
Abstract
Abstract
Objective:
The aim of this study is to assess etiopathogenesis of ureteral mid/lower benign strictures and outcomes of various methods of laparoscopic reconstruction and repair.
Materials and Methods:
We retrospectively reviewed the data of patients who underwent laparoscopic repair for mid and lower ureteral benign strictures at our department from January 2013 to February 2016. The demographic, operative, complication, and outcome data were analyzed.
Results:
Twenty-two patients were treated by various methods of laparoscopic reconstruction in the department of urology for benign ureteral strictures. Ureteroneocystostomy was done by psoas hitch in 15 and Boari flap in 2. Ureteral tapering, followed by ureteral reimplantation, was done in 2 and ureteroureterostomy in 3 cases. The most common predisposing factor that leads to ureteral stricture was prior pelvic gynecological surgery. Other causes included endometriosis, tuberculosis, impacted ureteral calculus, and ureteroscopic removal of calculus. Seventeen patients had lower, 3 had mid, and 2 had mid/lower ureteral strictures. Ureteral patency was successfully reestablished in all 22 patients without significant complications during a mean follow-up of 25 months (range 12–48 months).
Conclusion:
Laparoscopic treatment of benign ureteral strictures imparted excellent outcomes without major complications with the advantage of the minimally invasive technique.
Introduction
C
Materials and Methods
We retrospectively reviewed the data of patients who underwent laparoscopic repair of mid and lower ureteral strictures at our department from January 2013 to February 2016. Based on imaging, we included strictures of mid ureter, which overlies the sacroiliac joint, and lower ureter from lower border of the sacroiliac joint to the entrance into the bladder. We excluded patients who were managed for upper ureteral strictures. Twenty-two patients underwent laparoscopic reconstruction by various techniques during the mentioned period. During our time span of study, 27 cases of benign ureteral strictures were operated through open reconstruction and repair. As our study mainly concentrated on the laparoscopic approach of stricture repair, these cases were excluded. We assessed the underlying disorder, characteristics of strictures, treatment, and clinical course of patients (Table 1).
UNC, ureteroneocystostomy.
Preoperative evaluation included intravenous urography (IVU), retrograde pyelogram (RGP), computed tomography urography (CT urography) when needed, and antegrade nephrostogram where percutaneous nephrostomy (PCN) was present. Tc-99m diethylene triamine penta-acetic acid (DTPA) renal scan was considered in those patients when renal unit was not visualized. Sterile urine was confirmed before surgery. Fifteen patients underwent ureteroneocystostomy with psoas hitch, 2 patients underwent the Boari flap procedure, 3 patients underwent ureteroureterostomy, and in 2 patients, ureteral tapering and reimplantation were done.
Surgical techniques
Based on stricture location and length, definitive surgery was planned. All cases underwent surgery with similar basic surgical steps. Ureteroureterostomy was used in patients with mid ureteral strictures of length <2 cm. Ureteroneocystostomy with psoas hitch was used for lower ureteral strictures of length <4 cm. Boari flap reconstruction was used in 2 patients who had stricture length of 8 and 9 cm, respectively. Two patients with hugely dilated ureter were managed by intracorporeal ureteral tapering and reimplantation. Under general anesthesia, patients were placed in the supine position with 15°–30° Trendelenburg tilt. Initially, 10-mm trocar was placed at the infraumbilical site by the open method. Additional 5- and 10-mm working ports were placed according to the requirement.
Ureteroneocystostomy with psoas hitch
After adhesiolysis, posterior peritoneum over ipsilateral iliac vessels was incised and the ureter was identified. Ureteral mobilization was done till the pathologic segment, preserving adventitia. Stricture part was dismembered up to the proximal healthy segment. The distal unhealthy part was clipped with Hem-o-lok® clip or ligated with transfixation suture. The proximal healthy part was spatulated. The bladder was adequately mobilized and psoas hitch was performed in all cases. Detrusorotomy was done using electrocautery on the partially filled bladder. A submucosal tunnel of adequate length was created by blunt and sharp dissection. The mucosa was opened at the distal end of the tunnel. The spatulated ureter was sutured to the bladder mucosa by interrupted 4–0 polyglactin sutures over a ureteral stent. The detrusor muscle was buttressed over the ureter forming a submucosal tunnel using 3–0 polyglactin sutures as described by Lich-Gregoir (Fig. 1). The urethral catheter was removed on the 4th postoperative day (POD) and the pelvic drain was removed the next day, ensuring there was no increase in drain output.
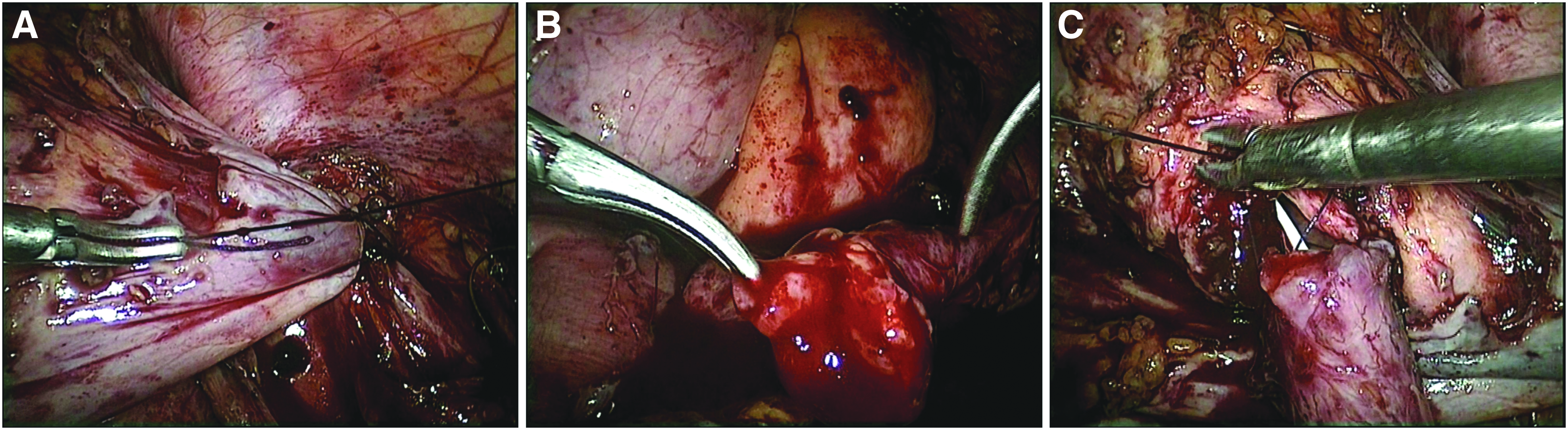
Intraoperative image depicting ureteroneocystostomy with psoas hitch.
Laparoscopic Boari flap reconstruction
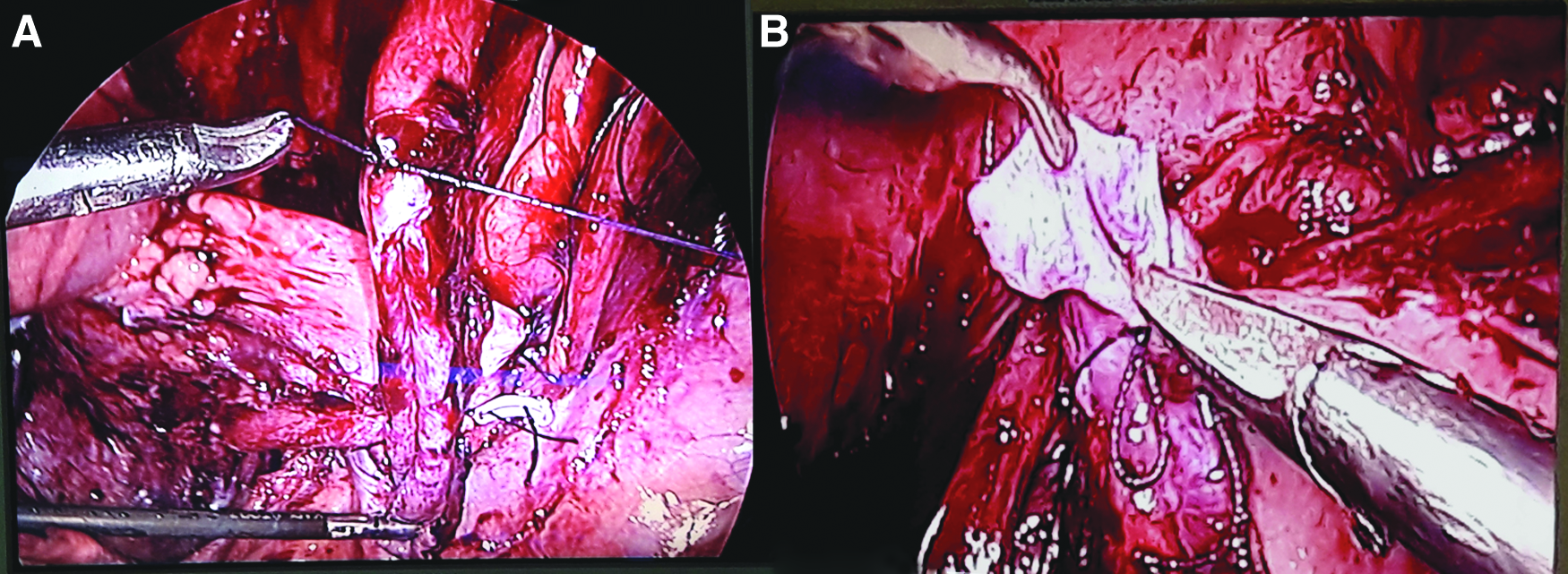
After ureteral mobilization, dismemberment, and spatulation of proximal healthy ureter, the urinary bladder was mobilized. As we could bridge the gap between the ureter and bladder, we did not ligate the contralateral superior vesical pedicle. The mobilized bladder was anchored to ipsilateral psoas muscle. A wide posterior-based bladder flap of length sufficient to bridge the gap between the ureter and bladder was elevated, preserving the blood supply. The spatulated ureter was anastomosed to the apex of the elevated bladder flap, ureteral stent was placed, remaining bladder flap was tabularized, and bladder defect was repaired with 3-0 polyglactin sutures (Fig. 2). Postoperatively drain was removed once the output was decreased to <20 mL in 24 hours. The urethral catheter was removed on 10th POD following cystogram if there was no leakage of urine.

Intraoperative image depicting Boari flap ureteroneocystostomy.
Laparoscopic ureteroureterostomy
Following ureteral mobilization, dismemberment, and spatulation, the ends of the ureter were anastomosed in a tension-free manner over a ureteral stent. The pelvic drain was removed once the output decreased to <20 mL in 24 hours, and the urethral catheter was removed the next day.
Ureteral tapering and reimplantation
In 2 patients, the left ureter was hugely dilated and tortuous because of idiopathic lower ureteral stricture. Ureteral tapering was performed and margins were approximated with 4-0 polyglactin sutures in a continuous manner. Bladder was hitched to the psoas muscle to alleviate the tension and mobility to the anastomosis. The distal end of the ureter was kept wide and anastomosed to bladder mucosa in a watertight manner over a ureteral stent (Fig. 3). Postoperatively, the drain and the catheter were managed as in the Boari flap procedure.
Intraoperative image depicting ureteral tapering and reimplantation.
Postoperative care and follow-up
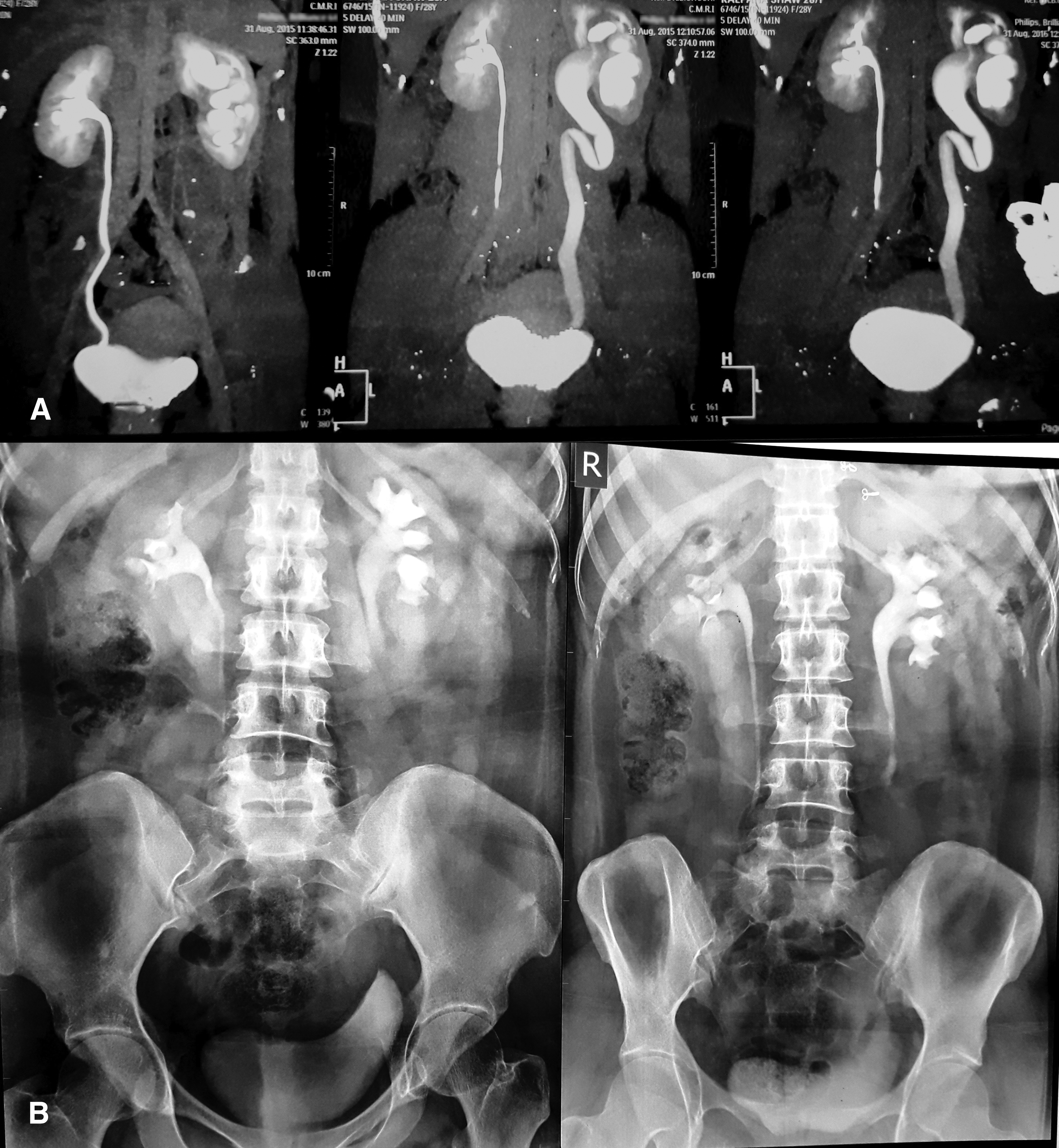
Double-J stent was removed after 4–6 weeks postoperatively in our outpatient operation theater. Complications were recorded according to the Clavien-Dindo grading system for classification of surgical complications. Follow-up was scheduled at 3 months postprocedure, which included the IVU study to check patency of anastomosis (Fig. 4), and voiding cystogram was performed in patients of ureteroneocystostomy to look for any reflux. Subsequent follow-up protocol included 6 monthly revisits for 2 years and yearly thereafter. Follow-up evaluation was done by clinical parameters, renal profile, and ultrasonography of KUB (kidney, ureter, and bladder). Surgical success was defined by improvement in symptoms, improvement in renal functions, and resolution/improvement in hydronephrosis. The demographic, operative, complication, and outcome data were analyzed.
Results
Twenty-two patients (19 females and 3 males) were treated in the Department of Urology for benign ureteral strictures. Among 19 females with ureteral stricture, the most common etiology was found to be iatrogenic injury due to previous gynecological surgery in 7 patients, followed by endometriosis in 3 patients. Among 3 male patients, 2 had undergone ureteroscopic removal of stone and 1 had impacted calculus. Sixteen patients had lower, 3 patients had mid, and remaining 2 patients had mid-lower ureteral strictures. The average length of lower ureteral strictures in 17 patients was ranging from 20 to 40 mm, whereas mid ureteral stricture in 3 patients had average length of 15–20 mm. Two patients had mid/lower ureteral stricture of length ∼80 and 90 mm following endometriosis and ureteroscopic removal of calculus, respectively. Table 1 depicts characteristics of various strictures along with the reconstructive laparoscopic procedure performed. The mean age was 36.18 years, mean body mass index (BMI) was 24.07, mean operative time was 170 minutes, and average blood loss was 115 mL. Planned laparoscopic surgery was successful in all but 1 patient with lower ureteral stricture following GUTB. In this case of lower stricture, due to the presence of dense fibrosis and poor vascularity, the decision to convert to open surgery was made intraoperative. The average hospital stay was 6 days. Table 2 summarizes the details and outcomes of the patients who underwent various laparoscopic reconstruction procedures. Three patients developed urinary tract infection that was managed with antibiotics according to urine culture sensitivity. In patients with ureteroneocystostomy, cystogram at 3 months revealed no reflux in 15 patients. Only 1 patient showed grade-1 reflux. Ureteral patency had been successfully reestablished in all 22 patients (100%) at a mean follow-up of 25 months (12–48 months). Except intraoperative time and intraoperative blood loss, there were no significant differences between the outcomes in different methods of ureteral reconstruction.
Ureteroneocystostomy
Boari flap reconstruction
ureteral tapering and reimplantation
ureteroureterostomy.
BMI, body mass index; EBL, estimated blood loss; ORT, operative time (port insertion to completion of the procedure); SD, standard deviation.
Discussion
Dramatic increase in incidence of ureteral strictures has occurred in recent years, largely as a result of the introduction and widespread use of upper urinary tract endoscopy.4,5 A 1%–11% incidence of stricture formation has been reported after upper tract endoscopy. 6 Various factors that can be attributed to development of ureteral strictures following ureteroscopy include stone impaction, proximal location of stone, large size of stone, relative ischemia often due to the use of larger scope size for prolonged intervals, ureteral injury with extravasation of urine, and direct mechanical or thermal trauma associated with the use of intracorporeal lithotripsy. 2 Stone impaction is a major risk factor; in a study, 24% of patients developed postoperative ureteral stricture where stone was impacted for an average 11 months. 7 In our cohort, trauma caused by impacted calculus and ureteroscopic removal of stone was associated with stricture formation in 6 patients (27%). Thorough insight of and acquaintance with ureter anatomy in various pelvic surgeries and proper selection of patients and instruments in upper urinary tract endoscopy are of paramount importance in preventing ureteral injury. With the exception of primary pelviureteric junction obstruction, most ureteral strictures are acquired and usually are iatrogenic. 8 Besides endoscopic upper urinary tract surgeries, open and laparoscopic surgical procedures may lead to stricture formation. Iatrogenic ureteral injury accounts for about 0.5%–2.5% during major gynecological surgeries. 9 In our cohort of patients, the most common cause of stricture was due to previous gynecological surgeries (32%). Before undergoing reconstruction surgery, urogenital fistulae were excluded owing to their common association with ureteral strictures caused by previous gynecological surgeries.
Other rare causes for ureteral stricture formation may include sarcoidosis, amyloidosis, schistosomiasis retroperitoneal fibrosis, abdominal aortic aneurysm, and endometriosis.10,11 Ureteral stricture as a sequel to GUTB is still prevalent in developing countries. In these countries, GUTB accounts for 15%–20% of cases of pulmonary tuberculosis in comparison with developed countries where it accounts for only 2%–10% of cases. 12 Ureteral involvement in tuberculosis may lead to fibrosis and stricture formation, which is most common in the lower ureter. In one series, it was found that healing of ureteral tuberculosis led to stricture formation seen in distal ureter in 56% cases, mid ureter in 13% cases, and multiple strictures in 17.19% cases. 13 Ureteral stricture as a sequel to GUTB is associated with both concentric and longitudinal fibrosis, pipe stem ureter, and poor vascularity. Laparoscopic mobilization of structures is usually difficult with a higher conversion rate to open surgery. 14 Laparoscopic reconstruction is technically feasible in GUTB as long as the defect length is small and the urinary bladder has adequate capacity to perform additional procedures such as psoas hitch and Boari flap to commensurate the gap between the ureter and bladder. Recent studies are also in favor of minimally invasive procedures for GUTB-associated ureteral strictures.15,16 During our study period, we encountered 4 cases of ureteral strictures as a sequel to GUTB. We successfully performed ureteroneocystostomy in 2 cases and ureteroureterostomy in 1 case. In 1 case of lower ureteral stricture, due to GUTB with dense fibrosis and poor vascularity, the decision to convert to open surgery was made intraoperative.
The presentation of ureteral strictures is very variable, ranging from mild hydroureteronephrosis to complete obstruction and loss of renal function. Clinical presentation of patients is also variable and may range from an asymptomatic individual with incidental finding of hydronephrosis to acute flank pain with sepsis and recurrent pyelonephritis. As the degree of symptoms correlates poorly with the degree of obstruction, the initial evaluation and treatment of patients with ureteral obstruction must be tailored to the clinical situation. Immediate decompression of the obstructed kidney is required in patients presenting with flank pain, persisting urinary tract infection or pyelonephritis, or in cases of solitary functioning kidney. Decompression may be done by internal stenting or external drainage by PCN tube placement.
Anatomical and functional evaluation of patients involves the use of ultrasonography, intravenous urogram, CT urogram, nephrostogram when PCN is present, and isotope renal scan. In suspected cases, RGP and ureterorenoscopy may be used to diagnose and assess the stricture characteristics. CT scan besides providing details about the urinary tract also provides an assessment of surrounding structures, which may be important in some patients with ureteral strictures especially in GUTB-associated strictures. Magnetic resonance urography is of value in assessment when intravenous contrast is contraindicated. 17
Indications for intervention include symptomatic ureteral stricture and the need to rule out malignancy and obstruction, which may threaten a patient's renal function. It is important to assess the renal unit for function before starting treatment for a reasonable success rate. Functional outcomes of treatment are mainly based on preoperative renal function. Renal function may improve in some patients after the obstruction is corrected; however, if the renal function is <10%, recovery is unlikely and nephrectomy may be the most appropriate treatment in symptomatic patients.
Depending upon stricture characteristics such as length, location, and renal function, surgical options vary from endoscopic to open or laparoscopic surgery. Balloon dilatation and endoureterotomy have less success rate compared with surgical treatment and the patient may eventually require surgery especially when overall renal function is poor (<25%), stricture length is more (>1 cm), and lumen stricture is tight (<1 mm). 8 The laparoscopic approach included ureteroureterostomy, ureteroneocystostomy with or without psoas hitch, Boari flap ureteroneocystostomy, or robot-assisted laparoscopic ureteral reimplantation with or without psoas hitch.18,19 Laparoscopic ureteroneocystostomy was first described in 1993 for treatment of vesicoureteral reflux. Although technically challenging, improvements in technology and technique have made this more feasible. Many studies compared the outcome between open surgical management for ureteral strictures with psoas hitch and Boari flap ureteral reimplantation and the results were comparable.20–22 In special situations where the ureter is hugely dilated due to ureteral strictures, ureteral tapering is required before reimplantation. In 2 of our cases, we successfully performed intracorporeal excisional tapering of hugely dilated ureter, followed by reimplantation with excellent outcomes. Agarwal et al. also found acceptable results in intracorporeal excisional tailoring of hugely dilated ureter, followed by laparoscopic ureteral reimplantation. 23 Outcomes of the surgical techniques are excellent in properly selected patients with appropriate surgical techniques based on ureteral stricture characteristics. Recurrent obstruction is the most significant long-term risk associated with surgical reconstruction of the ureter, and most stricture recurrences are identified within the first year of surgery. Clinical presentation of patients with stricture recurrence is considerably variable because of slow development of recurrent stricture. For this reason, extensive follow-up is required in the first year postsurgery to identify recurrent ureteral stricture by radiographic evaluation of the upper urinary tract. We had a strict follow-up protocol for patients, with clinical and renal functional parameter evaluation at each visit, including imaging in the form of IVU at 3 months, followed by 6-monthly ultrasonography for 2 years and yearly thereafter. Recurrent strictures, if detected early, may respond initially to endoscopic intervention, so endoscopic procedures should be considered before opting for surgical intervention. In our study with a mean follow-up period of 25 months, ureteral patency was successfully established in all the patients without major complications.
As with all retrospective studies, our study too has its own limitations, thus findings should be interpreted with circumspection. In our study, most of the patients were young and had mean BMI of 24.07 (range 20.2–28.5), which does not represent the whole population of the world. Although our study concluded that laparoscopic treatment of benign ureteral strictures imparted excellent outcomes without major complications, it is not a comparative study with open surgery, so true advantages in various variables cannot be stated.
Conclusion
Among various causes of strictures, ureteral calculus was found to be a common cause apart from iatrogenic injuries due to endoscopic procedures and complex pelvic surgeries. Management of benign ureteral strictures poses a diagnostic dilemma as well as tests the surgical skills of reconstructive surgeons due to varying stricture characteristics and patient factors. Laparoscopic reconstruction and reimplantation with or without psoas hitch or Boari flap are technically feasible with excellent results even in post-GUTB cases.
Footnotes
Disclosure Statement
No competing financial interests exist.