
Abstract
Abstract
Background:
There is a movement toward cost savings in healthcare worldwide. Surgeons can affect two main cost variables in an operation (controllable cost): disposables and time. Our hypothesis is that increasing disposable costs do not change outcome or operative time, but simply increases controllable cost.
Methods:
We retrospectively reviewed patients younger than the age of 18 years undergoing laparoscopic appendectomies for nonperforated appendicitis from January 2013 to November 2016. Data obtained included demographic information in addition to intraoperative details, including disposables used and associated cost, resident participation, operative time, and final pathology. Patients were excluded if perforation was present as confirmed by operative findings or pathology (Kansas City definition). Patients were also excluded if concurrent procedures were performed during the appendectomy.
Results:
We reviewed 918 patients and excluded 288 for a total of 690. Disposable cost, operative time, and complications were compared between cases with a resident present and those without. Residents did not increase the use of disposables, but did increase operative time and therefore the total controllable cost. Transumbilical laparoscopic-assisted technique was significantly faster with lower controllable cost when compared with all other methods. Using disposable trocars with an endostapler was the second fastest and second lowest controllable cost and retained a significant difference when compared with most other methods. Endoloop methods did not show overall controllable cost savings versus the vast majority of methods.
Conclusions:
To maximize controllable cost savings, we recommend a transumbilical laparoscopic-assisted appendectomy or a standard three-port laparoscopic appendectomy, with disposable trocars and the endostapler.
Introduction
I
Surgeons are uniquely positioned to both understand and impact the costs associated with surgical procedures.2,4 A study on surgeons' choice of instrument use during an appendectomy showed that the increased cost of disposable instruments could influence the overall procedure cost and often surpassed the reimbursement for that procedure. 4
Appendectomies are one of the most common surgical procedures for both the pediatric and general population.5–7 The laparoscopic approach to the appendectomy has been established as an accepted approach that optimizes patient safety, quality, and cost.8,9 Therefore, analyzing the cost of the laparoscopic appendectomy can offer additional insight into overall surgical healthcare spending. 10
At our institution, laparoscopic techniques for pediatric appendicitis include transumbilical laparoscopic-assisted approaches, traditional three-incision procedures, and nearly every option in between. In addition, surgeons utilize any combination of various staplers, endoloops, disposable, or reusable trocars with or without energy devices—all without the explicit direction of administration. The aim of this study was to further analyze the effects of the use of disposable instruments on operative time, complications, and overall controllable cost. Controllable cost is defined as disposable instrument cost combined with operative cost, which was operative time multiplied by the cost per minute. We hypothesized that increasing disposable instrument costs does not change outcome or operative time, but simply increases controllable cost.
Methods
Patient charts were retrospectively reviewed through electronic medical records, including surgeon operative reports, hospital charge codes, and progress notes, at an American tertiary children's hospital and its community-based sister hospital from January 2013 to November 2016. All patients were younger than 18 years of age and were undergoing laparoscopic appendectomies for nonperforated appendicitis. Data obtained included demographic information in addition to intraoperative details, including disposables used—endostaplers, endoloops, LigaSure™ (Covidien, Zelienpole, PA), Harmonic® (Ethicon, Cincinnati, OH), clips, hook cautery, disposable or reusable trocars, and Endobag™ (Covidien) or Endo Catch™ (Covidien), their associated costs, resident participation, operative time, and final pathology.
Due to the numerous methods (49 in total) used by multiple, different surgeons, the eight most common approaches were analyzed and compared. Perioperative complications within 30 days of their operation were also analyzed. Patients were excluded if they were older than the age of 18 years, if they had concurrent procedures performed at the time of the appendectomy, or if it was an interval appendectomy or perforated. We defined perforation using the Kansas City definition (perforated by operative or pathology report), a visible hole in the appendix or a fecalith found within the abdomen.
The data were analyzed by our Biostatistics Department using SAS for Windows®, 9.3 Cary, NC software. Complications were analyzed with Pearson's Chi-square test wherever possible (expected frequency >5), otherwise, Fischer's exact tests were used. Continuous variables were analyzed with either Wilcoxon rank sum tests or Kruskal-Wallis tests. The Dwass-Steel-Critchlow-Fligner Method for pairwise two-sided multiple comparisons was used, and P-values<.05 were considered statistically significant.
Results
There were 918 patient charts reviewed with 439 excluded for a total of 479 patients. Patients were excluded if the appendix was perforated, if they had an interval appendectomy or a concurrent procedure during their operation, or if they were not within the eight methods analyzed. The median age was 12 (range 3–17). The mean body mass index (BMI) ± standard deviation (SD) was 21.0 ± 5 (Table 1). There were 208 females and 271 males. The patient population was 78% Caucasian, 3% Asian, 5% African American, and 14% other, which is similar to our hospital population (Table 1). Patient comorbidities were identified from the chart such as history of cancer, diabetes, asthma, heart disease, irritable bowel, gastroesophageal reflux disease (GERD), or Celiac disease, but were not considered impactful on the outcome or speed of the case.
Median age in years reported along with range. Mean BMI is reported with the standard deviation (BMI could not be calculated for 61 patients due to incomplete records).
Outcomes for operative time, length of stay, and estimated blood loss (EBL) are listed below. Operative time was defined as incision to closure. Length of stay was preoperative admission to discharge.
BMI, body mass index; OR, operating room; SSI, surgical site infection.
The median operative time was 37 minutes (12–89 minutes). Median length of stay was 1.44 (0.28–13.1) days (Table 1). The maximum length of stay of 13.1 days was a patient with a new diagnosis of acute lymphoblastic leukemia that developed acute appendicitis during his hospitalization. There were 17 different attending surgeons found to have performed the surgery, but three pediatric surgeons performed the vast majority of cases (68%).
Most cases had resident involvement, 342 (71%) versus 137 (29%) that did not. The majority of cases had minimal blood loss recorded [≤9 mL, 474 (99%)]. The maximum blood loss was 20 mL, and those documented with greater than minimal blood loss were only 5 patients and not considered significant (Table 1). Complications were also evaluated. We found 12 patients with intra-abdominal abscess formation (2.5%), 6 with surgical-site infection (1.3%), 9 developed an ileus (1.9%), 2 patients developed pneumonia (0.4%), one patient with a bladder injury (0.2%), and 16 patients developed other complications (3.3%). However, there were not enough occurrences from which to draw meaningful conclusions about associated complications (Table 1).
There were many different appendectomy methods utilized with too few observations to discuss with significant meaning, consequently, only the eight most frequent methods were examined, which constituted 69% or 479 of the total cases. These were then labeled as Group A through H based on their total disposable cost ordered, least costly to most expensive.
Group A consisted of reusable trocars only, which was considered the transumbilical laparoscopic-assisted approach, described as an open cutdown Hassan approach (5 or 10 mm), placing the camera through that reusable trocar and then inserting an instrument through the fascia next to the camera port, grasping the tip of the appendix, incising the fascial bridge between the instrument and camera port, and suture ligating it extracorporially (45 patients); Group B, disposable trocars, hook cautery, and endoloops (52 patients); Group C, disposable trocars, hook cautery, endoloops, and Endo Catch (106 patients); Group D, disposable trocars and endostapler (69 patients); Group E, disposable trocars, endostapler, and Endo Catch (69 patients); Group F, reusable trocars, Harmonic or LigaSure, and endoloops (47 patients); Group G, reusable trocars, Harmonic or LigaSure, endoloops, and Endobag (57 patients); and Group H, reusable trocars, Harmonic or LigaSure, endostaplers, and Endo Catch (34 patients) (Tables 2 and 3).
Each group is described by entry method used, hemostasis method, how the base of the appendix was controlled, and whether or not a removal bag was used and the type.
Each group had a baseline cost, the basic laparoscopic tray plus the cost for any additional instruments, such as an endostapler or endoloop, and so on. Operative cost was calculated by the cost per minute of use. Controllable cost was calculated by combining instrument cost with operative cost. Group A used extracorporeal cautery for hemostasis and suture to ligate the base of the appendix, and these costs were considered trivial and not included in the analysis.
All groups had a baseline cost of a basic laparoscopic tray and since Group A used no disposables, this was considered the baseline instrument cost (Fig. 1). Group B and C, with disposable trocars and endoloops, had lower instrument costs than group D, which used endostaplers and disposable trocars. Operative time was considered time from incision to closure and as mentioned previously, Group A had the shortest operative time. Operative cost was calculated by the time per minute in the operating room (OR) and the cost of each minute. Controllable cost was the sum of instrument costs and operative costs. Group A had the lowest controllable cost followed by Group D. Groups B and C, while having lower instrument costs, did not have lower controllable cost. Groups B, D, and F were not statistically significantly different from each other. Both Groups D and F had higher instrument costs, but faster OR time and Groups B and F both used endoloops. There were not enough complications within these methods to compare the methods on complication rates (Table 3).
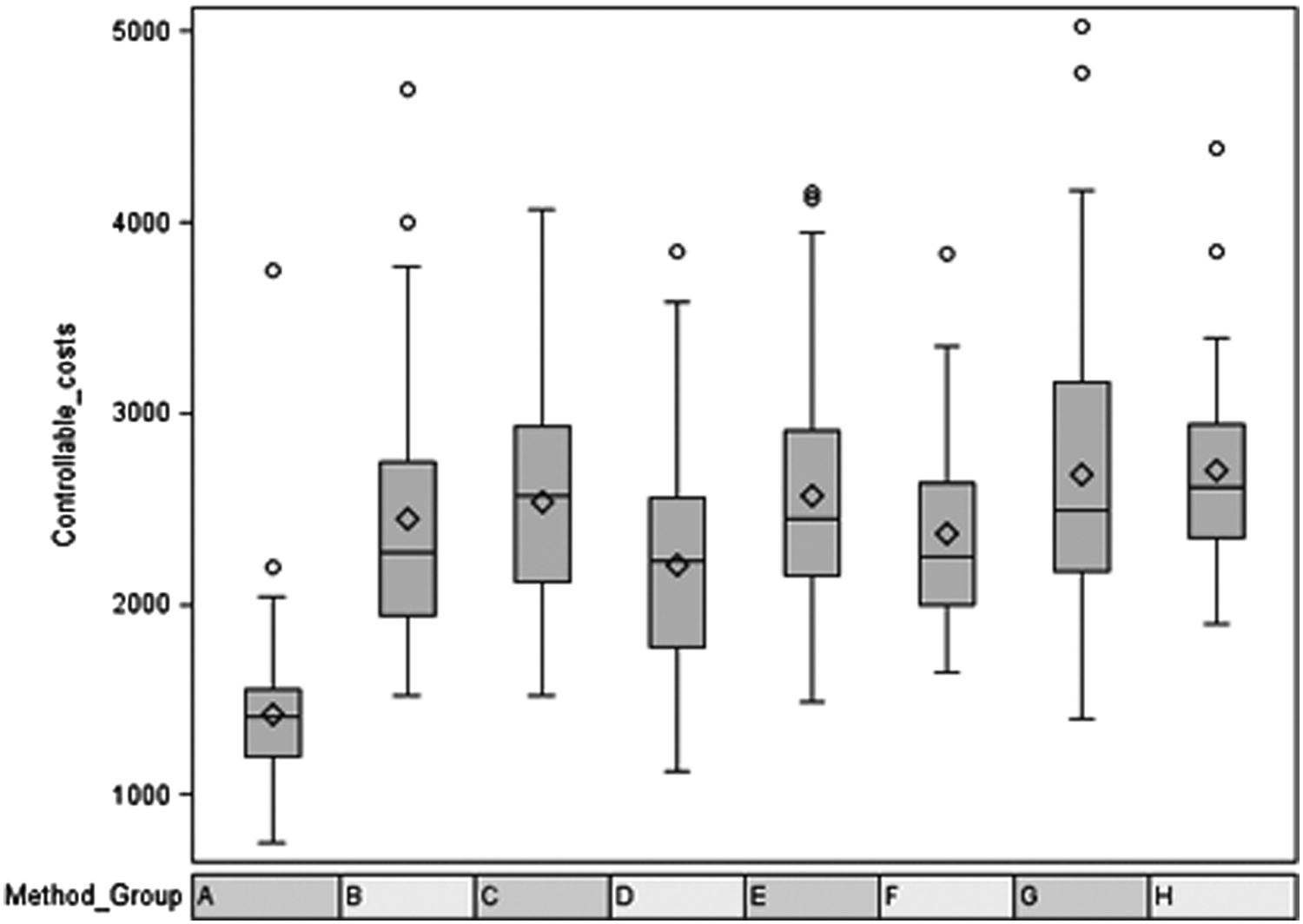
Distribution of controllable costs by group.
Transumbilical laparoscopic-assisted approach (Group A: reusable trocars only) was faster and had significantly lower controllable cost when compared with all other methods (P < .0001). Using disposable trocars and the endostapler (Group D) was the second fastest and second lowest controllable cost and retained a significant difference when compared with most other methods. While the median cost difference between Groups C and D (endoloop and staplers, respectively) was only $36, endoloop methods did not show overall controllable cost savings versus the vast majority of methods when the entire dataset was taken into consideration.
Disposable instrument cost, operative time, and complications were compared between cases with a resident and those without. Residents did not increase the use of disposables, but did increase median operative time (39 versus 34 minutes) and therefore the total controllable cost (P < .0001). There were not enough complications to make any meaningful statements about residents and complications.
Table 4 was included to assist surgeons in weighing the cost of a disposable instrument as a relative value when compared to time. The total cost of the instrument was divided by the operative time cost. This table ignores any possible complications associated with or prevented by the instruments and also the time to application, if applicable. The Endobag essentially costs 0.3 minutes of OR time, whereas the endostapler, depending on the type of stapler, size, and how many loads were used, could cost up to 15 minutes of OR time. Each endoloop costs much less OR time (0.2 minutes), although when application time was taken into account, the endoloop groups did not provide a statistically cheaper method when compared with the vast majority of other groups.
The value is obtained by dividing the cost of the instrument by the OR time cost. When weighing the utility of a disposable instrument, this table helps surgeons understand how much time needs to be saved to justify the use of specific disposable instruments (from a pure cost standpoint).
Discussion
With the cost of healthcare in the United States rising, it becomes increasingly important to find savings without compromising patient care. Eliminating the use of expensive disposable instruments or increasing the speed of the operation while doing so safely could be a way to decrease healthcare costs. In this study, we found that a transumbilical laparoscopic-assisted approach (Group A: reusable trocars only) with using a reusable trocar via the umbilicus and bringing the appendix up through that incision was the least expensive in terms of disposable instrument use, but also the quickest operation, making it the most cost-effective appendectomy operation (P < .0001).
Confounding factors must be considered, including that operative time may be influenced by patient size, mobility of the appendix, and the severity of the appendicitis. We attempted to control this bias by excluding perforated cases, but it is possible that larger patients who were not selected to undergo the transumbilical laparoscopic-assisted approach may have been more difficult, take longer, and therefore cost more. Wound infections have shown to be a concern in the transumbilical laparoscopic-assisted method and could therefore increase cost. 11 However, we had zero wound infections in this technique. The disposable trocars and endostapler appeared to have sped up the operation by allowing faster control of the appendiceal mesentery enough to compensate for the cost of the trocars and stapler. This is beneficial for larger patients and when single incision is not possible. Surprisingly, despite endoloops being much cheaper than the endostapler, the time of cauterization of the mesentery and application of the endoloops outweighed the cost savings.
One limitation of our study is its relatively small number of patients. Since the majority of the cases were done by three surgeons, surgeon skill could influence operative time and therefore surgeon controllable cost by technique. In addition, there was variance in technique even by surgeon (i.e., many surgeons performed multiple methods of removal). In addition, given the retrospective nature of this review, there may have been some selection bias in the transumbilical laparoscopic technique by surgeon preference and patient characteristics.
We did find that residents increased the operative time enough to significantly increase the overall cost of the operation. However, we feel strongly that surgeon training is vitally important and a slight increase in costs despite being statistically significant (P < .0001), far outweighs this drawback and should not be eliminated.
We are moving toward standardization to the lower cost methods at our institution. However, this is for the routine easy pediatric appendectomy, and the authors would like to emphasize that when there is concern for safety or increasing OR time, more costly disposable methods may be justified. Applying the most cost-effective method to all is potentially dangerous, given nuances of each patient and surgery. We do contend that education on costs could help decrease spending in surgical healthcare. Since the conclusion of the study, some surgeons have been performing the single incision more often, whenever it is safe to do so, in an effort to reduce cost, and we are encouraging others to follow suit.
In summary, we determined that disposable instruments can influence cost and operative time. We advocate for the use of the transumbilical laparoscopic-assisted technique or traditional three-port appendectomy with disposable trocars and endostapler whenever clinically appropriate. Further studies could be done with a randomized prospective, multi-institutional trial to gain enough power to better evaluate complications to compare the different disposables and to study each surgeon individually.
Footnotes
Disclosure Statement
No competing financial interests exist.