Surgery. The study received approval from the Stanford University Institutional Review Board (IRB). Both endoscopic and open approaches were discussed with the patients and their families before surgery. The risks and benefits of each technique were explained, as well as the possible need to convert to an open approach if endoscopic access could not be achieved in those who selected the endoscopic approach. The families of all patients provided informed consent for the operation.
A standard surgical technique was used in all cases. Patients underwent general endotracheal anesthesia for the procedure. Pre-operative antibiotics were administered as per hospital protocol. Povidone-iodine solution was used to clean the surgical site. For the endoscopic approach, the hair was washed at the site of incision and patients were administered a local anesthetic, most commonly 0.25% bupivacaine, that was injected directly into the incision site. A 1–2 cm incision was made above the hairline. A periosteal elevator was used to access the subgaleal plane, and a combination of direct and hydro-dissection was employed to tunnel a channel for endoscopic access of the mass (Figs. 1–3). The tunnel was irrigated and examined for hemostasis (Fig. 4). For the open approach, an incision was made directly over the mass. In all cases, the mass was excised and submitted to pathology for routine analysis. The incision was closed with absorbable suture.

Subgaleal tunnel dissection.
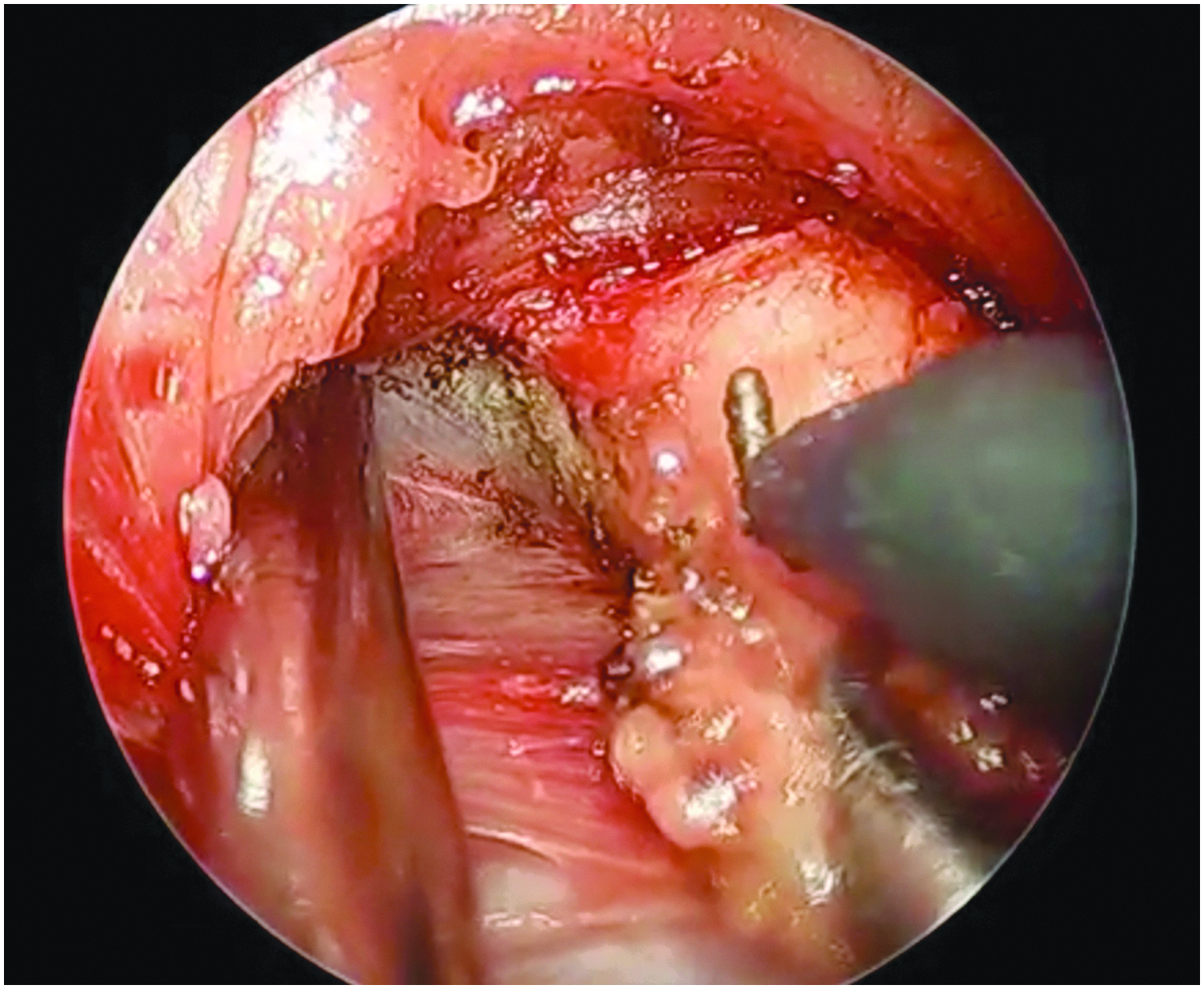
Cyst dissection with hook electrocautery.
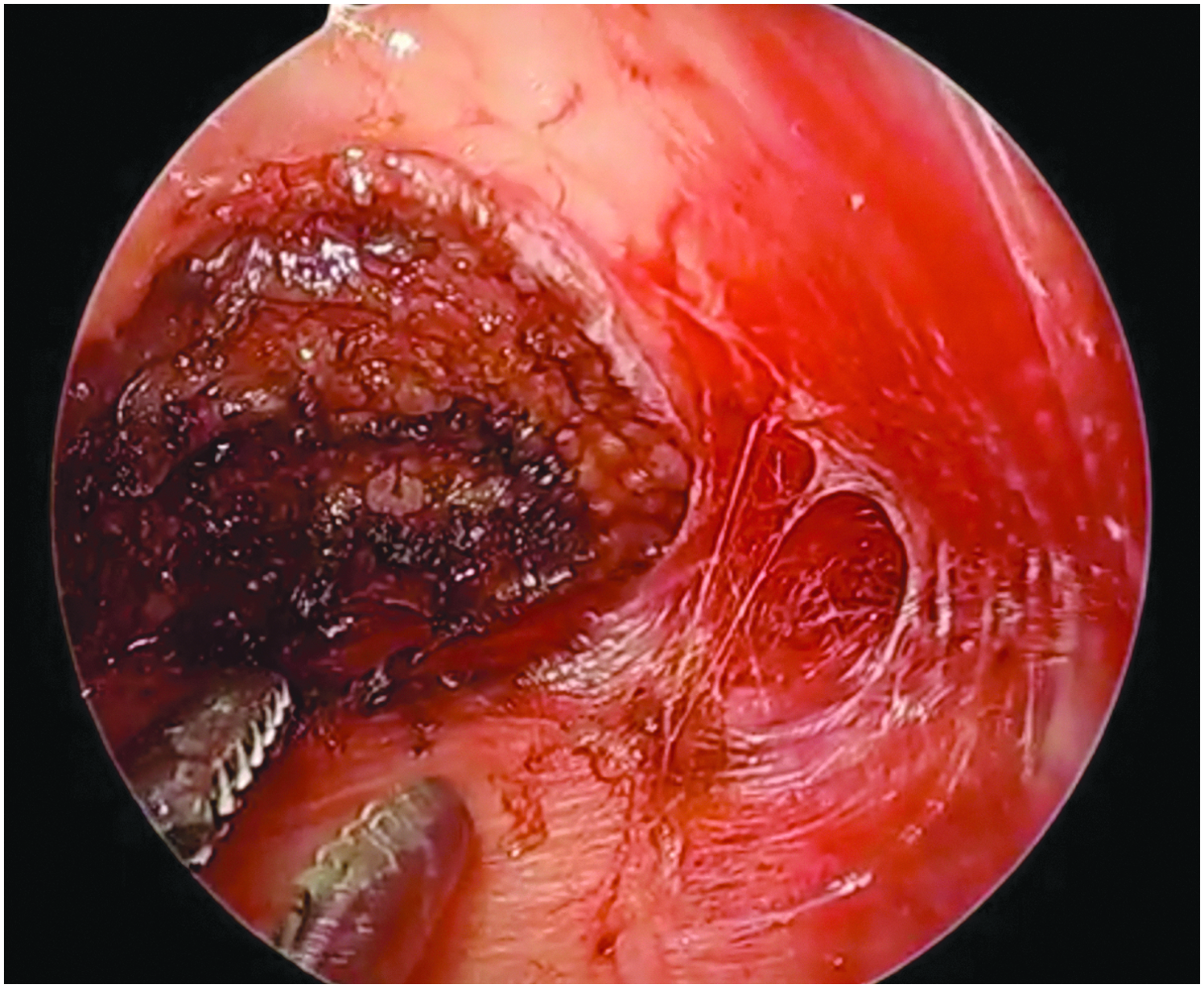
Cyst cavity after excision.
Patient data were collected, including demographic information, pre-operative imaging, procedure details, complications, pathology, cosmetic outcomes, and recurrence. Data were analyzed with descriptive statistics and the following statistical tests: Fisher's exact test was used to compare proportions of variables, t test was used to compare categorical variable means between the two groups, and a P value <.05 was considered statistically significant. Statistical tests were performed by using GraphPad Prism version 6.00 for Mac (GraphPad Software, La Jolla, CA).
Results
A total of 40 relevant endoscopic cases were identified and included in the analysis. The average age of patients was 2.1 years (range 1 month–13.8 years). Twenty-five patients (63%) were male, whereas 15 (38%) were female. The majority of patients (85%) presented with a mass located at the eyebrow (20 on the left, 14 on the right). Two patients had a mass in the right periorbital region, 2 had a forehead mass, and 2 had a nasal bridge mass. Reasons for electing to pursue excision included risk of infection or observation that the lesion was rapidly enlarging, resulting in cosmetic concerns. On pre-operative assessment, most of the patients were noted to have mobile masses; however, 5 patients underwent pre-operative imaging (2 ultrasounds, 2 magnetic resonance imaging, and 1 plain film) to evaluate for possible deep involvement or intracranial extension. The surgery was performed as an outpatient procedure in all but 2 cases. Patients were observed in the post-anesthesia care unit until stable and then discharged home the same day. One patient was admitted for post-operative observation overnight due to young age (1 month old); the second patient was admitted because of young age (5 months old) and concern for post-operative pain, having undergone excision of multiple lesions on the head and torso during the same operation.
In 26 of the 40 cases reviewed (65%), the cyst was removed intact. In the remaining cases, the cyst either spontaneously burst during dissection or was punctured purposefully to facilitate removal. In all cases, the cyst wall was removed completely. Histologic examination of the lesions revealed dermoid cysts in 36 of the 40 cases (90%), pilomatrixoma in 2 cases, an epidermal inclusion cyst in 1 case, and an epidermoid cyst in 1 case.
Four patients were lost to follow-up. Of the 36 cases who had documented post-operative follow-up, 32 patients (89%) had an uncomplicated recovery with good cosmesis. Two patients were found to have an eyebrow droop post-operatively. In both patients, this resolved without intervention. One patient was noted to have localized numbness of the skin overlying the site of prior pilomatrixoma that self-resolved, but no motor deficits. One patient had an uncomplicated recovery after excision of a dermoid cyst, but it presented again 1 year later with a recurrent mass. The patient underwent an open re-resection and recovered uneventfully. Patients and their families were satisfied with the outcome in all cases.
For the purpose of comparison, 25 cases of open excision of benign facial masses from our institution were selected and analyzed. Open cases were selected for inclusion only if they could have also been approached endoscopically. Of this cohort, the average age was 5.3 years, with a range of 1 month to 17 years old. Eleven patients were male (44%), and 14 were female (56%). Most patients (92%) had a mass in the region of the eyebrow (15 on the right side, 8 on the left side). One patient had a dermoid within the eyelid, inferior to the orbital rim and 1 patient had a temporal lesion.
Pre-operatively, the primary reason for excision was growth of the lesion with related cosmetic concerns. Three of the 25 patients in this cohort underwent pre-operative imaging (two ultrasounds and one head CT scan). The cyst was removed intact in 14 (56%) of cases. In all cases, the cyst wall was removed completely. On pathology, 13 of the 25 specimens (52%) were dermoid cysts, 9 (36%) were pilomatrixoma, and the remaining 3 (12%) were epidermal inclusion cysts. All 25 patients were discharged home on the same day as their surgery.
Within this group, there were 3 patients who were lost to follow-up. Of the 22 patients who did follow-up post-operatively, 20 patients (90%) had an uncomplicated recovery. One patient had a slight eyebrow droop that also resolved spontaneously, and 1 patient had spots of hypopigmentation within the scar.
Comparing the two groups, there was a difference in the mean age of the two groups, with the cohort that underwent endoscopic surgery being significantly younger (t-test, P = .004). There was no difference between the proportion of cysts located on the brown versus other locations between the two groups (Fisher's exact test, P = .47), nor was there a difference between the groups in terms of the proportion of children who had their cyst removed intact (Fisher's exact test, P = .60). There was a significant difference between the cohorts in terms of the proportion of dermoid cysts to epidermal cysts or pilomatrixomas (Fisher's exact test, P = .0003). Comparing the rate of any complications between the endoscopic and the open cohorts, there was no statistically significant difference (Fisher's exact test, P = 1.0) (Table 1).
S.S., statistically significant; N.S., not significant.
Discussion
Endoscopic excision of benign facial masses in children can be successfully conducted by pediatric surgeons and is often pursued at our institution for resection of these lesions. In our case series, all the patients had excellent cosmetic results after endoscopic excision with no long-term complications. When compared with open excision, there was no significant difference in post-operative outcomes. However, there was 1 patient in the open excision cohort who had notable hypopigmentation associated with the scar over the surgical site. This might have been avoided with an endoscopic approach. Overall, these results support our practice of offering endoscopic resection to pediatric patients with benign facial lesions.
In our experience, pre-operative imaging is not required in the vast majority of cases, particularly if the lesion is lateral and mobile on exam. In a prior case series, ultrasound or MRI was pursued pre-operatively in all cases to assess for deep involvement; however, endoscopic excision was still pursued in all cases. 2 In general, pre-operative imaging has been reserved for non-mobile, midline, nasoglabellar lesions with concern for possible intracranial extesion.3,7 Nasoglabellar lesions comprise less that 3% of facial masses and are still amenable to endoscopic excision in some cases. 8 In our series, 2 patients received pre-operative imaging; pre-operative imaging did not change management or outcome in any of the cases.
Given the relative novelty of this approach to excision of benign facial lesions, the operative technique has varied in the reported case series. Some centers have described pursuing the endoscopic dissection in the sub-periosteal plane whereas the subgaleal plane is used in other cases as described here. 6 The subgaleal plane is slightly more superficial and, in our experience, easily accessible for this procedure. In other studies, two, 9 three, 2 or even four 10 ports have been used to pursue the technique. In our experience, a single endoscopic port technique is feasible and preferable to further minimize the risk of post-operative scarring.
We observed no negative outcomes in patients with rupture of the cyst during excision. In all cases, both endoscopic and open, the whole cyst was removed. Previous studies have suggested that incomplete cyst excision may increase the risk of recurrence. 8 One patient in this series developed a cyst recurrence; in that case, the cyst was removed intact.
Despite our encouraging results, there are risks associated with endoscopic excision of benign facial lesions. The major risk is the possibility of injury to a facial nerve branch or other local nerve that could lead to muscle weakness or sensory changes. The incidence of this complication is very low in the literature. Two of the patients in the endoscopic patient cohort in our study developed a temporary eyebrow droop post-operatively that resolved without intervention. One patient from the open cohort also experienced this temporary result. These symptoms were likely secondary to post-surgical edema or nerve stretching that resolved spontaneously over time. To minimize the risk of nerve injury during endoscopic excision, care should be taken intra-operatively to stay in the appropriate plane during dissection and particular attention should be paid to the medial locations of the supraorbital and supratrochlear nerves and the facial nerve branches laterally. 7 In general, satisfaction with the endoscopic approach from both the surgeon and patient perspective has been reported to be very high. 11
Conclusion
An endoscopic approach to the excision of benign forehead and eyebrow lesions in pediatric patients is feasible and yields excellent cosmetic results. When compared with open excision, complication rates are similar between both approaches, and a facial scar can be avoided with the endoscopic approach.
Footnotes
Disclosure Statement
No competing financial interests exist.