
Abstract
Abstract
Introduction:
We previously developed a porcine model of long gap pure esophageal atresia (EA) to aid in the creation of novel devices and techniques for treatment of EA. Shortcomings of the model included difficulty decompressing the proximal esophageal pouch (leading to recurrent aspiration) and a requirement for gastrostomy tube (G-tube) feeds. Therefore, we sought to create a porcine model with a bifurcated esophagus wherein one portion of the esophageal lumen retained patency and the other part mimicked EA.
Methods:
After G-tube placement, thoracotomy was performed with subsequent partial stapled transection of the esophagus in a transverse manner, followed by longitudinal, partial stapled transection of the esophagus proximally and distally. Magnets were placed in the esophageal pouches.
Results:
Proximal and distal esophageal pouches were created while preserving a parallel, narrower segment of continuous esophagus. G-tube feeds were used initially, but the animal ultimately tolerated full nutrition by mouth. The magnets successfully restored esophageal continuity. The animal regained much of the initial weight lost and survived to planned euthanasia. Necropsy revealed anastomosis formation without evidence of leak.
Conclusions:
A bifurcated porcine esophagus model was successfully devised, simulating EA while allowing the animal to receive oral feeds and clear oral secretions. This model is anticipated to promote animal well-being and ease of care during future investigations, as well as a platform for the safe development of new therapies for EA.
Introduction
O
Herein, we detail the successful creation of a bifurcated porcine esophagus to serve as an improved animal model for EA. Furthermore, we demonstrate its robustness by subsequently restoring esophageal patency using a magnetic device.
Materials and Methods
Animal experimental protocols were approved by the Case Western Reserve University Institutional Animal Care and Use Committee (IACUC protocol 14-0052).
Esophageal pouch creation
A female domestic swine (Sus scrofa domesticus) ∼5 months of age (68.2 kg) was used for the study. Tulathromycin (2.5 mg/kg, intramuscular [IM]) was administered upon arrival to the laboratory (8 days before surgery). Omeprazole (20 mg daily, per os [PO]) was started 2 days before surgery.
Sedation (Telazol, 6 mg/kg, IM) was performed before endotracheal intubation. Anesthesia was maintained with isoflurane (1.5%–3.0%, titrated to effect) and mechanical ventilation (100% O2). Pulse oximetry, end-tidal CO2, respiratory rate, temperature, and airway pressure were monitored intraoperatively. Fluids were administered (through an aural intravenous catheter normal saline, 12.5 mL/(kg·hr)). Antibiotic (enrofloxacin, 5 mg/kg, IM), analgesic (buprenorphine, 0.03 mg/kg, IM), and other medications were given (carprofen, 4 mg/kg, subcutaneous [SC]; famotidine, 0.2 mg/kg, IM; ondansetron, 0.15 mg/kg, intravenous [IV]; atropine, 0.04 mg/kg, IV).
Standard technique was used to place a 24-Fr MIC Safety (Kimberly-Clark, Irving, TX) percutaneous endoscopic gastrostomy (PEG) tube. A Carter–Thomason suture passer (Cooper Surgical, Trumbull, CT) was used to place three transfascial 2-0 Monosof (Medtronic, Dublin, Ireland) sutures to fix the stomach to the abdominal wall.
A right thoracotomy was performed with the animal in the left lateral decubitus position. The incision site was two rib spaces below the tip of the scapula. Local anesthetic was administered along the planned incision line (bupivacaine, 0.5 mg/kg, SC) and paralytic was administered (rocuronium bromide, 0.2 mg/kg, IV). The esophagus was generously dissected both superiorly and inferiorly using electrocautery, with a vessel loop aiding in manipulation of the esophagus and care was taken to avoid injury to the anterior and posterior vagus nerve branches.
A modified orogastric tube (OGT) was created by cutting an ∼15-cm segment from the end of an 18-Fr OGT. This was reattached to the OGT with suture to create a “hinged” segment that could be oriented to create two parallel tubes (Fig. 1). This tube was subsequently placed into the esophagus with the two tube segments in parallel. A halfway point of the exposed esophagus was selected for partial transection. The presence of longer OGT prevented the stapler from being placed completely across the esophagus (whereas the shorter tube segment was distal to this point), thereby ensuring that a patent lumen (henceforth identified as the “common channel”) would be preserved. An Endo GIA Universal Roticulator stapler with a 60-mm purple TriStaple load (Medtronic, Dublin, Ireland) was fired in a transverse manner for partial transection of the esophagus (Fig. 2).
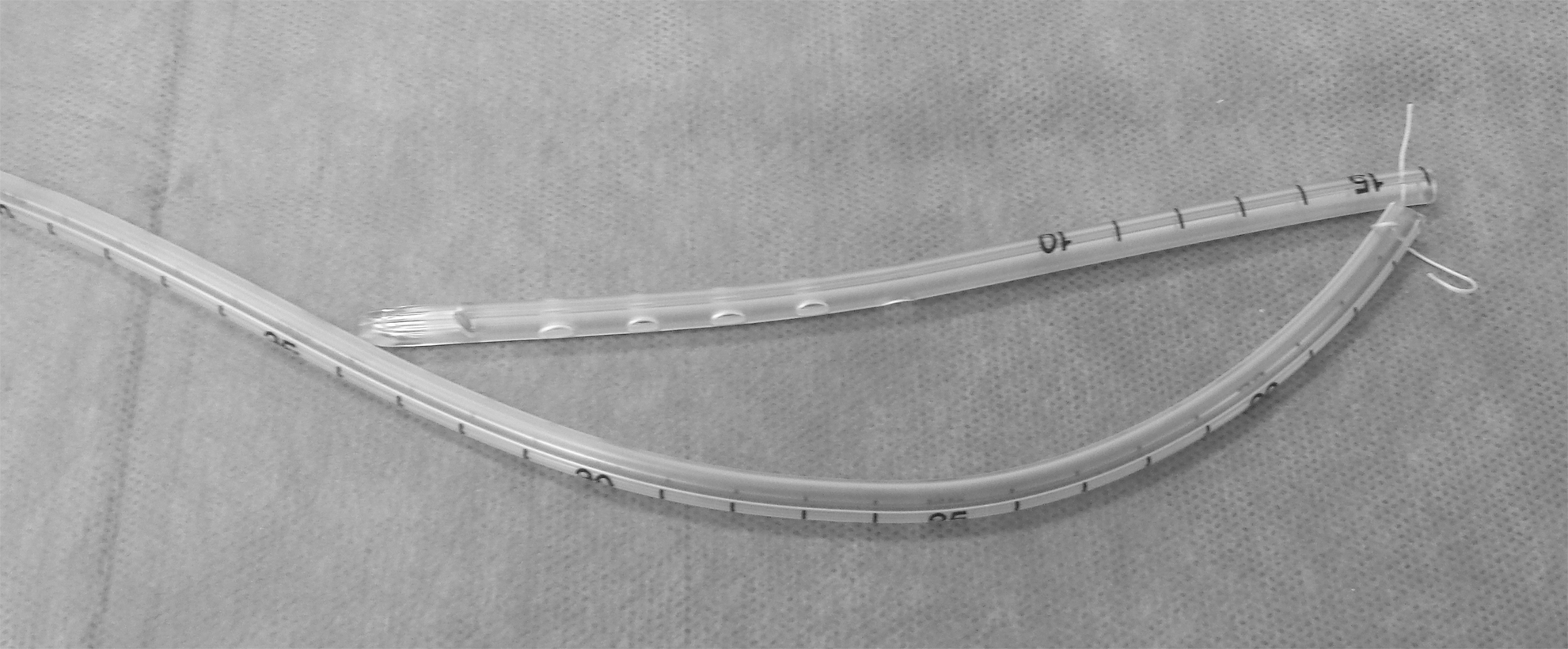
The modified orogastric tube with “hinged” segment was used to create two patent, parallel esophageal lumens.
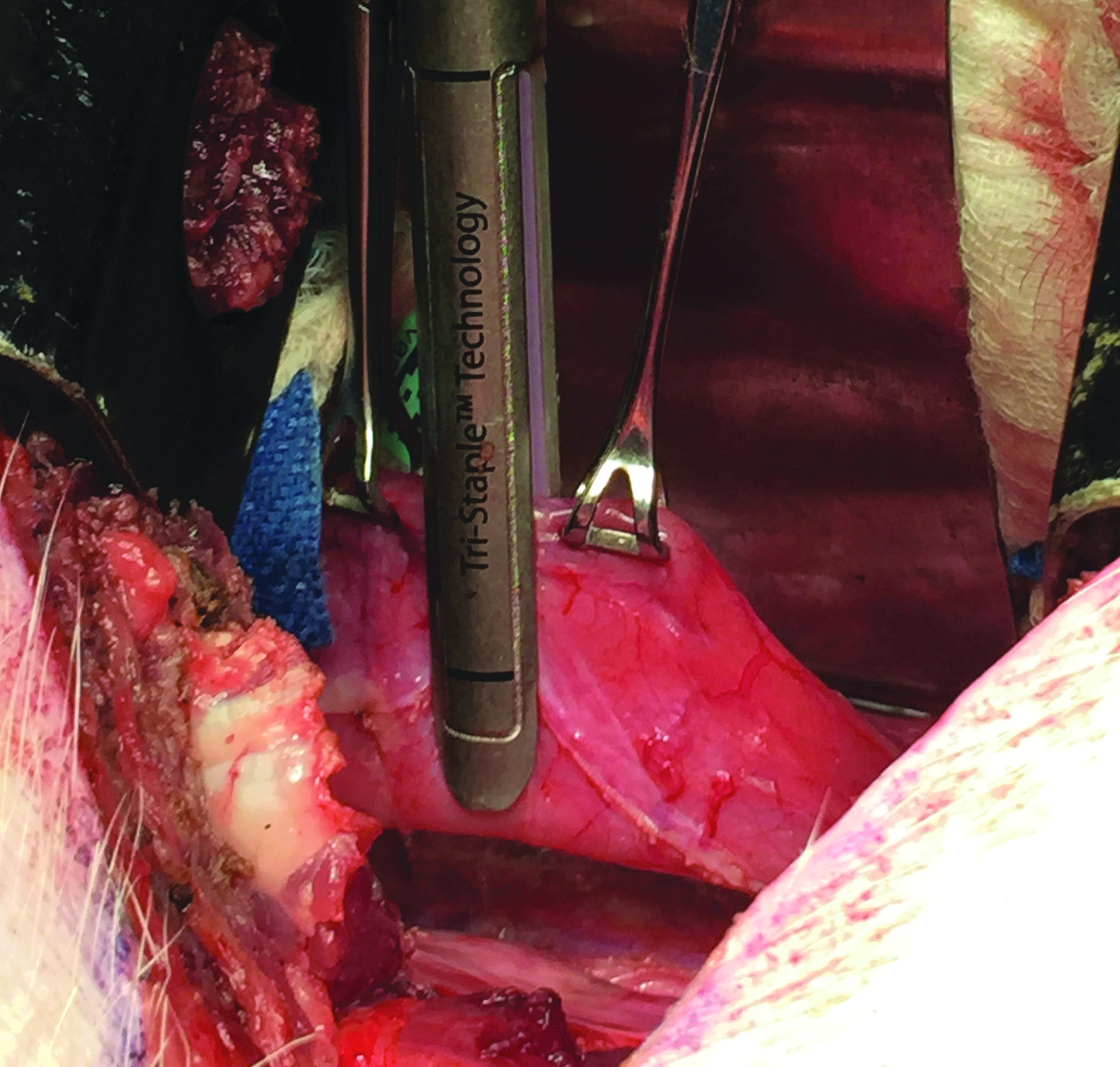
The stapler is fired transversely to partially transect the esophagus. An intraluminal orogastric tube prevents complete transection of the esophagus and allows for creation of the common channel.
Next, the distal esophageal pouch was created. The modified OGT was withdrawn such that the longer segment of OGT would occupy the common channel and the shorter segment would define the distal pouch. The stapler jaws were oriented between the two tubes and the esophagus was palpated to ensure that the short OGT segment was abutting the distal staple line and the longer OGT remained in the common channel (Fig. 3). A purple stapler load was then fired in a longitudinal manner, creating an ∼3-cm staple line, and the modified OGT was removed.
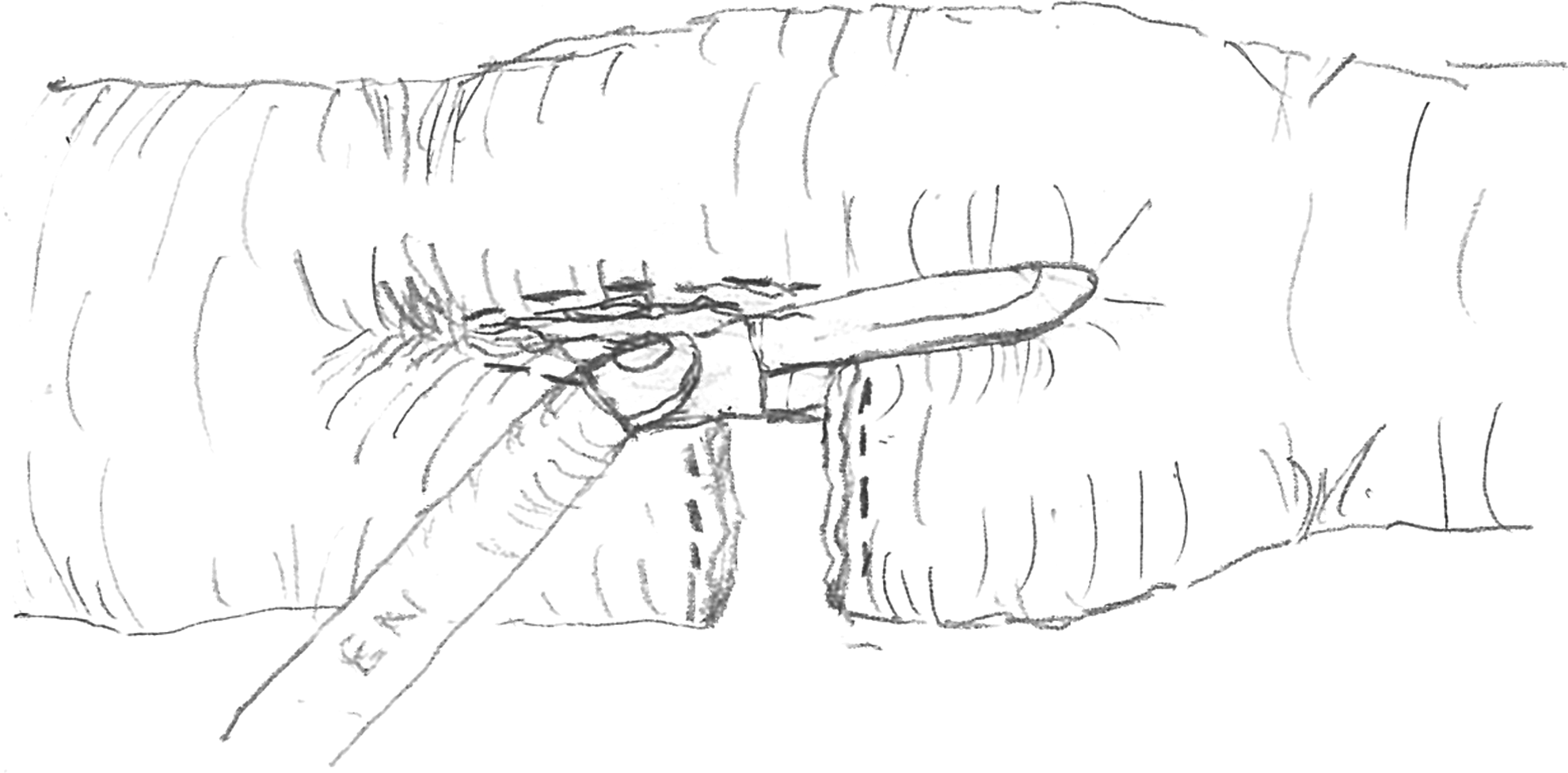
The stapler is fired longitudinally to create the proximal esophageal pouch.
Similarly, a 3-cm proximal pouch was created using two parallel, full-length OGTs in the proximal esophagus. The newly created distal and proximal esophageal pouches (Fig. 4) were carefully affixed in proximity to one another, creating an ∼1.5-cm gap.
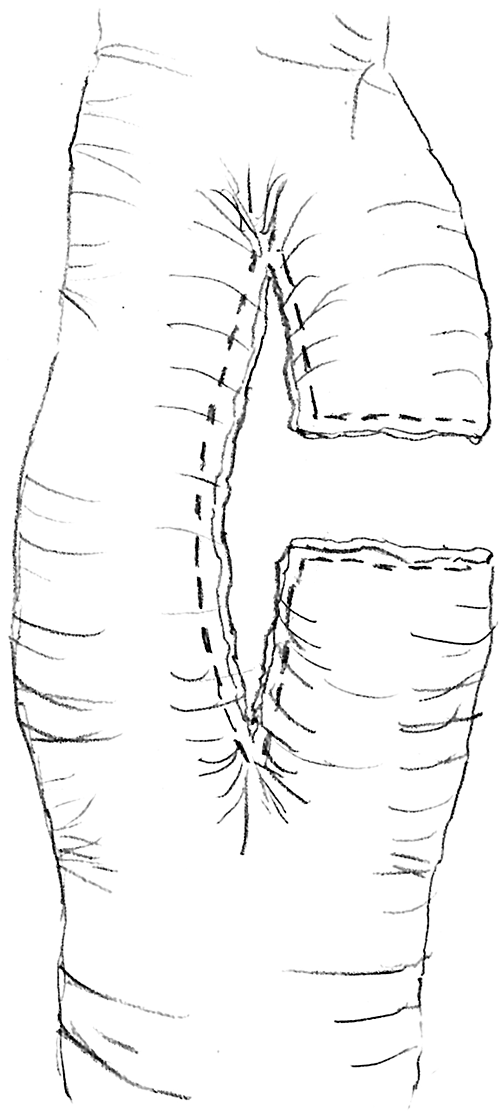
After three firings of the stapler, proximal and distal esophageal pouches have been created. The common channel can also be seen.
A leak test was performed by filling the right hemithorax with sterile saline and gently insufflating the esophagus using the endoscope.
A 24-Fr chest tube (Medtronic, Dublin, Ireland) was placed through a separate stab incision in the right posterolateral chest.
The ribs were reapproximated using #1 Maxon suture (Medtronic). Muscle and fascia were closed using 2-0 Polysorb (Medtronic), and the skin was closed with 3-0 Polysorb. The PEG tube and chest tube were secured to the skin and positioned between the scapulae for easy access. A protective cloth vest was placed on the animal. A Heimlich valve (Becton, Dickinson and Company, Franklin Lakes, NJ) was secured to the chest tube and the animal was weaned from ventilation, recovered, and returned to her pen. Food, water, and edible enrichments were withheld.
Postoperative medication included butorphanol (0.3 mg/kg, SC, daily [QD] for 4 days) upon recovery, buprinex (0.03 mg/kg, per rectum [PR], every 12 hours, pro re nata), omeprazole (20 mg, through PEG tube, QD for 6 days), carprofen (4 mg/kg, SC, QD for 4 days), famotidine (0.2 mg/kg, IM, every 12 hours [Q12H] for 4 days), ondansetron (0.15 mg/kg, IM, Q12H for 6 days). The pig was given a small volume of water through the PEG tube on the evening of surgery and then a water-soluble liquid diet (TD 120151; Envigo, Madison, WI) was gradually introduced during the 3–4 daily feedings to a goal of 1000 mL of tube feed through PEG tube three times daily.
The chest tube was removed on postoperative day (POD) 3.
Magnet placement
On POD 10, the pig was again anesthetized and intubated using the same procedure as for the initial surgery. The esophagus was intubated with an overtube (US Endoscopy, Mentor, OH) to facilitate repeated endoscopy and magnet placement. A pediatric, flexible endoscope with 8.5-mm outer diameter (Olympus GIF-P140; Tokyo, Japan) was inserted and used to identify the proximal esophageal staple line and common esophageal channel.
Fluoroscopy with barium was used to assess for patency as well as determine the gap between the esophageal pouches.
To place the distal esophageal pouch magnet, the PEG tube was removed and a second pediatric, flexible endoscope with 5.9 mm outer diameter (Olympus XP-160) was placed into the stomach through the gastrostomy. This distal scope was advanced retrograde through the lower esophageal sphincter and into the distal native esophagus. To advance this scope into the distal pouch, a snare was inserted into the working channel (with the sheath of the snare removed so it would fit through the 2.0 mm channel). This snare was advanced cephalad through the common channel and grasped through the proximal scope, and the distal scope was subsequently brought out of the pig's mouth. A 1/5″ × 1/4″, DH24-N42 magnet (K&J Magnetic, Pipersville, PA) was placed into the snare and the loop of the snare was drawn tightly to the tip of the distal scope, securing the magnet. The distal scope was carefully withdrawn into the distal esophagus and then the snare and magnet were advanced into the distal pouch. The location was verified by fluoroscopy. The proximal scope had a foreign body retrieval net (Roth net; US Endoscopy, Mentor, OH) placed into its working channel and a magnet of the same size was placed into the net. The scope was inserted into the proximal pouch, again with fluoroscopic verification. Owing to lack of adequate visual indication of attractive forces, the proximal magnet was exchanged for a stronger magnet (5/16″ × 3/8″ cylinder, D58-N52; K&J Magnetic). By withdrawing the snare, the distal magnet could be released into the distal pouch. By forcefully retracting the Roth net with the magnet inside the net, the magnet tore through the net and was thus deployed into the proximal pouch. Fluoroscopic images were recorded upon initial magnet placement (Fig. 5) and ∼5 minutes later.

Fluoroscopy reveals the proximal (larger) and distal (smaller) esophageal magnets shortly after placement. The proximal endoscope is visible.
A 24-Fr Foley catheter was placed into the gastrostomy site to continue tube feeds.
On POD 13, TID tube feeds were stopped in favor of twice daily PO liquid feeds consisting of the same formula, which was previously given through a PEG tube.
On POD 16, the pig was again anesthetized and intubated. Fluoroscopy was performed, followed by endoscopy and a barium fluoroscopy study.
On POD 21, endoscopy and barium fluoroscopy were performed. The magnets were retrieved endoscopically by placing a third magnet in a Roth net, advancing the net, and allowing the magnetic force to engage the implanted magnet pair. The Roth net was withdrawn carefully, under fluoroscopic guidance, thus removing both the proximal and distal magnets simultaneously.
Barium contrast imaging was repeated to assess the newly formed anastomosis and resultant stricture.
In an attempt to enlarge the anastomosis (thereby relieving the stricture), larger magnets were placed across the stricture. Using an endoscope and Roth net, the distal magnet was placed from above, through the common channel, into the distal esophagus, just beyond the point of distal pouch bifurcation. Then, a snare (stripped of its plastic sheath) was placed across the anastomosis into the distal pouch, under fluoroscopic guidance. The distal magnet was attracted to the snare and the snare could be withdrawn to pull the magnet into the distal pouch. Using the wire as a magnetic “track,” the proximal magnet was pushed with the tip of the endoscope along the snare down the esophagus into the proximal pouch. The snare was removed, followed by the endoscope. Fluoroscopic images verified the position of the magnetic pair across the stricture.
On POD 27, awake barium fluoroscopy was performed by adding barium to the animal's feed.
On POD 29, the animal underwent planned euthanasia (pentobarbital overdose) followed by endoscopy and barium fluoroscopy before necropsy.
Results
Animal welfare
The course of recovery from anesthesia was unremarkable and the pig was returned to her pen ∼2 hours after the initial procedure. Chest tube drainage was minimal and the tube was removed on POD 3. No postoperative complications were noted. The pig recovered from the procedure as expected after a thoracotomy with no adverse events.
In the early postoperative period, great care was taken in gradually reintroducing feeds to protect the anastomosis, and the pig initially lost weight (preoperative weight 68.2 kg to 59.1 kg on POD 10). However, the animal gained weight once oral feeds were begun on POD 13 (Fig. 6). The pig never had excessive salivation.
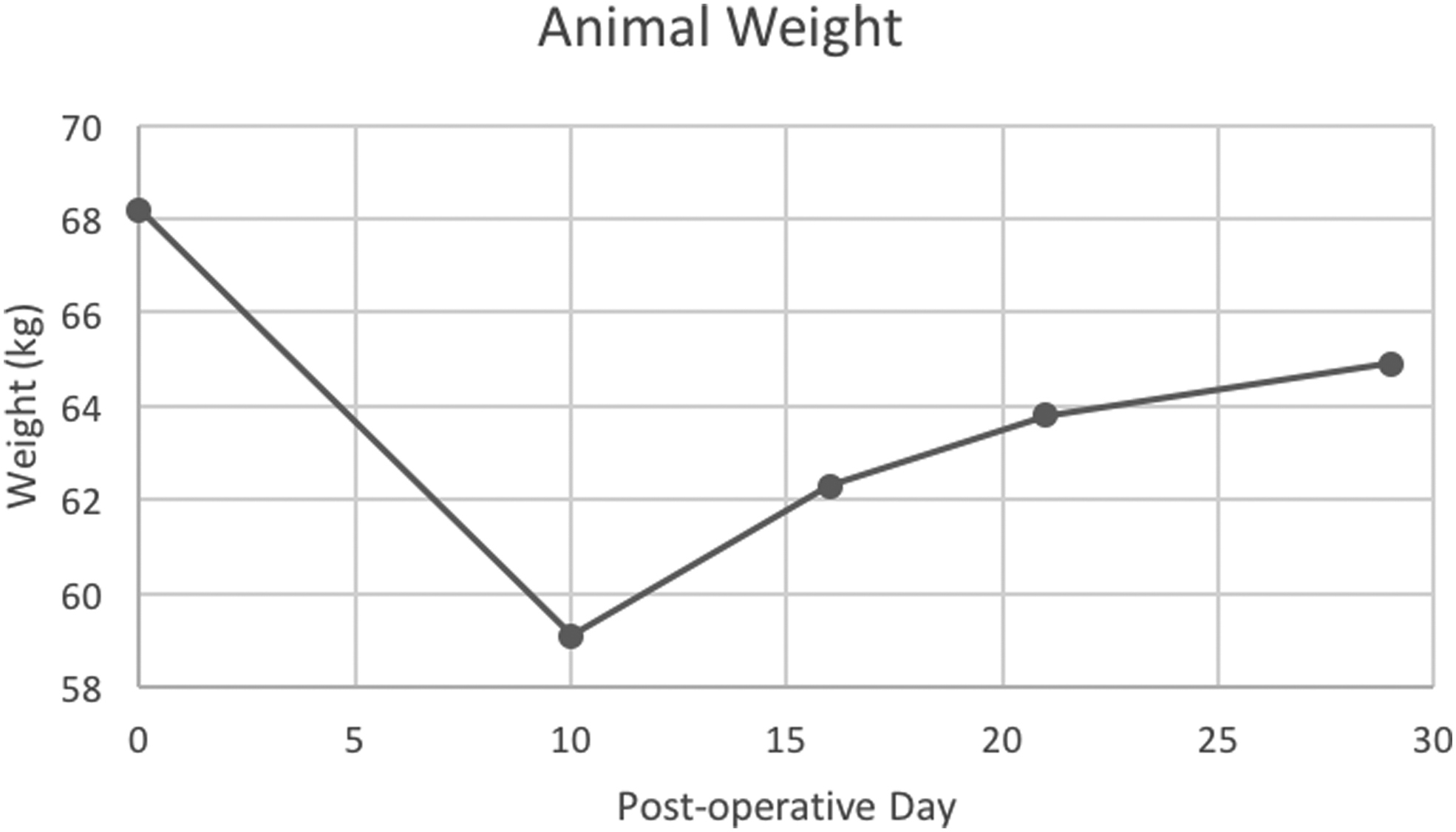
Animal weight gain over time.
Esophageal pouch creation
The distal and proximal pouches measured ∼3.0 cm long and 1.0 cm wide. The internal lumen was at least 18-Fr as defined by the OGT.
The intraoperative leak test showed no evidence of anastomotic leak from the staple lines.
Magnet placement
Endoscopy performed on POD 10 demonstrated a widely patent common channel with intact staple line. The distal end of the common channel was slightly narrowed. The channel was wide enough, however, to allow for the pediatric endoscope to pass into the stomach.
Fluoroscopic images showed contrast in both the proximal and distal esophageal pouches. The gap between the pouches was estimated at ∼3 cm.
Upon initial placement of the magnets, there was an obvious gap between the magnets (Fig. 5). Upon repeat fluoroscopy, ∼5 minutes later, the gap had decreased significantly to ∼1 mm, indicating compression of the tissues and demonstrating the attractive forces of the magnets.
The pig tolerated a switch to liquid oral feeds on POD 13. The animal was noted to have gained weight from 59.1 kg on POD 10 to 62.3 kg on POD 16 (Fig. 6).
On POD 16, fluoroscopy demonstrated that both magnets remained in the thorax and were mated but there was still a small gap between the magnets. Endoscopy demonstrated a qualitatively narrower distalmost aspect of the common channel. However, this could be traversed and the scope was able to be passed into the stomach.
A barium upper gastrointestinal (GI) series confirmed there was a narrowing at the aforementioned location. There was barium filling of the proximal pouch. The only filling of the distal pouch was due to reflux from the stomach. Thus, there was no continuity between the esophageal pouches.
On POD 21, successful anastomosis of the pouches was demonstrated through barium fluoroscopy (Fig. 7). There was a significant anastomotic stricture that was unable to be traversed with the endoscope.

Fluoroscopy demonstrates flow of contrast through the newly formed anastomosis (right side of image) and the widely patent common channel (left).
POD 27 upper GI findings were notable for continued anastomotic patency but with the presence of the magnets paired (without evidence of intervening tissue) and located distal to the stricture. In addition, the stricture at the distalmost aspect of the common channel was noted to be qualitatively larger in diameter. By POD 29, the magnets were unable to be located on fluoroscopy or necropsy. Necropsy demonstrated an esophageal stricture at the site of the anastomosis (Fig. 8), which was determined by the location of the adjacent transverse esophageal staple lines. There was no evidence of anastomotic leak. Based on the gross appearance, the anastomosis appeared to contain all the normal layers of esophagus. Furthermore, there were significant adhesions between the lung and the esophagus at the site of the anastomosis.

Necropsy specimen of the esophagus shows the anastomotic stricture.
Discussion
The challenges of a chronic animal model of EA are largely due to the inability of the animal to clear saliva, leading to aspiration and subsequent death. Unless the institution's animal facility is equipped with an ICU and 24-hour care to suction the saliva, an alternative method of clearing secretions must be used.
The goal of the model described here was to improve upon our previous model by creating a patent esophageal channel while still creating the blind pouches of EA. The patent channel allowed the animal to swallow saliva and, ultimately, water and liquid nutrition, thereby greatly reducing the risk of aspiration and easing the burden of tube feeding. The blind esophageal pouches provided a useful model for investigating modalities to repair the EA anomaly.
Furthermore, the hope for the model was that the retention of a common patent esophageal channel would facilitate PO magnet placement, even in the distal pouch, without requiring a G tube. Although neonates with EA will inevitably require a G tube for feeding, a model that does not require gastrostomy feeds may provide a convenient, and less invasive, means of evaluating repair of EA with less labor-intensive procedures.
A larger animal was used when compared with our previous work, wherein the animal was ∼8 kg. This was done to ensure an esophagus that was large enough to accommodate bifurcation while still allowing for creation of the esophageal pouches, which were felt to be comparable in size to those found in a neonate with pure EA. A possible limitation of this approach is that the esophagus may be thicker than that of neonate.
Clinical evidence of the success of the creation of the common channel was available almost immediately. Prior models involved complete ligation of the esophagus and these pigs expectorated all oral secretions, leading to adverse events and even death. At no point in this study did the pig have any of these problems. By POD 4, the pig was tolerating small amounts of water and liquid feed by mouth.
Use of magnets to create a small intestine anastomosis has been previously described by Harrison and colleagues.2,3 That group has demonstrated that the same principles may be utilized in a more minimally invasive approach utilizing a colonoscope. 4 Utilizing similar techniques and principles, we created an upper GI tract anastomosis.
A significant challenge encountered was initial placement of the distal pouch magnet. Initial attempts to place the distal magnet, on POD 10, were made endoscopically. Although a magnet could be positioned into the proximal pouch, advancing a magnet retrograde into the distal pouch proved too difficult with standard endoscopic techniques. Similarly, attempts to place the distal magnet through the PEG tube also proved futile and, ultimately, the PEG was removed to facilitate endoscope placement through the gastrostomy to place the distal magnet with fluoroscopic guidance.
After the endoscopy and fluoroscopy on POD 10, which demonstrated wide patency of the common channel, the decision was made to start liquid feeds by mouth. The PO feeds were started on POD 13, as POD 10 was a Friday and it was deemed safer to not change the feeding regimen when fewer staff members were present.
When the POD 16 barium fluoroscopy study (6 days after magnet placement) demonstrated that there was no flow of contrast from the proximal pouch into the distal pouch, the suspicion was that either the anastomosis had not yet formed or the anastomosis had formed but the presence of the magnets was completely occluding the lumen. For reference, human experiments utilizing magnets for treatment of EA demonstrated that anastomosis formation occurred between 2 and 9 days after magnet placement.5–7 It was felt that the safest course would be to return in 5 more days to reassess the pouches rather than manipulate the magnets and risk interrupting a partially formed anastomosis.
The POD 21 findings of successful anastomosis with associated stricture were encouraging and consistent with expectations (as postrepair stricture rates of 9%–78% have been reported). 8 It was presumed that the stricture took place at the site of the anastomosis between the two pouches. The magnets were exchanged for larger magnets with the intent of eliminating, or at least mitigating, the stricture. The presence of magnets distal to the stricture on POD 27 and complete absence of magnets on POD 29 are highly suggestive that the magnets continued to pass distally and were eliminated by the animal. Based on the final barium fluoroscopy, the stricture was noted to be slightly dilated compared with that on POD 21.
It is difficult to conclude whether the magnets helped dilate the stricture. First, the stricture may have been in the early phase of healing (with significant inflammation and edema) when it was first noted on POD 21 (particularly given the fact that this was only 11 days after magnet placement). Thus, it is quite possible that the stricture would have shown some radiographic resolution in the absence of upsizing the magnets. Second, the magnets may have mechanically dilated the stricture as opposed to causing tissue necrosis and new tissue growth at the site of the stricture.
This study details successful creation of a unique porcine animal model for EA. The significant advance of this study is the creation of a bifurcated esophagus with simultaneous formation of a patent common channel in addition to proximal and distal esophageal pouches simulating EA. The common channel allowed for elimination of oral secretions, instrumentation, and ultimately for oral feeds, obviating the need for the G-tube and associated labor-intensive patient management.
Repair of EA can have significant associated morbidity. As such, it represents an area of pediatric surgery that is positioned for significant improvement in both technique and technology. However, without an animal model, such innovation may not be possible. The magnet-based platform discussed herein is only one example of numerous potential advances in treatment of EA. This technology has been successfully used in humans, but these studies were performed either outside the United States5,6 or under United States Food and Drug Administration Expanded Access (also known as “compassionate use”) approval.7,9 Although this study comprises only a single animal, it is expected that further validation of this model may help to facilitate creation and testing of a variety of different devices and techniques. More significantly, the existence of an animal model provides a safe experimental platform that avoids unnecessary, or premature, human experimentation.
Future directions for the bifurcated EA animal model include immediate oral feeds, eliminating the placement of the G-tube, and developing a similar model in a smaller animal. In addition, this model may be useful to investigate long gap esophageal atresia and tracheoesophageal fistula. If the study is to be performed without placement of a G-tube, a new technique must be developed for placement of the distal pouch magnet.
Footnotes
Acknowledgments
This study was funded by a grant from the Akron Children's Hospital Foundation. Special thanks to Cassandra Cipriano, RVT, of the Case Western Reserve University, School of Medicine, Animate Skills Core Facility for her assistance with the laboratory portions of this study, and Victor C. Glenn, DDS, for his assistance with creation of the figures.
Disclosure Statement
Dr. Ponsky is a member of the CONMED advisory board. The remaining authors have no conflicts of interest.