
Abstract
Abstract
Background:
Laparoscopic hepatic resection (LHR) has been developed as a novel minimally invasive surgery. However, despite improvements in equipment and procedures, intraoperative hemorrhage remains an issue that requires great precaution. To reduce the amount of intraoperative blood loss, we perform the Pringle maneuver, aimed at occluding the inflow of blood into the liver during LHR. This article describes our experience performing LHR using the Pringle maneuver, including postoperative results, and discusses the safety and effectiveness of the Pringle maneuver.
Methods:
Data from 83 patients who underwent laparoscopic partial right hepatic resection with or without the Pringle maneuver were retrospectively analyzed with respect to surgical outcomes, safety, and utility.
Results:
In LHR, the amount of bleeding was significantly lower in cases that included the Pringle maneuver (P = .0314). However, there were no differences in the duration of surgery, surgical margin, rate of curative resections, and incidence of postoperative complications. Laboratory data collected after surgery showed no significant difference between the two groups regardless of whether blood flow was occluded or not.
Conclusions:
The Pringle maneuver may be effective in reducing the amount of intraoperative blood loss during laparoscopic partial right hepatic resection, although the difference is not clinically significant. Rather, the reduction in bleeding can reduce the stress experienced by the operator while keeping the transection stump of the liver dry. Particularly, the extracorporeal Pringle maneuver using cotton tape is simple and convenient and can be carried out within a short amount of time.
Introduction
F
We previously reported that, compared with open partial hepatic resection, laparoscopic partial hepatic resection yielded significantly better outcomes in terms of reduced intraoperative blood loss, reduced incidence of infection at the superficial incisional surgical site, and alleviation of the postoperative inflammatory response.1,6 These results were due to an improvement in the surgical procedure for laparoscopic hepatic resection (LHR) associated with progress in instrumentation for laparoscopic surgery. However, despite improvements in equipment and procedures, intraoperative hemorrhage remains an issue that requires significant precautions in LHR.
In our facility, we perform the Pringle maneuver, aimed at occluding the inflow of blood into the liver, as a measure against intraoperative hemorrhage during LHR. The Pringle maneuver was first reported by Pringle in 1908 as a method of occluding the inflow of blood into the liver during laparotomy; currently, it is used worldwide. 7 Some reports have described in detail the merits and demerits of using the Pringle maneuver in LHR.8–10
In this study of a series of patients treated with laparoscopic partial hepatic resection in our department for resection of tumors in the right hepatic lobe, we report the surgical outcomes and improvements added to the extracorporeal Pringle maneuver by using cotton tape; we also examine the safety and utility of the procedure.
Materials and Methods
Patient population and selection
Between March 12, 2012 and December 31, 2016, we conducted laparoscopic partial hepatic resection for liver tumors on 83 consecutive patients with a single resection area in the right lobe (segment V, VI, VII, VIII) at Osaka Medical College Hospital in Takatsuki City, Japan. All patients were fully informed of the study design according to the Ethics Committee on Clinical Investigation of Osaka Medical College Hospital (No. 1828 and 1997) and provided written informed consent. Tumor size less than 5 cm is the main criterion for LHR. Patients with portal or hepatic vein involvement and invasion to adjacent organs were not considered candidates for LHR.
The Pringle maneuver was not performed in a total of 25 cases, including 16 patients who had been treated before March 2013, and 9 patients for whom taping was judged impossible due to adhesions in the hepatic portal area. The Pringle maneuver was carried out in 58 patients treated in April 2013 and thereafter, in whom taping of the hepatoduodenal mesentery was feasible.
Criteria to convert laparoscopic to open hepatic resection were: (1) liver stumps of both preserved and resected sides unable to be adequately expanded, (2) uncontrolled intraoperative bleeding, (3) blood loss exceeding 500 mL, (4) total time of Pringle maneuver (hepatic blood flow occlusion) exceeding 120 minutes, and (5) intraoperative bile leakage identified intraoperatively that cannot be improved.
Surgical procedure
In this series, all patients underwent potentially curative hepatic resection with removal of gross tumor with negative macroscopic margins. All procedures were performed by three experienced hepatobiliary surgeons (Y.I., F.H., K.U.) during the study period.
All procedures were performed with the patient under general anesthesia. The detailed laparoscopic surgical technique routinely used in our department has been described in previous reports.1,11,12 In brief, the patients are placed in a moderate left lateral decubitus position. After the introduction of a 12-mm umbilical port using an open technique, continuous carbon dioxide pneumoperitoneum is induced at a pressure limit of 12 mmHg and flow of 6 L/minute to decrease the risk of gas embolism. Four 5- to 12-mm trocars and a 45° laparoscope (1588 AIM; Stryker Japan K.K., Tokyo, Japan) are fixed. The liver is evaluated in all cases using intraoperative laparoscopic ultrasonography (Prosound α7; Hitachi Aloka Medical, Ltd., Tokyo, Japan).
Then, mobilization of the liver is initiated; the right lateral hepatic attachment and the triangular ligament were divided using the Surgical Tissue Management System (Thunderbeat; Olympus, Inc., Tokyo, Japan) after the round and falciform ligaments were dissected. This dissection was typically carried up to the diaphragm, allowing more effective mobilization of the liver.
Next, the avascular lesser omentum was divided. From the port that was inserted at the midaxillary line, the device was inserted from Winslow's foramen to pass behind the hepatoduodenal ligament; the forceps was inserted until it reached the orifice that was opened in the lesser omentum. A cotton tape was inserted through the left upper abdominal port; its edge was held with a forceps and was pulled out to carry out taping of the hepatoduodenal ligament; and finally, the cotton was pulled out of the abdominal cavity through the left upper abdominal port. A cotton tape was then passed through a vascular occlusion tube (Vessel-Clude; Argon Medical Devices, Inc.) for use as a tourniquet to enable performance of a Pringle maneuver (Fig. 1). To perform an extracorporeal Pringle maneuver, blood flow was occluded by clamping the Vessel-Clude from outside the body. Intermittent clamping was applied, with 15-minute clamping and 5-minute release periods.
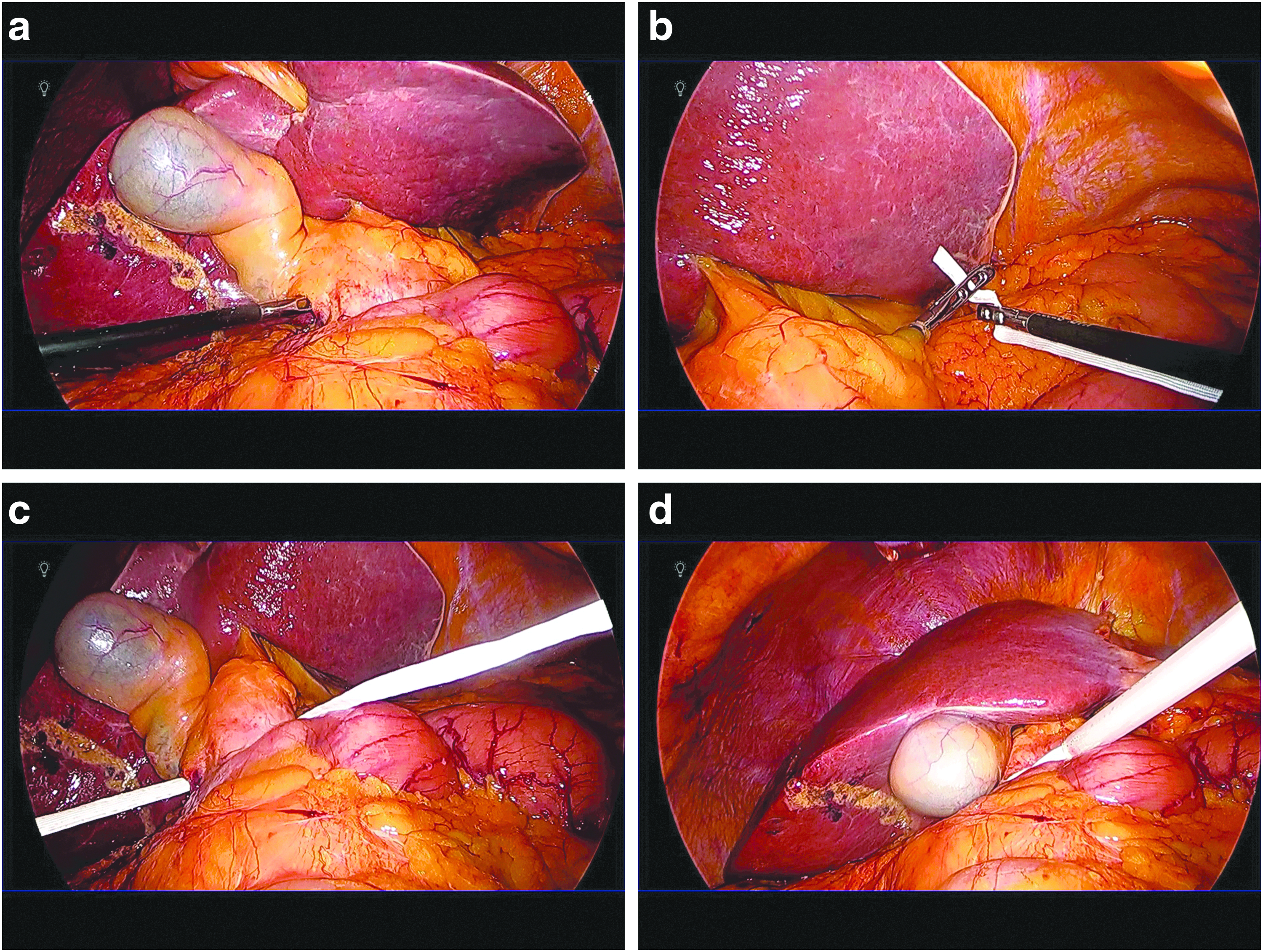
Placement of extracorporeal Pringle maneuver during laparoscopic hepatic resection.
By changing the port inserted, the laparoscope operator formed a triangle with the laparoscope in the center, placing the operator, target area, and the laparoscopic monitor on a straight line, maintaining the coaxial position. Central venous pressure was maintained at 3–5 mmHg during parenchymal transection. Parenchymal transection was achieved using an ultrasonic dissector; the SonoSurg ultrasonic surgical system (Olympus, Inc.) and Thunderbeat under extracorporeal Pringle maneuver. Small vessels were ligated or coagulated using a soft-coagulation system. Intraparenchymal control of the major vessels was achieved with clips, whereas biliary and vascular radicle division was obtained with clips or stapling devices. Then, the laparoscopic Pringle maneuver was performed. The resected, undivided specimen was placed in a plastic retrieval bag and removed through the slightly enlarged periumbilical incision.
Preoperative factors
Data examined included preoperative factors, surgical factors, and pathological factors. Preoperative factors investigated were age, sex, viral infection status, aspartate aminotransferase (AST) level, alanine aminotransferase (ALT) level, platelet count, albumin, total bilirubin, prothrombin time (PT), Child-Pugh classification, and indocyanine green retention rate at 15 minutes (ICGR-15).
Surgical and pathological factors
Surgical factors included conversion rate, surgical duration, intraoperative blood loss, and blood transfusion requirements. Pathological factors evaluated included the size of the largest tumor, number of tumors, and surgical margin status. “R” classification denoted the absence or presence of residual tumor after surgery. 13 R0 resection refers to excision of the tumor in one piece without violating the tumor plane or achieving negative margins after sequential reexcision of the involved margins. R1 resection involves a microscopically positive margin anywhere, and R2 resection involves a macroscopically positive margin(s) with visible tumor.
Postoperative evaluation
The following parameters were evaluated: AST, ALT, albumin, total bilirubin, PT, conversion rate, surgical duration, intraoperative blood loss, transfusion rate, pathological margins, postoperative complications, 30-day mortality, and hospital stay.
Morbidity was graded according to Clavien's classification.14,15 Surgical site infections were defined according to the Center for Disease Control's National Nosocomial Infection Surveillance system. 16
On the basis of the criteria of the International Study Group of Liver Surgery (ISGLS), 17 posthepatectomy liver failure was defined as an impaired ability of the liver to maintain its synthetic, excretory, and detoxifying functions, which we assessed by detecting an increase in the international normalized ratio and concomitant hyperbilirubinemia (according to the normal limits of the local laboratory) on or after postoperative day 5. 18
Statistical analyses
To minimize the influence of potential confounders on selection bias, propensity scores were generated using binary logistic regression. Independent variables entered into the propensity model included preoperative information. One-to-one matching between groups was accomplished using the nearest-neighbor matching method. This matching was performed without replacement and using a caliper width of 0.2 standard deviations of the logit of the estimated propensity score. After propensity score matching (PSM), the two matched groups were handled as unpaired independent groups. Continuous variables were expressed as median ± standard deviation. Continuous variables were compared using Student's t-test and the χ2 test. Univariate analyses of categorical variables were compared using the likelihood-ratio test, Fisher's exact test, or Mann-Whitney test, as appropriate. Multivariate analyses were performed by Cox proportional hazards regression. P < .05 was considered significant. All statistical analyses were performed using JMP version 12 (SAS Institute, Inc., Cary, NC).
Results
In the Pringle maneuver group, most of the patients were undergoing repeat hepatic resection, the amount of liver excised was large, and liver function had decreased significantly. Therefore, to avoid selection bias between the two groups, a comparative study was carried out by using one-to-one propensity score matching (Table 1). As a result of propensity score matching, 19 patients were selected each for the Pringle maneuver group and the non-Pringle maneuver group (Table 2).
denotes p < 0.05.
HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; ICGR-15, indocyanine green retention rate at 15 minutes; PM, Pringle maneuver; PSM, propensity score matching.
denotes p < 0.05.
PHLF, posthepatectomy liver failure; PM, Pringle maneuver; PSM, propensity score matching; SSI, surgical site infection.
The most important finding was that when laparoscopic partial hepatic resection was used for the treatment of tumors of the right lobe of the liver, the amount of bleeding was considerably lower among those who underwent the Pringle maneuver. However, no significant difference was found between the two groups in terms of the duration of surgery, surgical margin, rate of curative resections, and incidence of postoperative complications. Furthermore, the results of tests conducted on blood samples collected at day 1, day 2, day 4, and day 7 after surgery showed that, regardless of whether blood flow was occluded or not, no significant difference was found between the two groups in terms of the clinical course of total bilirubin, albumin, PT, AST, and ALT.
In the year 2011, we performed the Pringle maneuver intracorporeally using the Endo intestinal clip (PL541S; Aesculap AG, Tuttlingen, Germany; Fig. 2), but since 2012, we have performed extracorporeal Pringle maneuvers using cotton tapes. In the year 2015, extracorporeal Pringle maneuver using cotton tapes and intracorporeal Pringle maneuver using Endo intestinal clip were performed consecutively on 10 patients, and the blood flow in the main trunk as well as that in the right branch of Glisson's capsule were compared. Results showed that with the method using Endo intestinal clip (3/10, artery: one, portal vein: one, artery and portal vein: one), the arterial blood flow was not adequately occluded, but with the extracorporeal Pringle maneuver, blood flow in both the artery and the portal vein was completely occluded in all patients (Table 3).

Pringle maneuver using Endo intestinal clip with application directly to the hepatoduodenal ligament.
Discussion
As the amount of intraoperative blood loss has previously been reported to correlate with postoperative surgical site infections, intraoperative blood loss is an important factor that considerably affects the surgical outcome of hepatic resection, mainly in terms of the occurrence of postoperative complications. 19 A number of reports on laparotomy have shown that in hepatic parenchymal dissection, which carries a major risk of intraoperative hemorrhage, occluding the hepatic inflow of blood is a means for reducing the amount of intraoperative blood loss. 20 However, previous reports have shown that in LHR, hemostasis could be fully achieved by simply increasing pneumoperitoneal pressure; as a result, the utility of blood inflow occlusion, otherwise known as the Pringle maneuver, still remains controversial. Therefore, in this study, we report a surgical technique consisting of laparoscopic partial hepatic resection using an extracorporeal Pringle maneuver, as well as its outcomes.
Bleeding during hepatic resection consists of bleeding from arteries, veins, and from the portal vein. Because the movements of the forceps are limited and enlargement of the surgical field of view is virtually impossible in LHR, dealing with such bleeding can be difficult. For this reason, venous bleeding during LHR can be treated by increasing pneumoperitoneal pressure, reducing central venous pressure, reducing ventilatory volume, or reducing positive end expiratory pressure. 21 However, what should be the treatment for bleeding from arteries or from the portal vein? As the results of our study show, only occluding the inflow of blood was effective in reducing the amount of intraoperative blood loss. This would help reduce the stress experienced by the operator while keeping the surgical field of vision dry; however, there were no significant differences in clinical outcomes. Before we begin hepatic parenchymal dissection, we initially carry out an extracorporeal Pringle maneuver using cotton tape, except when taping is impossible due to adhesions. This technique is easy and does not require any special instruments; in addition, cotton tape cost and the Vessel-Clude cost is inexpensive. By doing so, one can manage sudden bleeding by first carrying out an extracorporeal Pringle maneuver to reduce the intensity of the bleeding, fully evaluating the bleeding source, and conducting hemostasis.
The following instruments are used in the Pringle maneuver. In the intracorporeal Pringle maneuver using the Endo intestinal clip, which was performed up to the port in the right flank region, had to measure 12 mm, but there was no need to add a port. However, with this method, complete closure of the vascular pedicle is difficult to achieve. This might be due to the abundance of visceral fat, and also due to the fact that if the hepatoduodenal ligament is thick, pinching with the tip of an intestinal forceps is not strong enough, allowing some blood to flow through. Since an extracorporeal Pringle maneuver using cotton tape occupies one port, one additional port is required with this method. However, with an extracorporeal Pringle maneuver, complete closure of the vascular pedicle is easy to achieve, and the procedure does not take long even if avascularization has to be carried out repeatedly.
What are the postoperative changes in liver function and portal venous blood flow? We performed an extracorporeal Pringle maneuver consisting of a 15-minute occlusion time and a 5-minute reperfusion time, but results of blood tests, particularly in terms of postoperative liver enzyme levels, showed no difference compared with patients who had not been subjected to the Pringle maneuver. In addition, in the group which was subjected to an extracorporeal Pringle maneuver using cotton tape and Endo intestinal clip, postoperative portal vein thrombosis due to intimal damage caused by crushing injury of the hepatoduodenal ligament did not develop in any patient, and results showed no significant difference in the incidence of postoperative complications. 22
In conclusion, the Pringle maneuver may be effective in reducing the amount of intraoperative blood loss during laparoscopic partial right hepatic resection, although the difference is not clinically significant. Rather, the reduction in bleeding can reduce the stress experienced by the operator while keeping the transection stump of the liver dry. In particular, the extracorporeal Pringle maneuver using cotton tape is simple and convenient, and can be carried out within a short amount of time. However, our study is limited because it was conducted on a small number of cases and the surgical procedure was limited to partial resections; thus, the study may have been vulnerable to various biases. Well-designed studies, such as randomized controlled trials and meta-analyses, will need to be performed in the future.
Footnotes
Acknowledgment
This work was supported by the Mitsui Life Social Welfare Foundation.
Disclosure Statement
No competing financial interests exist.