
Abstract
Abstract
Background:
Uniportal video-assisted thoracoscopic surgery (VATS) is increasingly being performed worldwide. During the operation, specimen extraction from a small incision less than or equal to 2 cm can be challenging without the use of a commercial specimen retrieval device. There have been no reports regarding the use of the glove-finger technique in uniportal VATS. The aim of this study was to assess the feasibility of the alternative specimen retrieval method by glove-finger technique.
Methods:
We retrospectively investigated 50 patients with peripheral lung lesions who underwent uniportal VATS wedge resection with a 2-cm incision at Kaohsiung Medical University Hospital between August 2015 and December 2016. The cut end of the glove-finger was used to extract the specimen.
Results:
Fifty-five wedge-resected specimens were extracted successfully by glove-finger technique. There was no conversion to two-port nor three-port VATS. After intraoperative frozen section analysis for all specimens, 24 were revealed to have primary lung cancer and subsequently underwent completion lobectomy or segmentectomy; the other 31 showed 10 pulmonary metastases, 9 pulmonary benign lesions, and 12 pulmonary infectious lesions. All specimens were resected with free margins and the mean diameter of the lesions was 1.64 ± 0.59 cm (range: 0.2–2.6 cm) by pathological examination. No intraoperative complication related to the technique was observed.
Conclusions:
This is the first study to reveal the efficacy and benefits of the glove-finger extraction technique in uniportal VATS. In our preliminary experience, this method can decrease costs without compromising the quality and safety of patient care.
Introduction
U
Materials and Methods
This study was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (approval number: KMUHIRB-E(I)-20170006) and the need for informed consent was waived.
Fifty consecutive patients with peripheral lung lesions who underwent uniportal VATS wedge resection with 2-cm incisions between August 2015 and December 2016 were reviewed. Of the 50 patients, 55 specimens were collected and analyzed in terms of characteristics and lesion size by pathological examination. Glove-finger extraction technique was applied to all specimens and the detailed procedure is described as follows.
Operative technique
The uniportal VATS was performed by creating an ∼2-cm skin incision through the fifth intercostal space on the anterior axillary line (Fig. 1A). Instruments routinely used included the 3-mm grasping forceps, a ring forceps, and a 3-mm 30-degree thoracoscope (Karl Storz, Munich, Germany). We do not use a wound protector to allow more camera mobility and wider instrument manipulation, similar to the viewpoint of Gonzales-Rivas et al. 2 Use of unfolded gauze to reduce disturbance of the surgical view from oozing blood was adopted when necessary, as mentioned previously. 3 Peripheral lung lesions that were considered small, relatively deeply seated, or with a ground-glass component were subjected to preoperative computed tomography-guided dye localization. Target peripheral lung lesions were all identified by visualizing the visceral pleural abnormality, dye marking, or direct finger palpation, then followed by wedge resection via an articulating Endocutter (ECHELON FLEX™ ENDOPATH®; Ethicon US LLC).
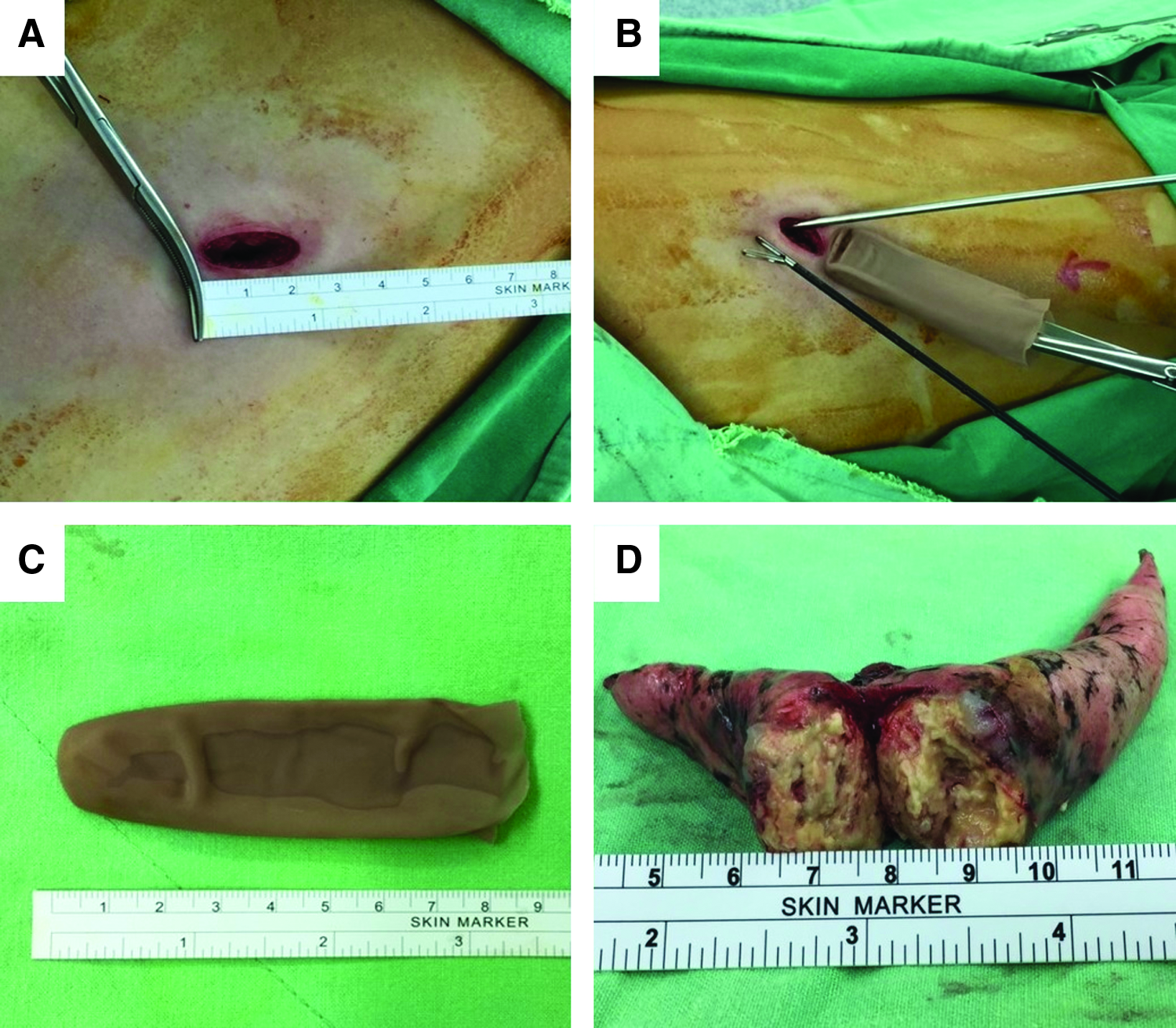
To remove the specimen, we cut the middle finger at its base from the surgical glove (Triflex®; Cardinal Health, Illinois, USA) number 8 (Fig. 1C). The gloves used were without talcum powder coating to avoid causing adverse effects, such as adhesion formation and its potential carcinogenic effect.
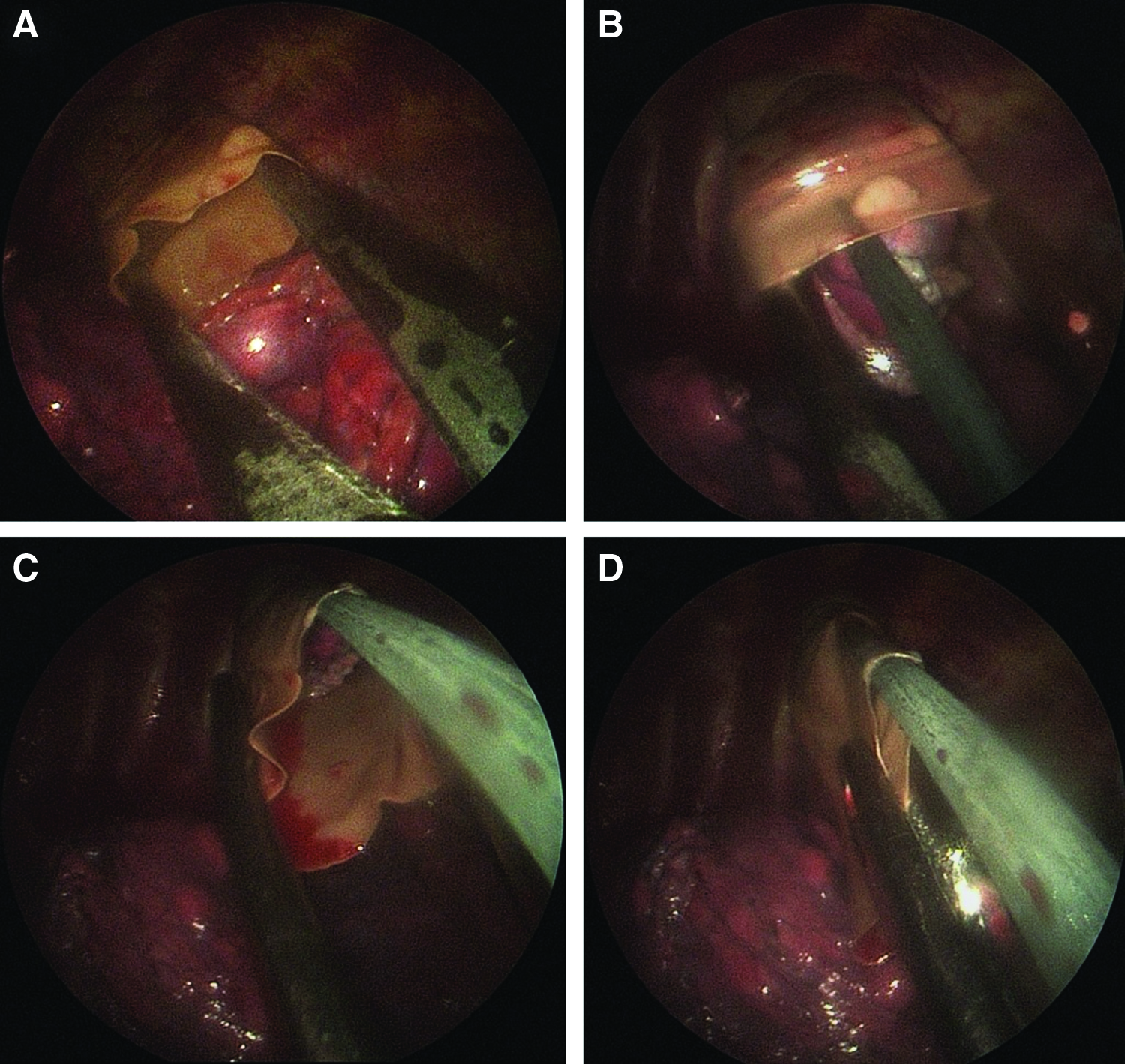
The ring forceps was inserted into the glove-finger first and both were passed into the thoracic cavity through the single incision (Fig. 1B). The ring forceps was kept open to widen the glove finger's orifice (Fig. 2A). Next, the 3-mm grasping forceps was used to grasp the specimen and pack it into the glove-finger (Fig. 2B). Once the whole specimen was inside the glove, the ring forceps was retreated and the mouth of the glove-finger clamped, followed by extraction under thoracoscopic visualization (Fig. 2C, D). The extraction technique typically took 1 to 2 minutes (see Supplementary Video S1, Glove-Finger Extraction Technique in uniportal VATS; Supplementary Data are available online at www.liebertpub.com/lap).
Statistics
Results are expressed as mean ± standard deviation.
Results
In our initial experience, 55 specimens were obtained through uniportal VATS wedge resection in 50 patients. There was no conversion to two-port nor three-port VATS. The study cohort composed of 28 men and 22 women, aged 58.43 ± 11.21 years. After intraoperative frozen section analysis for all 55 specimens, 24 were revealed to have primary lung cancer and subsequently underwent completion lobectomy or segmentectomy, by either single port or two-port VATS. The other 31 showed 10 pulmonary metastases (Fig. 1D showed metastatic colorectal adenocarcinoma), 9 pulmonary benign lesions, and 12 pulmonary infectious lesions, all listed in Table 1. All specimens were resected with free margins and the mean diameter of the lesions was 1.64 ± 0.59 cm. Table 2 shows the range of diameter of pulmonary lesions by pathological examination. No specimen disruption or wound contamination was present during the extraction process, and no wound infection or local recurrence occurred during the postoperative follow-up period (3–19 months).
ACC, adenoid cystic carcinoma; SCC, squamous cell carcinoma.
Data are number of lesions (%).
Discussion
Jain and Sedman 4 were the first to use the glove-finger to extract a dissected appendix in laparoscopic appendectomy (LA). Later, Tebala 5 and Hennessey 6 described the refinement and modification of the Glove-Finger Extraction Technique in LA. Nazir et al. proposed that the glove-finger extraction technique allows clinicians to maintain an optimal standard of patient care while reducing the financial burden of the LA. 7 Mendoza-Sagaon et al. 8 also advocated the use of the glove-finger to remove the appendix in LA for its advantages of ease, safety, and inexpensiveness.
In uniportal VATS with a small incision less than or equal to 2 cm, instrument collision is frequently encountered, which increases operative time and surgeon's stress. Specialized articulating instruments, wound protectors, and commercial specimen retrieval devices were introduced to enhance the operative quality and shorten operative time. 9 It is obvious that financial burden is a great concern.
According to our experience in uniportal VATS wedge resection, with the routine use of the 3-mm 30-degree thoracoscope throughout the operation and good communication with the cameraman, we can still obtain space for multiple instruments manipulated together to minimize interference. Furthermore, we reduce the operative cost by using the glove-finger extraction technique. In our hospital, comparing the costs of specimen retrieval devices, one pair of surgical gloves (Triflex; Cardinal Health) merely costs US$0.3, which is significantly cheaper than the commonly used commercial devices, such as Covidien Endo Catch (Medtronic) and LapSac® surgical tissue pouch (COOK MEDICAL, Bloomington, USA) (2 × 5 inch version), which cost US$60 and US$31.7, respectively. Also, since a wound protector (Alexis®; Applied Medical, California, USA; US$121.3) is not used with this technique, the charges would be lowered even further.
It is worth mentioning that a pair of gloves has 2 middle fingers. If the index finger and ring finger are included, we have a total of 6 glove-fingers to extract specimens with, which is useful when multiple wedge resections have to be performed during the operation.
However, a limitation of this technique should be emphasized; specifically, that the glove-finger is not suitable for large tumors or bulky specimens that are beyond the capacity and elasticity of the glove-finger. When confronted with this situation, the glove-finger technique should be replaced by other methods. Sometimes, we pack the specimen into the “palm portion” of the glove and remove it entirely. Moreover, this often means that the skin incision has to be enlarged to avoid tumor spillage and wound contamination. Although our results are positive, this may be limited by the small sample size and the selection bias as to when to use the glove-finger technique. Based on our results, the technique causes no damage to the specimen and disruption of cancer cells if applied to patients having small peripheral lung lesions with a diameter <2 cm. With refinement of the technique and accumulation of experience, we are even able to deal with lesions between 2 to 3 cm successfully. Further studies with larger sample sizes are necessary to confirm our findings.
To the best of our knowledge, this is the first time that the glove-finger technique has been described for uniportal VATS. The technique possesses merits of availability of common thoracoscopic instruments, reduced costs, and ease of execution.
In conclusion, our glove-finger technique is feasible and cost-effective, enabling successful specimen extraction in uniportal VATS.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.