
Abstract
Abstract
Background:
Band slippage is known to be a troublesome complication of laparoscopic adjustable gastric banding (LAGB), often requiring surgical intervention. To prevent band slippage, a new auxiliary device “S-loop” was developed.
Methods:
From July 2010 to January 2014, a total of 814 LAGBs were performed by a single surgeon. The patients were divided into two groups based on the application of S-loop: conventional LAGB group (n = 378) and S-loop group (n = 436). The operative outcomes were compared between the two groups.
Results:
The mean operative time and the length of hospital stay were significantly longer in the conventional LAGB group than in the S-loop group (64.3 minutes versus 57.1 minutes; P < .001 and 5.0 hours versus 3.6 hours; P < .001, respectively). The complications occurred in 7.1% of the conventional LAGB group and 1.6% in the S-loop group (P < .001). Slippage was the most common complication: 13 cases were observed in the conventional LAGB group, whereas no slippage was observed in the S-loop group.
Conclusion:
Infra-band fixation using S-loop is a simple and effective method for preventing band slippage compared with the conventional LAGB.
Introduction
O
Bariatric surgery is currently considered the most effective treatment for obesity. It offers great weight reduction with high resolution of obesity-related comorbidities, which cannot be achieved by nonsurgical interventions.3–6 Of the available surgical options for obesity, laparoscopic adjustable gastric banding (LAGB) has been performed worldwide because of its effectiveness in weight loss and surgical safety in the short-term period.7,8 Accounting for 10% of all bariatric surgery in 2013, LAGB's adjustability and reversibility are the distinctive advantages above all merits, thus it still remains a good option for treating obesity in selective patients. 9
One of the current challenging issues facing LAGB is the high rate of long-term complication such as band slippage and erosion. Gastric band slippage is a troublesome complication, which can result in abdominal pain and dysphagia, often requiring surgical intervention. The rates of slippage have fallen dramatically over the past decade after changes of surgical techniques: from the perigastric to the pars flaccida approach method and gastrogastric suture to fix the gastric band.10,11 However, although gastrogastric suture has been used for preventing anterior slippage, its occurrence was not reduced but reported up to 8%.12–14
To prevent gastric band slippage effectively, a new auxiliary device “S-loop” was developed. Herein, we introduce this novel device and present the experience in a large group of patients.
Materials and Methods
Patients
This retrospective study was performed based on the prospectively maintaining database, and some patients' information was reviewed from the electrical medical records. From July 2010 to January 2014, a total of 814 patients underwent LAGB at the clinic for obesity, Seoul Slim Surgery. Of them, 629 patients have met the criteria for morbid obesity surgery: BMI ≥30 kg/m2with obesity-related comorbidity or BMI ≥35 kg/m2. 15 In 185 patients with BMI <30 kg/m2, LAGB was performed for weight control by the patients' request. Because S-loop was applied to the patients since May 2012, the patients were divided according to the band fixation method: the conventional LAGB group (n = 378) and the S-loop group (n = 436).
Informed consents were obtained from all patients before the operations and this retrospective study was approved by the Korean National Institute for Bioethics Policy.
S-loop for gastric band
The S-loop (the initial meaning: safety) is designed for minimizing the gastric wall injury caused by gastrogastric sutures. It is entirely made of silicone and consists of two parts: an easily distensible soft strap and a relatively hard loop (Fig. 1). The strap part is large enough to be joined with a gastric band and designed for providing flexibility between the gastric band and the loop part. The loop part is designed to be narrow for avoiding excessive tension and shape transformation after gastrogastric suture. The S-loop was issued for the Korean patent in 2010 (Patent number: 10-1329169), which was obtained in 2013 (PCT/KR2013/005093).

The feature and composition of S-loop.
Surgical procedure: infra-band fixation using S-loop
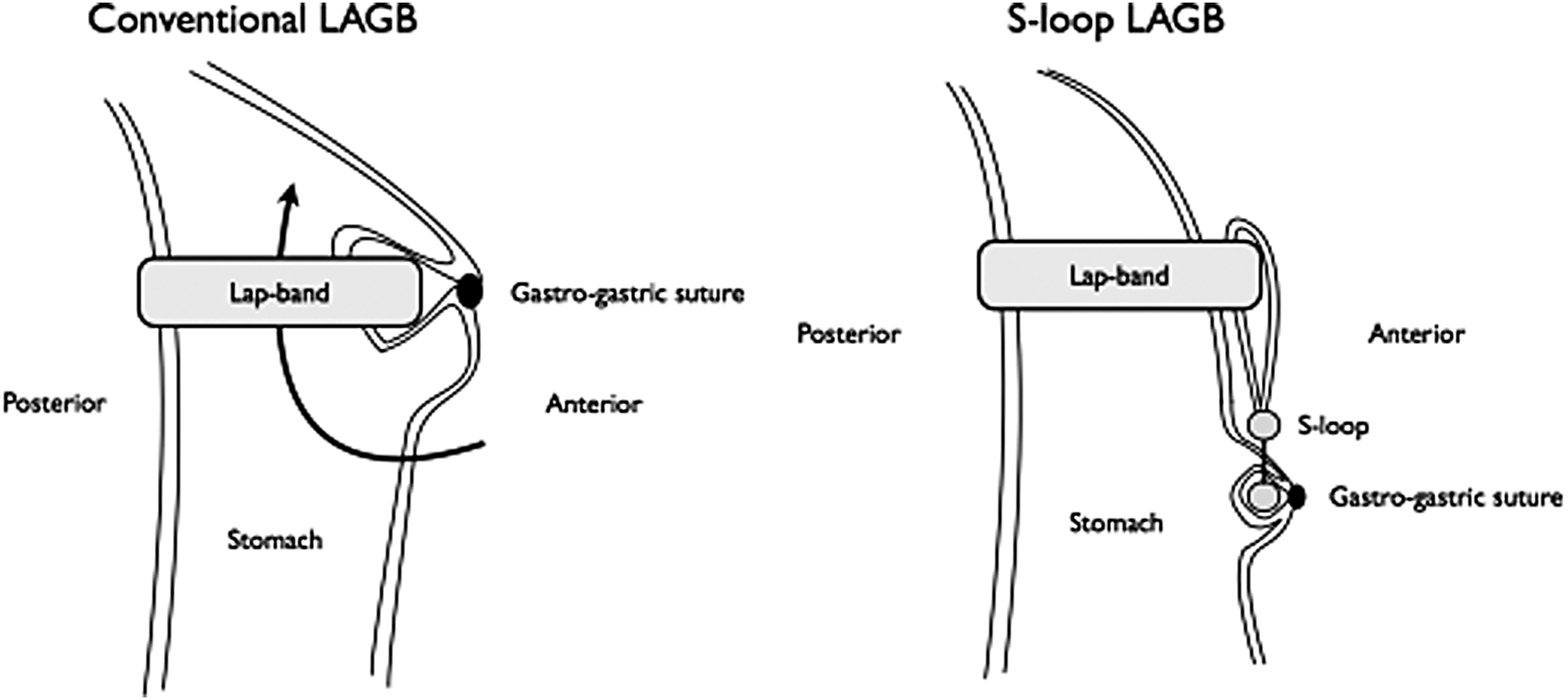
All LAGBs were performed by a single surgeon. Lap-Band® System AP small (LBAP, Allergan, Inc.) was used for both the conventional LAGB and the S-loop LAGB. All band positioning was performed through the pars flaccida approach. 16 After placement and buckling of the gastric band, four or five gastrogastric sutures were applied in all cases to fix the gastric band for preventing anterior slippage. Regarding the S-loop technique, S-loop was installed to the gastric band before buckling, then gastrogastric suture was performed only around the S-loop and not around the band (Fig. 2A, B).

Gastrogastric sutures in conventional LAGB and S-loop LAGB.
Band adjustment and follow-up
All band adjustments were performed by a surgeon (Y.C.P.) with the goal being the adjustments be optimized for the “green zone”, werein the patients experienced prolonged periods of satiety and weight loss, while minimizing any nausea or sensation of sticking.
Clinical assessments were performed at baseline and scheduled for every 1–2 weeks for the first postoperative month, 2–3 weeks for the second and third postoperative months, and semiannually or biannually thereafter. The assessments included body weight, body composition using bioelectrical impedance analysis, satiety and satiation, band adjustments, changes in medical history or comorbid conditions, changes in concomitant medications, any adverse events associated with the lap band, and upper gastrointestinal series. Gastroscopy was selectively performed when an erosion was suspicious.
Whether or not a band slippage occurred was evaluated every visit. An upper GI series was mostly performed to diagnose a band slippage and the c-arm device was also used to view the phi (φ) angulation of the band and a normal phi angle was considered between 4 and 58°.
Statistical analysis
Statistical analyses were conducted by SPSS software (version 18.0; SPSS, Inc., Chicago, IL). All data are shown as mean ± standard deviation or number and percentage. The χ2 and Fisher's exact test were used for categorical variables, and Student's t-test was used for continuous variables. A P value of <.05 was considered statistically significant.
Results
The preoperative characteristics and short-term outcomes are summarized in Table 1. The mean age of all patients was 34.3 years, women were dominant as 86.6% (705/814), and the mean preoperative body weight and BMI were 94.5 kg and 34.6 kg/m2, respectively. There was no significant difference between the conventional LAGB group and the S-loop group, especially in terms of BMI and comorbidity. The most common comorbidity was hypertension, followed by fatty liver and amenorrhea. Type 2 diabetes was observed in 9.1% of all patients.
Data are presented as number (%) or mean ± standard deviation.
LAGB, laparoscopic adjustable gastric banding; BMI, body mass index; DM, diabetes mellitus.
The short-term and long-term outcomes are summarized in Table 2. The mean operative time including anesthetic time and the length of hospital stay was significantly longer in the conventional LAGB group. The overall complications occurred in 7.1% (27/378) of the conventional LAGB group and in 1.6% (7/436) of the S-loop group, which was statistically significant (P < .001). Slippage was the most common complication, which was observed in 13 cases of the conventional LAGB; however, slippage did not occur in patients with S-loop. Early leakage occurred in 2 patients who underwent conventional LAGB. The median follow-up period was 22 months in the conventional LAGB group and 19.1 months in the S-loop group (P = .126). During the follow-up period, a reoperation was needed in 32 patients mostly due to the complications. Band removal was performed in 12 patients (7 in the conventional LAGB group and 5 in the S-loop group); however, four of five band removals in the S-loop group were determined by patients' request without evidence of any complication.
Patients who followed up postoperatively are presented as numbers and percentages.
Data are presented as number (%) or mean ± standard deviation
LAGB, laparoscopic adjustable gastric banding.
Discussion
One of the most common complications of LAGB is the band slippage. It is caused by prolapse of the lower stomach part through the band, so the proximal portion of the stomach is dilated and intragastric space is narrowed, sometimes completely blocked. An immediate operation for band repositioning or removal is usually needed to prevent further damage to the stomach, as the stomach can be ischemic because of insufficient blood supply.14,17,18
Recently published data indicated that the rate of slippage has dramatically improved over the years. This has been predominantly facilitated by the pars flaccida approach, which has largely reduced the incidence of posterior slippage.19–21 The other contributing factor for reducing band slippage might be a suture for band fixation.11,22,23 Several gastrogastric sutures are commonly used for fixing the anterior portion of the gastric band. This technique is classically based on the hypothesis that strong fixation would prevent band slippage. However, recent studies demonstrated that the results of the gastrogastric suture were not satisfactory.12,13 This implicates that the classic hypothesis may be wrong and a new method for preventing slippage is needed.
Our belief is that band slippage can be prevented if the infra-band stomach is grasped with the band, because the lower part of the stomach can rotate on the gastric band even after gastrogastric sutures (Fig. 3). Thus, we believe that suturing the supra-band stomach may not be helpful but that suturing the infra-band stomach is needed. The S-loop was designed to fix more inferior part of stomach away from the gastric band. As from our experience, infra-band fixation using S-loop has given satisfactory results, especially in terms of incidence of slippage. Thirteen slippages occurred in the conventional gastrogastric suture method, whereas no slippage occurred in this new method using S-loop. In addition, there was no early leakage, which is caused by iatrogenic injury of the band during gastrogastric sutures. We assume that these remarkable results originated from several advantages of the S-loop: (1) double fixation by the gastric band and S-loop may be more resistant to slippage, (2) minimized gastrogastric sutures may reduce the tension of stomach wall, and direct compression of suture site and early leakage can be avoided, (3) unnatural shape transformation caused by gastrogastric suture can be avoided, and (4) iatrogenic vessel injury during sutures can be avoided because fixation site is more inferior than the conventional method. Large vessels are crowded around the esophagogastric junction that is the main cause of bleeding during the conventional gastrogastric sutures, which might result in vascular compromise and early leakage.
The principle of S-loop for preventing slippage of the band.
This study had several limitations. First, there is the potential for confounding given the study design and analyses. Second, it is a single institution study and, therefore, patients could have gone to other institutions with band-related problems. Third, because S-loop was applied to the patients since May 2012, the S-loop group showed better short-term outcomes in operative time and the length of postoperative hospital stay. These results are thought to be mostly due to the learning curve effect, which might also affect the result related to a surgical technique such as access port-related complication. Finally, weight changes and resolution of comorbidities were not analyzed in this study because this study aimed to focus on the technical report and its feasibility.
Conclusion
In conclusion, we believe that infra-band fixation using S-loop is a simple and effective method for preventing band slippage compared with the conventional LAGB based on our experience.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Footnotes
Disclosure Statement
S.Y. Son has no conflicts of interest or financial ties to disclose. Y.C. Park has Korean and U.S. patents for the S-loop device.