
Abstract
Abstract
Aim:
Inguinal hernias may be direct or indirect, and supravesical hernias, a subtype of inguinal hernias, are often mistaken as direct hernias as their symptoms are similar. The purpose of this study was to describe the characteristics of supravesical hernias and to introduce a minimally invasive surgical method as a treatment for supravesical hernias.
Materials and Methods:
Thirty-seven patients with supravesical hernias were treated using laparoscopic herniorrhaphy and wall defect suture with a mesh implant from September 2012 to December 2016 at Damsoyu hospital, Seoul, Korea. Patient characteristics and surgical outcomes were retrospectively evaluated.
Results:
All 37 patients were men with external supravesical hernias. The mean age was 55.3 (range 32–79) years; 23 patients had right-sided, 12 had left-sided, and 2 had bilateral hernias. Comorbidities included lipoma (7/37), contralateral indirect hernia (1/37), and contralateral direct hernia (14/37). No recurrences were reported at the end of the study period.
Conclusions:
Laparoscopic transabdominal defect closure with a mesh implant herniorrhaphy seems to be an effective, minimally invasive treatment option for supravesical hernia.
Introduction
S
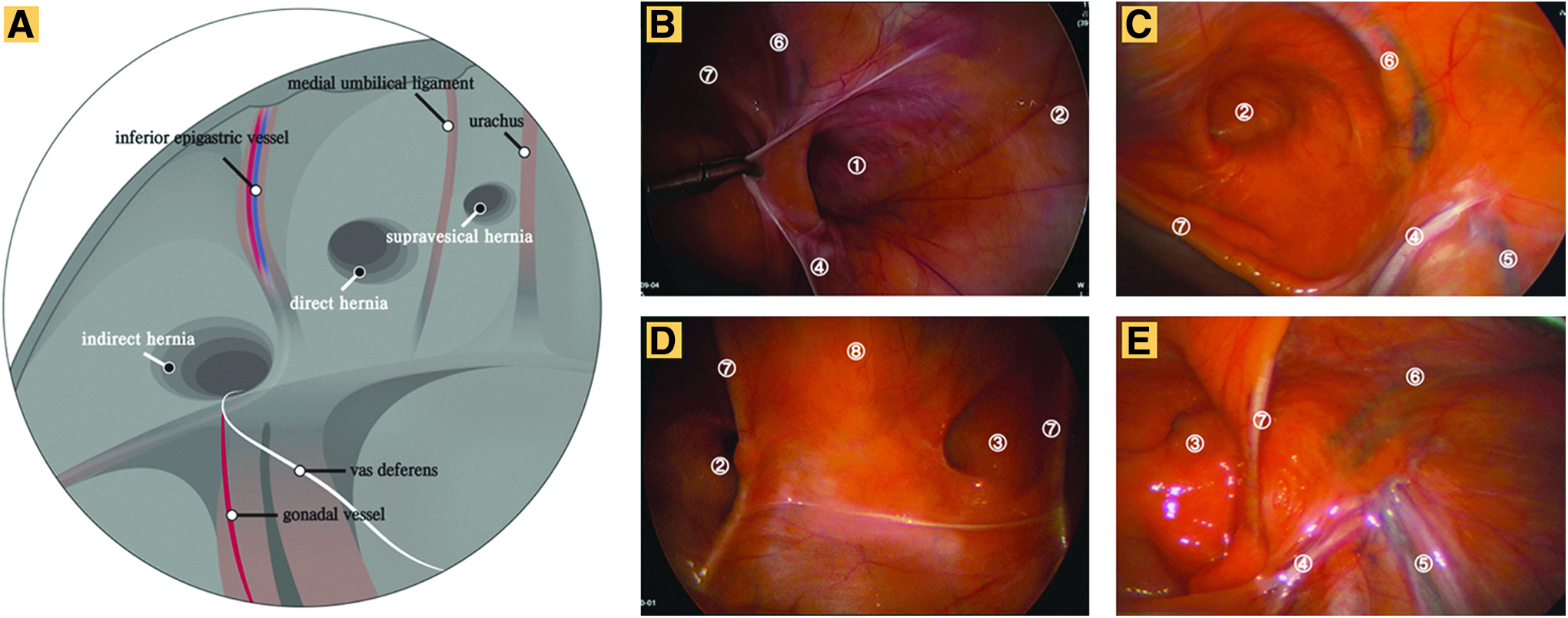
Anatomic features and operative findings of the inguinal region.
Materials and Methods
Clinical and demographic characteristics, intraoperative findings, and surgical outcomes were retrieved from medical records of adult patients who were found to have inguinal hernia and who underwent laparoscopic transabdominal wall defect suture with a mesh implant in a single center from September 2012 to December 2016. Patients with indirect and direct hernias were excluded (Fig. 2).
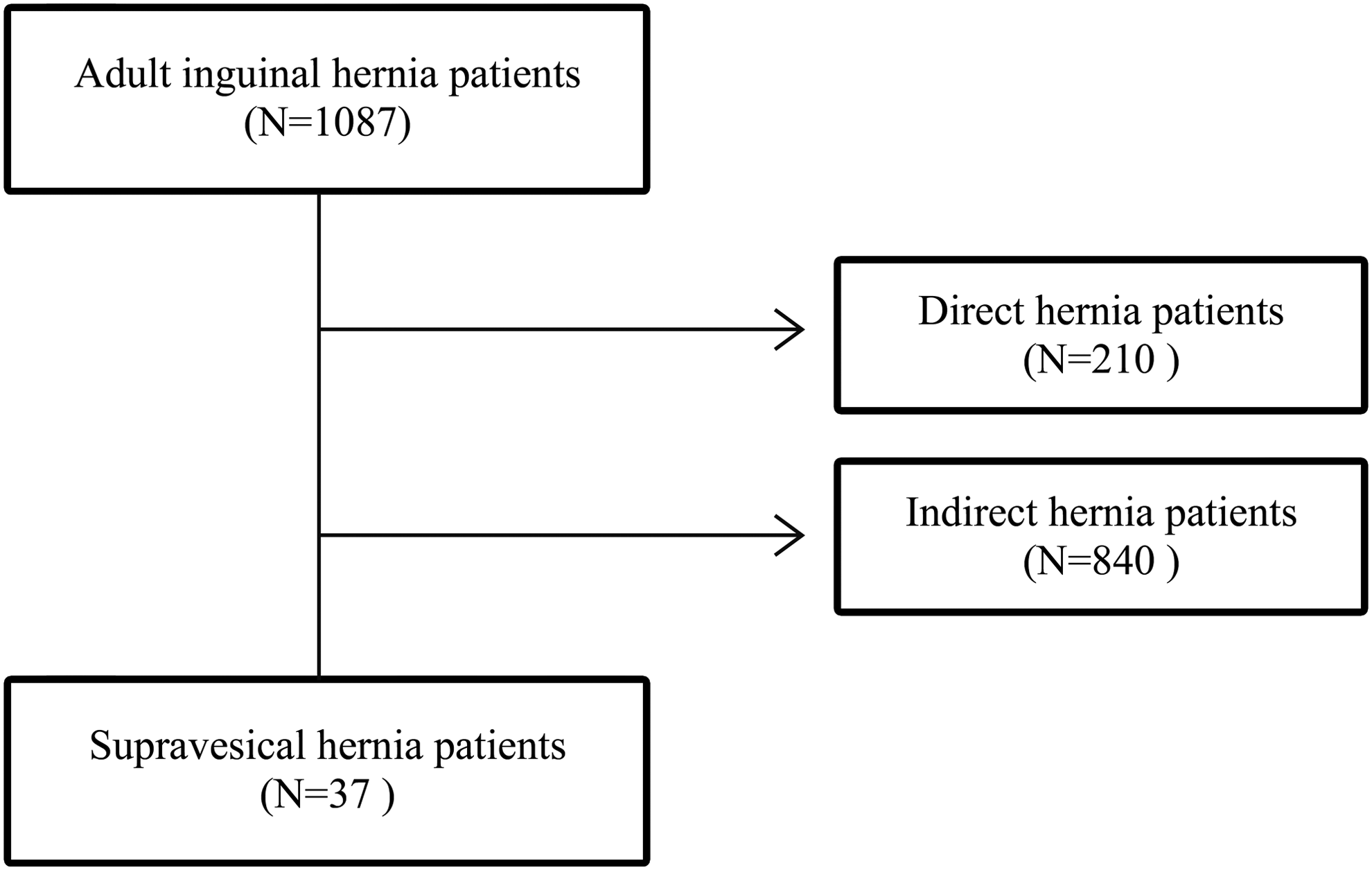
Flowchart of patient enrollment.
Eleven patients underwent reoperation, and all the patients were referred to our clinic after the first operation at another hospital. We reviewed all the medical records of the first operation and confirmed the type of hernia. The direct and indirect regions, which were the primary surgical sites, were confirmed to be obstructed during the operation.
This study was approved by the Public Institutional Review Board designated by the Ministry of Health and Welfare of the Republic of Korea (P01-201612-21-005).
Laparoscopic herniorrhaphy technique
Laparoscopic transabdominal preperitoneal herniorrhaphy was performed using three ports. The procedures were performed under general anesthesia with patients in the supine position; a 5.0-mm camera and 5.0-mm instruments were used. The hernia defect was closed using nonabsorbable multifilament (silk 1-0) sutures as shown in the Supplementary Video S1 (Supplementary Data are available online at www.liebertpub.com/lap). The bottom of the wall defect was tied, sutured in the upward direction to the top of the defect, and then sutured in the downward direction before tying to the initial knot. The defects were repaired using a 7 × 6 cm2 mesh (Fig. 3). The peritoneum was repaired using absorbable multifilament Vicryl 2-0 sutures.

Surgical procedures.
Follow-up protocol
Patients were permitted food after a 1 h observation period and were discharged when they could comfortably perform activities of daily living such as walking and eating. The outpatient follow-up routine included clinic visits at 1 week and 1 month for physical examinations and telephone follow-up for the subsequent years.
Results
Patient clinical characteristics
Patient characteristics are shown in Table 1. All patients had external supravesical hernias; all were men; and the mean age was 55.3 (range 32–79) years, which was regarded as high. Eleven patients had previously undergone inguinal hernia repairs (Supplementary Video S2): 4 underwent tissue repairs, 3 underwent Lichtenstein repairs, 2 received mesh plugs, 1 underwent repair by the PROLENE® Polypropylene Hernia System (PHS) method, and 1 underwent repair by the totally extraperitoneal patch plasty (TEP) method (Fig. 4). Two of the 11 patients who underwent a second operation had recurrent supravesical hernias. Nine of the patients had ipsilateral supravesical hernias after initial indirect (5 cases) or direct (4 cases) inguinal hernia repair. Two patients had bilateral supravesical hernias, 12 had left-sided supravesical hernias, and 23 had right-sided supravesical hernias. Seventeen patients (45.9%) had bilateral hernia symptoms; of these 17, 2 patients had both supravesical hernias, 1 had a contralateral indirect hernia, and 14 had contralateral direct hernias.
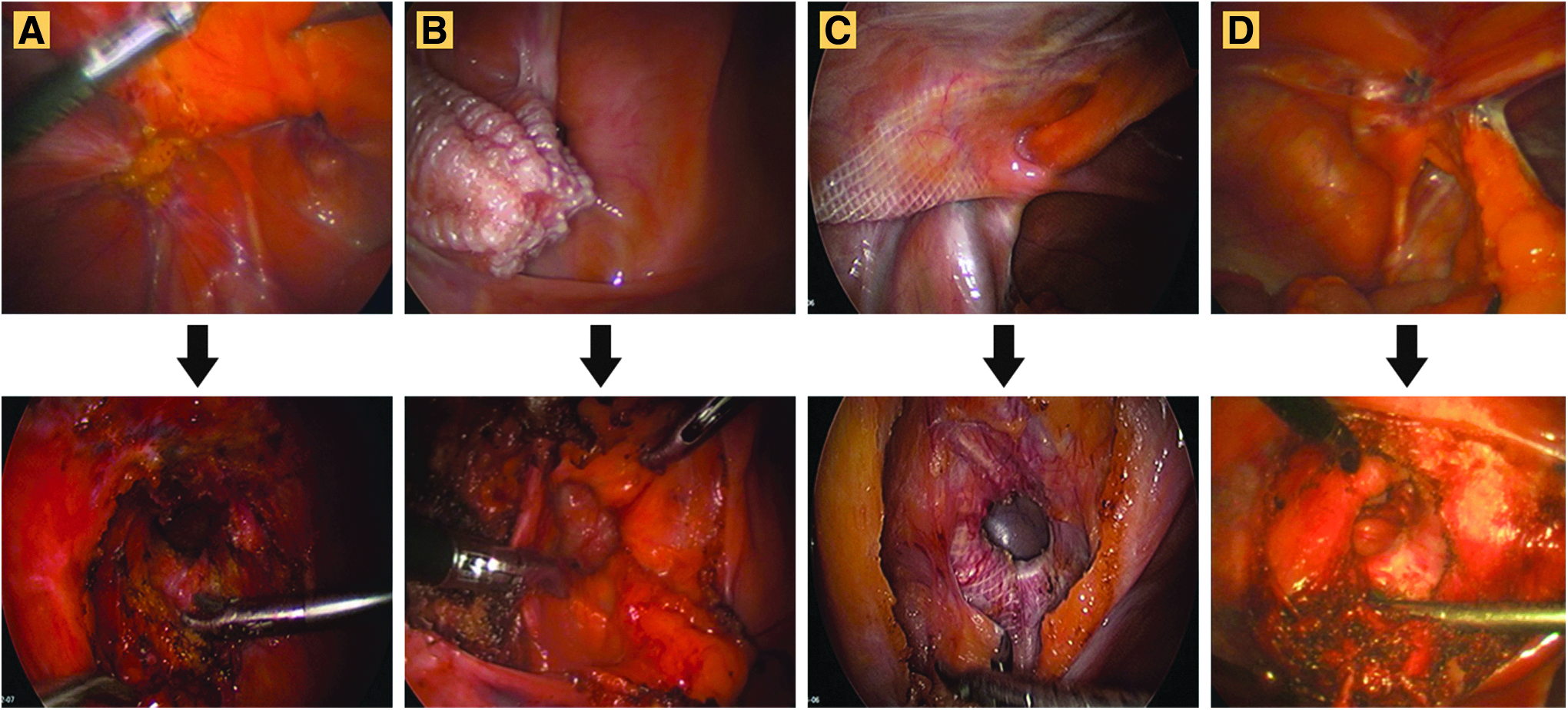
A second operation for supravesical hernias.
All patients in this study had visited our hospital because of inguinal bulging, which had characteristics similar to those of direct hernias. Three patients complained of inguinal pain, 2 complained of pain before urination, and 1 had an incarcerated omental hernia with prolonged symptoms.
Postoperative outcomes
The mean procedure time was 31.3 (range 20–60) min; postoperative outcomes are shown in Table 2. Postoperative hospital stay was 15.6 (range 4–96) h. A lipoma was excised from the lax transversalis fascia in 7 patients (Fig. 5). One patient developed an inguinal hematoma as a postoperative complication, but it resolved during follow-up. No recurrences were observed.
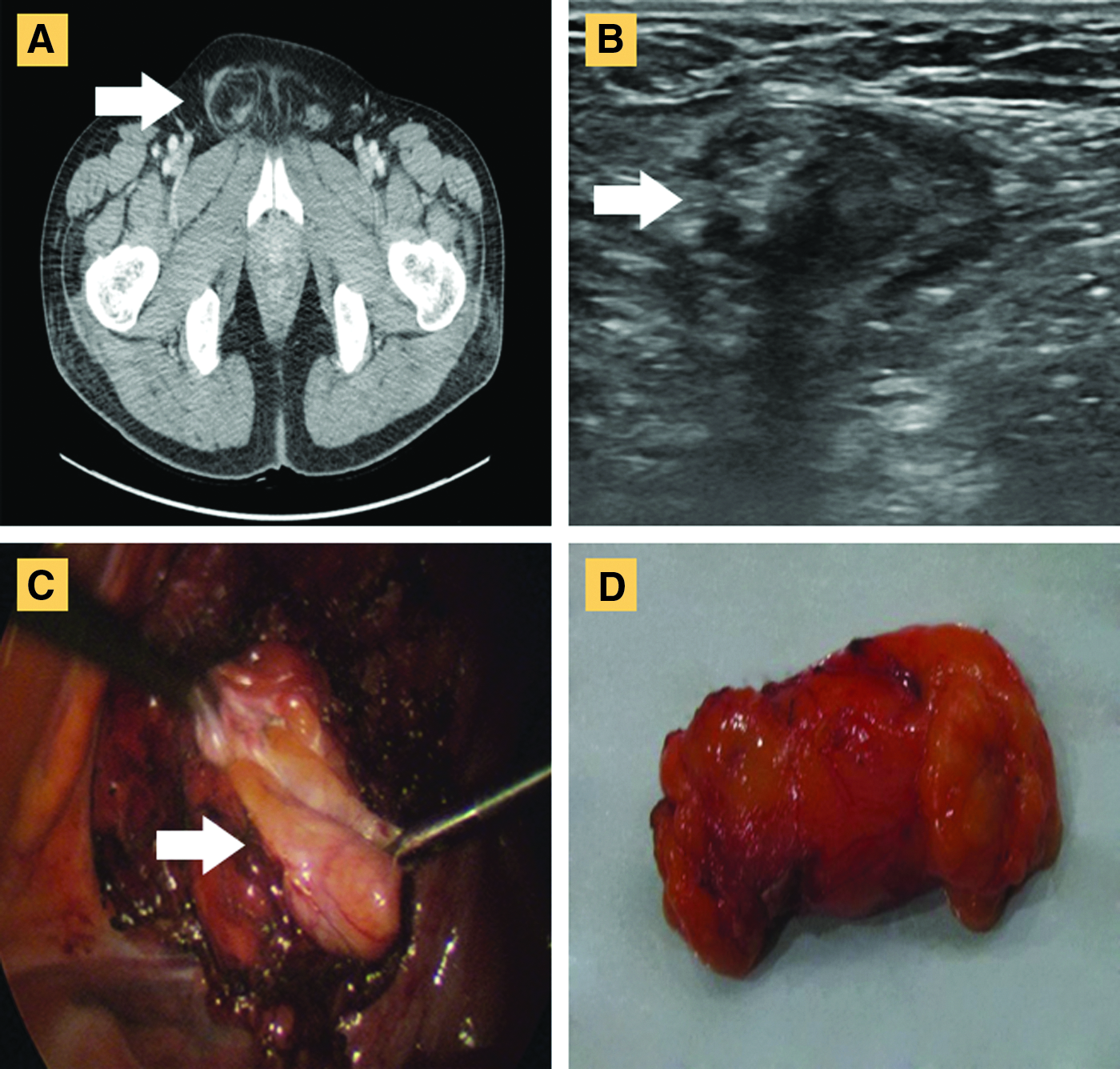
Supravesical hernia containing a lipoma.
VAS, visual analogue scale.
Discussion
The term supravesical fossa was first introduced by Waldeyer in 1874, 9 and it is a triangular area laterally bounded by the medial umbilical ligament and medially bounded by the urachus, and its base is formed by Cooper's ligament. The hernia sac may remain above the pelvis and form an external supravesical hernia or it may descend to become an internal supravesical hernia. Supravesical hernias develop because of failure of integrity of the transversus abdominis aponeurosis and transversalis fascia. 10
Supravesical hernias predominantly occur in adult men and may result from anterosuperior enlargement of the urinary bladder during filling. In women, distension of the urinary bladder occurs laterally. 9
Some patients with supravesical hernias have urinary symptoms such as frequent urination. 11 In our study, of all 37 male patients, 2 complained of pain during urination when their bladder was full. Preoperative diagnosis of supravesical hernias is difficult because their clinical symptoms are similar to those of direct hernia; however, supravesical hernias were suspected preoperatively in 2 patients because of their urinary symptoms. Because preoperative sonograms or CT results were ambiguous, most accurate diagnoses were made during the surgical procedure. The laparoscopic camera allows the surgeon to observe the anatomical structure of hernias and to make an accurate diagnosis of indirect, direct, supravesical, or pantaloon hernias. The supravesical fossa is bordered by the urachus and umbilical ligament, and in this study, only patients with supravesical hernias originating from the supravesical fossa were included.
Seventeen of the 37 supravesical hernias were accompanied by contralateral hernias. Two patients had two supravesical hernias, 14 had contralateral direct hernias, and 1 had a contralateral indirect hernia. In the 14 patients with a direct hernia on one side and a supravesical hernia on the other, there was no difference in symptoms on either sides. Seven patients (18.9%) had accompanying lipomas that had to be checked and removed because lipomas increase the risk of recurrence after herniorrhaphy. 12
Eleven of the 37 patients had previously undergone open surgery or TEP for hernia repair. Two were supravesical hernias, five were indirect hernias, and four were direct hernias. In some of the previous procedures, the Hesselbach's triangle had been covered with a mesh implant, and the supravesical hernia developed medial to the Hesselbach's triangle, suggesting that the previous coverage had been insufficient.
There are no guidelines for the treatment of supravesical hernias. In this study, repair was performed by a laparoscopic transabdominal preperitoneal method with wall defect suture. For inguinal hernias, most reports recommend that the mesh implant should overlap the hernia defect by at least 3 cm in all directions, and there is a strong evidence of reduced recurrence rates with an increased mesh size of up to 10 × 15 cm. 13 After suturing the hernia defect, the suture line is approximately ±1.5 cm, a 7 × 6 cm round-shaped mesh was used in this study (Fig. 2 and Supplementary Video S1). This allowed repair of the wall defect with an overlap of >3 cm in all directions without dissecting the indirect and direct areas. The “triangle of pain” and “triangle of doom” are important structures in the indirect area. Therefore, reducing the size of the dissecting area reduces the risk of injury. The follow-up period was not long enough for optimal monitoring and reporting of recurrence; therefore, we plan to continue monitoring the patients. The patients could be discharged after an average of 15 h postoperatively, and no recurrences were reported at the end of the study period.
The study was limited by its retrospective single-center design and lack of a comparative group. As noted, a longer follow-up is needed to obtain better recurrence data. Surgery that repairs only supravesical defects may lead to subsequent indirect or direct hernias, but until now there have not been any studies on the development of other types of hernias. Therefore, we chose a minimally invasive surgical procedure similar to mesh implantation after fascia suture for repair of small ventral hernias. 14 I have previously reported a novel technique for direct inguinal hernia operation using a 7-cm mesh after a wall defect suture. 15 Although not a common hernia, there are currently no guidelines for supravesical hernia treatment. Therefore, we report this operative method as an option for minimally invasive treatment. To obtain long-term recurrence results, we plan to continue monitoring these patients.
In conclusion, most patients with supravesical hernias were elderly men, and many had bilateral symptoms similar to those of direct inguinal hernia. However, some patients had urinary symptoms. Laparoscopic transabdominal defect closure with a mesh implant herniorrhaphy is an effective, minimally invasive treatment.
Footnotes
Acknowledgments
We thank the members of staff of the Damsoyu hospital who participated in this study.
Disclosure Statement
The author has no conflicts of interest, sources of funding, or financial ties to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.