
Abstract
Abstract
Introduction:
Currently, neoplasms of the trachea and lower airway demand open transcervical approach with or without thoracotomy. We describe here a novel, minimally invasive approach for an intraluminal lesion of the thoracic trachea, called percutaneous trans-tracheal endoscopic approach (PTEA). Apart from obvious advantages over potentially morbid open procedures, this technique has certain peculiar benefits over rigid or flexible bronchoscopic approach.
Materials and Methods:
A 43-year-old male patient had glomus tumor of thoracic trachea. After detailed workup and informed written consent, he was taken up for percutaneous trans-tracheal excision under general anesthesia. The foremost step of the procedure is awake fiberoptic guided intubation, using the microlaryngeal tracheal tube, followed by elective tracheotomy. Subsequently, the lower end of the microlaryngeal tube was carefully pushed further inside the trachea so that the cuff of the tube lies distal to the tumor. The cuff is then inflated so that the operating area is sealed off from lower airway to aid continuous inhalational anesthesia and to prevent aspiration of blood. The surgeon sitting at the head end removed the tumor through tracheotomy under endoscopic guidance. After achieving absolute hemostasis, neck wound was closed.
Results:
Patient had complete removal of the tumor without any aspiration intraoperatively or in the postoperative period. The anesthetic agent could be delivered uninterrupted through the secured airway, below the operative area separated by sealed cuff of the microlaryngeal tube.
Conclusions:
For excision of benign luminal lesions of the lower trachea, the novel approach of PTEA has many distinct and fool proof advantages in comparison to the transoral laryngoscopic/bronchoscopic and the transcervical approaches.
Introduction
I
Materials and Methods
A 43-year-old army personnel from Nepal came to our institute for the management of residual glomus tumor of thoracic trachea. He had undergone rigid bronchoscopic removal of a tracheal mass under general anesthesia twice in the past, at another hospital. At presentation, he had intermittent breathing difficulty and the bronchoscopy showed a multilobulated vascular tumor arising from the posterolateral wall of the thoracic trachea. Gallium-68 DOTATOC scan showed somatostatin receptor positive tumor in right lateral wall of the trachea at the level of D4 vertebra (Fig. 1). I131 Monoiodo Benzoguanidine whole body scan showed no uptake. He was taken up for percutaneous trans-tracheal excision under general anesthesia. Informed written consent was taken from the patient and his relatives by explaining the detailed steps of the procedure along with all probable complications, their implications, and the management plan. Risk of pneumothorax, pneumomediastinum, and aspiration pneumonia were explained along with the probable need for mechanical ventilation in the postoperative period.
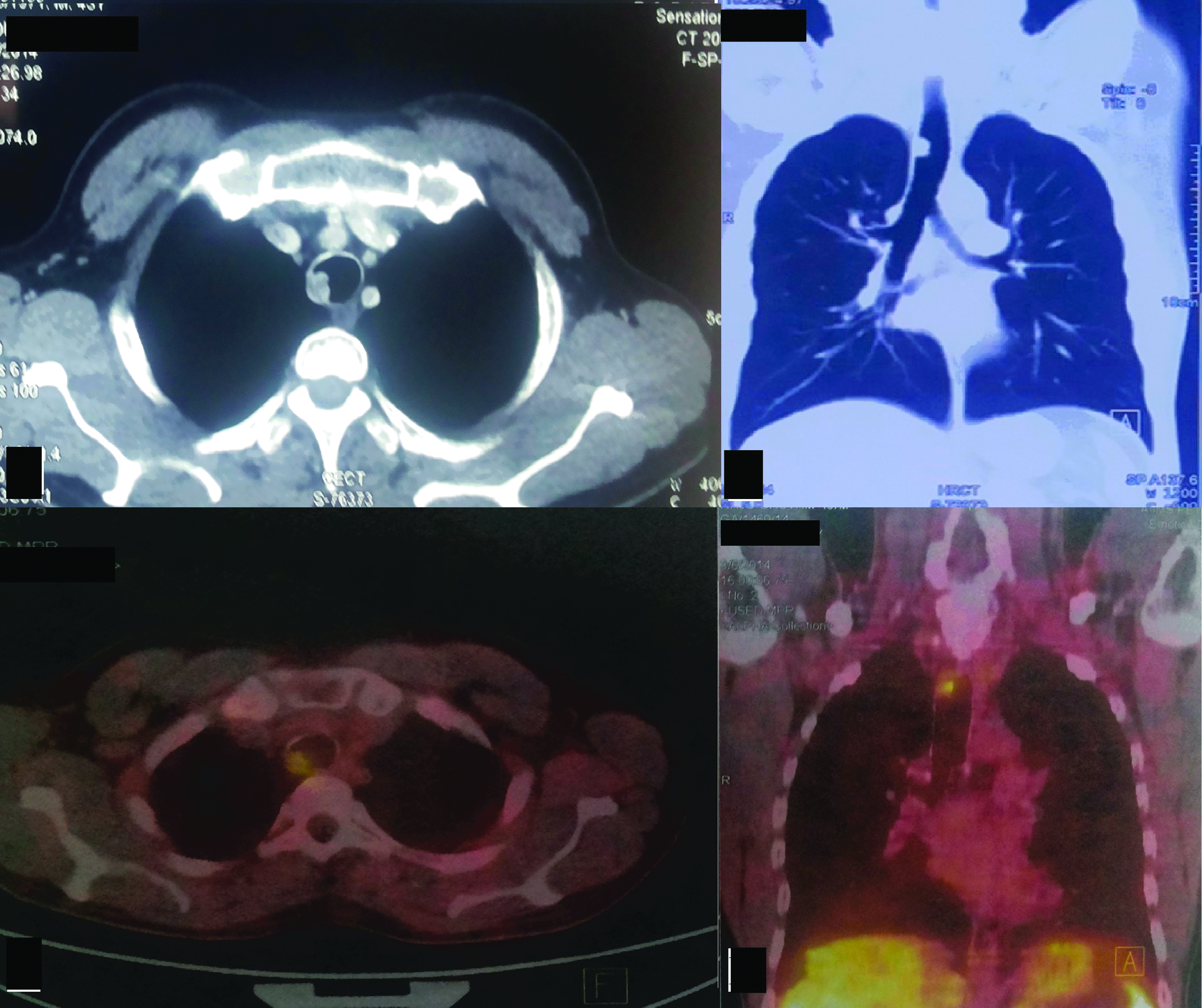
Computed tomography and Gallium-68 DOTATOC images showing uptake in tumor located at the posterior lateral of thoracic trachea.
Results
The patient was moderately built with body mass index of 23.15 kg/m2 (weight: 60 kg; height: 161 cm). The airway was secured by awake fiberoptic guided intubation, to avoid tumor disruption and bleeding. Cuffed microlaryngeal tracheal tube (MLT) (Mallinckrodt™, Coviden, Inc., Ireland) of size 5.0 was used for securing the airway, owing to its longer length for the given size. The lower end of the tube was lying above the tumor at this stage as illustrated (Fig. 2A). Then the patient was positioned to Rose's position (extension at cervical spine and extension at the atlantooccipital joint). Through a small vertical skin incision in the neck, strap muscles were dissected in the midline and retracted laterally to expose anterior tracheal wall. A vertical tracheotomy was performed in the midline and stay sutures are taken on either end of incised tracheal wall so that adequate retraction can be applied for endoscopic instrumentation.

Illustrations showing the location of the cuff of the endotracheal tube above the tracheal tumor in
The surgeon then sat at the head end of the patient and Hopkins telescope (0°, 4 mm and 14 cm) (Karl Storz GmbH and Co. KG, Tuttlingen) was introduced into the lumen of the trachea to visualize the tumor and its attachment. Under endoscopic visualization, the MLT was then carefully pushed further inside the trachea so that the cuff of the tube lies distal to the tumor as illustrated (Fig. 2B). Later, the cuff of the MLT was inflated with around 8 mL air, distal to the tumor to seal off the operating area, preventing entry of blood into bronchi (Fig. 3A).
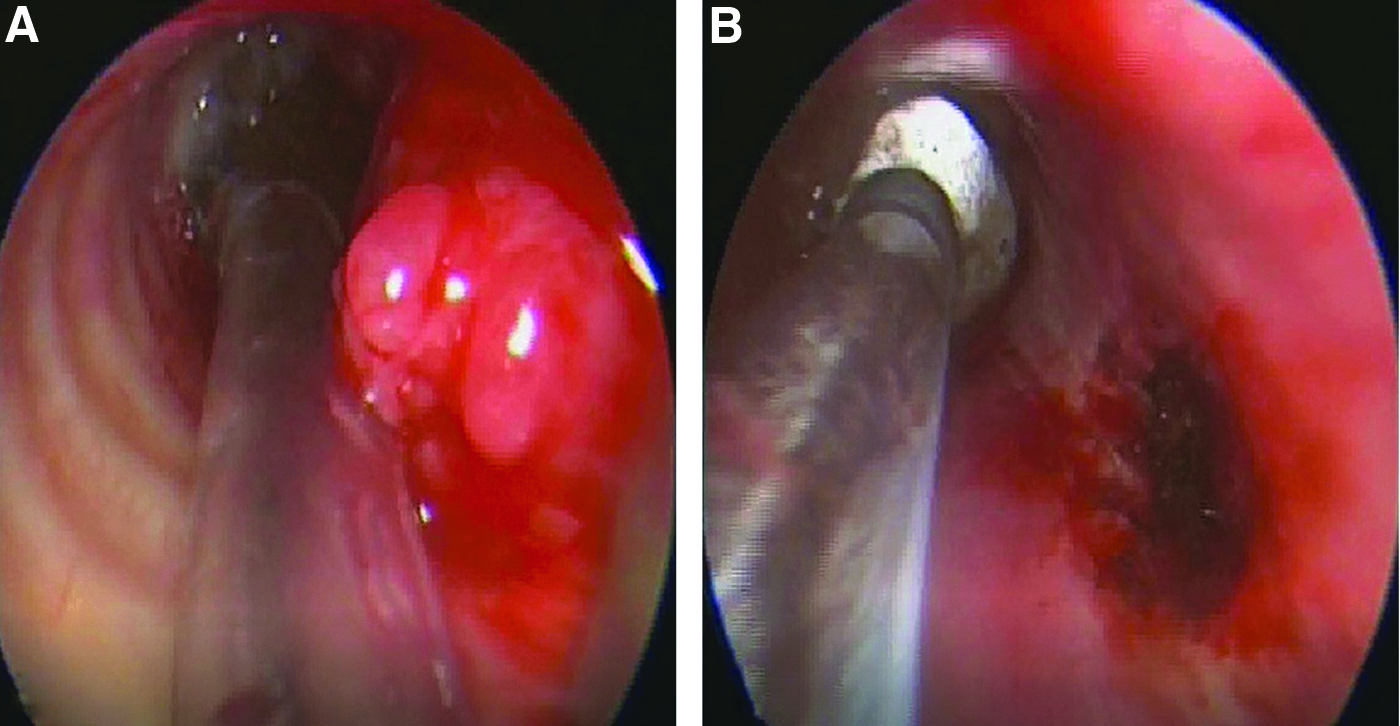
Intraoperative pictures as visualized using telescope passed through the tracheotomy. In
The tumor was removed in piecemeal, under endoscopic visualization and sent for histopathological examination. Skimmer airway blade of microdebrider (Medtronic) was used then to excise the rest of tumor tissue. Intraoperatively, the surgeon could hold the endoscope in the nondominating hand and cutting instruments or suction or cautery or skimmer in the dominating hand, as necessary. After hemostasis was secured using bipolar cautery, a thorough saline wash was given to clear of clot/blood stain from trachea above the inflated cuff and absolute hemostasis was confirmed by check endoscopy (Fig. 3B). The tracheotomy margins were approximated and the neck wound was closed in layers. Total duration of the procedure was 75 minutes, during which the patient was supported with following ventilatory setting. Ventilation mode was volume controlled ventilation with tidal volume of 450 mL, respiratory rate of 15/min, and positive end expiratory pressure of 20 cm H2O. The video showing the described procedure is provided in the link below. The patient had an uneventful recovery in the postoperative period and the histopathological examination was confirmatory of glomus tumor.
Discussion
The neoplasms of the trachea are rare and glomus tumor is the rarest among all the neoplasms of trachea. 1 Most of these glomus tumors of the trachea are conventionally managed by resection and anastomosis through transcervical approach, at times even requiring open thoracotomy.1–4 However, these open procedures have an additional risk of morbidity due to exposure of vital structures like cranial nerves, esophagus, major vessels rendering them vulnerable to injury during surgery. The transoral laser and robotic surgical approaches have already been the standard of care for benign lesions of larynx and oropharynx in most of the tertiary care centers. However, for the lesions of the trachea, transoral approaches may not be feasible due to narrow field available for instrumentation and visualization. The novel approach through percutaneous trans-tracheal route is a simple and less morbid procedure overcoming the disadvantages of transoral approaches.
In PTEA, the instrumentation through the tracheotomy is easy and better controlled. In contrast to suspension laryngoscopy, there is no constraint of a long and narrow tube through which manipulation of instruments could be difficult (Fig. 4). Similarly, the endoscope inserted through tracheotomy helps in better visualization of the lesion. In addition, the maintenance of anesthesia is easy in this approach as compared to intermittent apnea or jet ventilation techniques used in rigid bronchoscopic excision. 5 Percutaneous trans-tracheal approach has been used by some authors for providing jet ventilation in cases of anticipated airway difficulty during laryngoscopy. 6 However, most of these cases are biopsy procedures, done for laryngeal lesions. In contrast, we are describing PTEA for excision of tracheal lesions, with airway secured distal to the surgical site. The advantages of instrumentation through tracheotomy as compared to laryngoscope as explained earlier helps in efficient removal of the tumor. Theoretically, jet ventilation can be used in PTEA via a small catheter (maximum external diameter is 4.3 mm) passed distal to operating area through the MLT (5 mm internal diameter). However, it is not desirable due to following drawbacks. It has a potential risk of barotrauma, leading to pneumothorax or pneumomediastinum. Use of inhalational anesthesia is rather not practical with the jet ventilation and often the efficacy of gas exchange is not predictable. Also, there will be a hindrance for expiatory flow through MLT (due to the catheter) increasing risk of hypercapnia along with the difficulty in continuous monitoring of the end tidal carbon dioxide in jet ventilation technique. Alternatively, trans-tracheal jet ventilation through the tracheostoma can also be an option; however, this will also expose the lower airway to the surgical site increasing the risk of aspiration pneumonia, in addition to the other above-mentioned drawbacks.
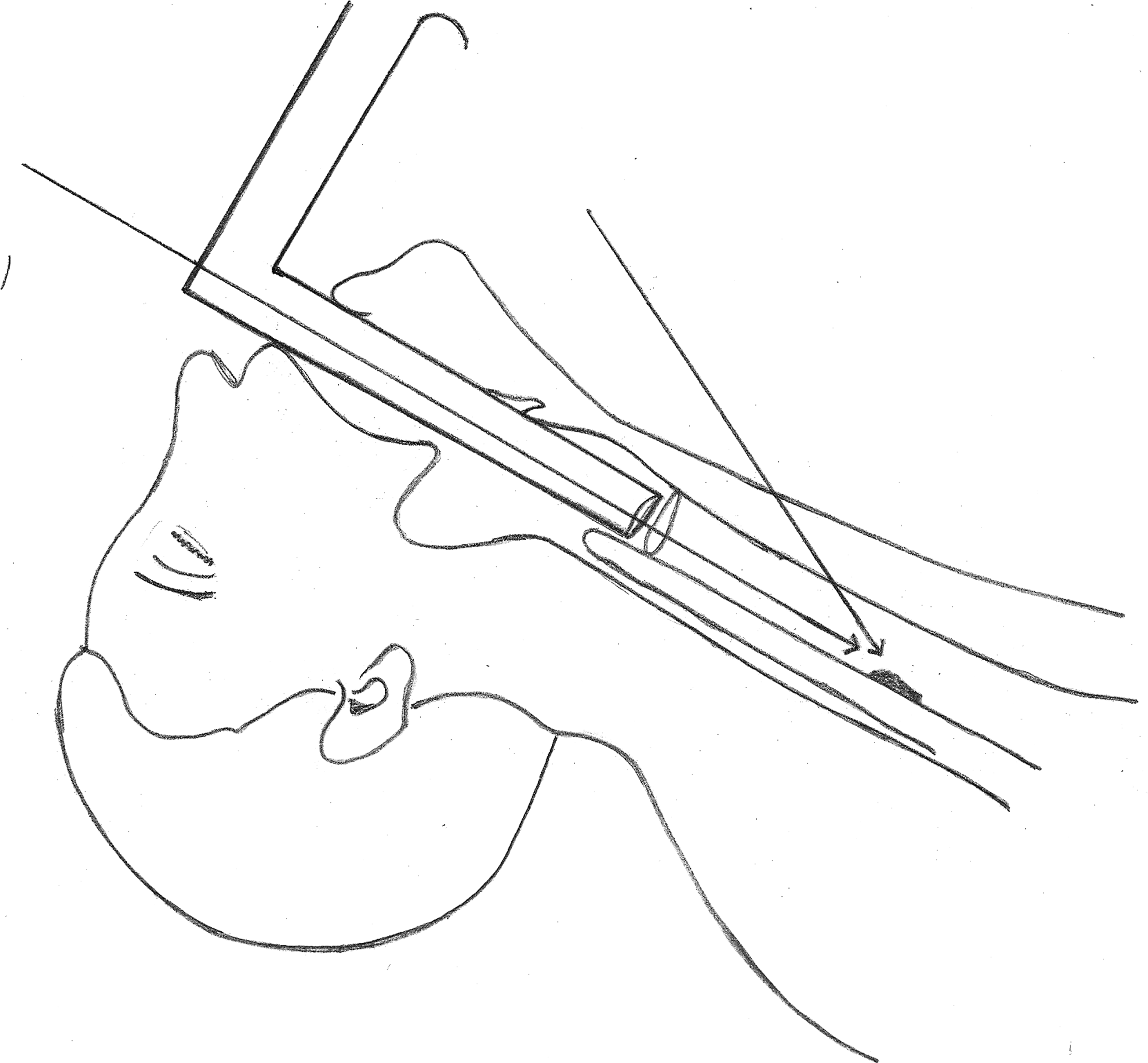
Illustration demonstrating the intraoperative difficulty in instrumentation through narrow and long transoral route as compared to transtracheal approach.
For similar lesions, flexible bronchoscopy guided excision using electrocautery and plasma coagulation have been described for patients not willing for surgery or not fit for general anesthesia. 7 However, the requirement of the equipment and the expertise are the constraints. There is also a risk of aspiration if the tumor starts bleeding while manipulation making this procedure undesirable. According to a report that analyzed more than 1000 diagnostic flexible bronchoscopies, the risk of complication has been reported to be 8%. 8 In another study, it was shown that risk of massive bleeding induced by therapeutic bronchoscopies and fatality were significantly higher compared to diagnostic flexible bronchoscopies. 9 The distinct advantage of PTEA over bronchoscopy (both rigid and flexible) is that the lower airway distal to the surgical area can be secured early in the course, reducing the risk of aspiration. For the same reason PTEA can be used for many benign and vascular lesions of trachea like paragangliomas, schwannomas, chondromas, and so on. This procedure can be used to effectively address the tracheal papillomatosis. The sealed cuff of MLT distal to operating area not only reduces the risk of aspiration of blood from vascular papillomas, but it also prevents the distal seedling of debrided pieces of papillomas. Rarely, PTEA can be of use while removing impacted tracheal or bronchial foreign body.
The procedure can safely be done by an experienced otolaryngologist or thoracic surgeon; however, it is preferable to have a team approach by involving both otolaryngologist and thoracic surgeon especially early in the learning curve and when the surgeon anticipates potential intraoperative difficulty like in an obese patient with a short neck, large tumor, etc. Appropriate planning and an efficient team consisting of an experienced surgeon, assisting staff, and anesthetist are the essential requisites for safely performing PTEA. Understanding and communication between these personnel are imperative preoperatively and intraoperatively.
There are some risks associated with PTEA that are to be kept in mind. There is a risk of cuff puncture and aspiration of blood, which can be minimized by keeping the operating area clear with repeated suctioning above the cuff. The suctioning should be gentle over the cuff to prevent any damage by the metallic suction tip. If the cuff ruptures intraoperatively, one should replace it by new cuffed tube through tracheotomy. Inadvertent damage to the tracheal wall is another concern, however, air leak through such tracheal tear is minimal, as the lower end of the anesthetic tube has been sealed off from the operation site. If any tear is noted intraoperatively, the patient is to be kept ventilated selectively for 2–3 days. Even pneumothorax in such situation can be managed conservatively unless it is rapidly progressive, in which case decompression is advised. However, considering the severity of probable complications, the surgeon should have the experience and the resources to manage them at the earliest. Along with the detailed informed written consent explaining all possible and probable complications before surgery, it is important to discuss with the patient and the relatives about all possible outcomes, including abandoning the procedure and/or staged excision of the tumor.
In summary, the novel approach of PTEA could be a simple and less morbid procedure in experienced hands. Theoretically, it has distinct and foolproof advantages over transoral and/or the transcervical approaches while excising benign luminal lesions of lower trachea. Further studies with more number of cases are needed to establish the utility and the safety of this approach. Although the procedure is potentially safe, the surgeon should have the capability and the facility to manage any untoward events.
Footnotes
Disclosure Statement
No competing financial interests exist.