
Abstract
Abstract
Introduction:
Magnamosis forms a compression anastomosis using self-aligning magnetic Harrison rings. The device has been approved by the Food and Drug Administration for first-in-human testing and has been applied in adults for intestinal anastomosis during urologic reconstructions. We now report the first cases of magnamosis to functionally undivert the fecal stream from a previously created loop ileostomy in pediatric patients.
Materials and Methods:
Case 1: A 4-year-old male underwent a diverting loop ileostomy for malignant bowel obstruction. The obstruction gradually resolved with chemotherapy, and persistently high stomal output and malnutrition prompted undiversion. Case 2: A 16-year-old female with iloecolonic polyposis underwent ileoproctectomy with J pouch and diverting ileostomy. The magnamosis functional undiversion (FUN) technique involves introducing a Harrison ring through each stomal limb under general anesthesia with X-ray guidance. Magnets are each tied with sutures that exit the stoma and are then tied to each other externally. The device is removed when patency is detected.
Results:
The introduction procedure took less than 20 minutes and there were no complications. Enteral feeding was initiated 24 and 6 hours postoperatively, and distal passage of stool occurred by the fourth and fifth days, respectively. Magnets were removed 14 and 15 days postoperatively, without evidence of leak.
Conclusion:
We conclude that the magnamosis undiversion procedure is a safe, minimally invasive way to gradually refunctionalize the excluded distal bowel after previous diverting ostomy.
Introduction
M
Materials and Methods
Patient selection
Case 1
A 4-year-old male was diagnosed with a ruptured liver tumor during exploration for an acute abdomen. The tumor was extensive, invading the portal vein, the spleen, the gallbladder, the diaphragm, and the inferior vena cava. Tumor biopsy showed hepatoblastoma, and a CT scan revealed bilateral lung metastases. The patient evolved with persistent symptoms of partial bowel obstruction so he was taken for exploratory laparotomy. Tumor had extended into the right colon at the hepatic flexure causing large bowel obstruction, so a diverting loop ileostomy was created. In the weeks that followed, during chemotherapy, he presented with very high ileostomy output and was started on parenteral nutrition. A gastrointestinal contrast study was performed showing tumor remission and relief of the intestinal obstruction with adequate passage of contrast. Due to the critical condition of the patient, characterized by malnutrition and thrombocytopenia, the decision was made to undivert the ostomy in an attempt to improve the patient's nutritional status without requiring a conventional ostomy takedown.
Case 2
A 16-year-old female with ileocolonic polyposis underwent ileocoloproctectomy with J pouch and diverting side-to-side loop ileostomy. She was expected to have perineal skin problems after refunctionalization since over 30 cm of ileum had been resected and she had a high stomal output. A magnetic functional undiversion (FUN) procedure was proposed to the family as a first step in bowel reconstruction.
Technique
Parental and institutional approval was obtained after detailed description of the procedure.
The magnamosis FUN technique involves introducing a Harrison ring through each stomal limb 5 cm deep from the skin under general anesthesia with X-ray guidance to check for a correct magnet alignment. Magnets are each tied with nonabsorbable sutures that exit the stoma and are then tied to each other externally (Fig. 1). The device is removed when patency is detected.
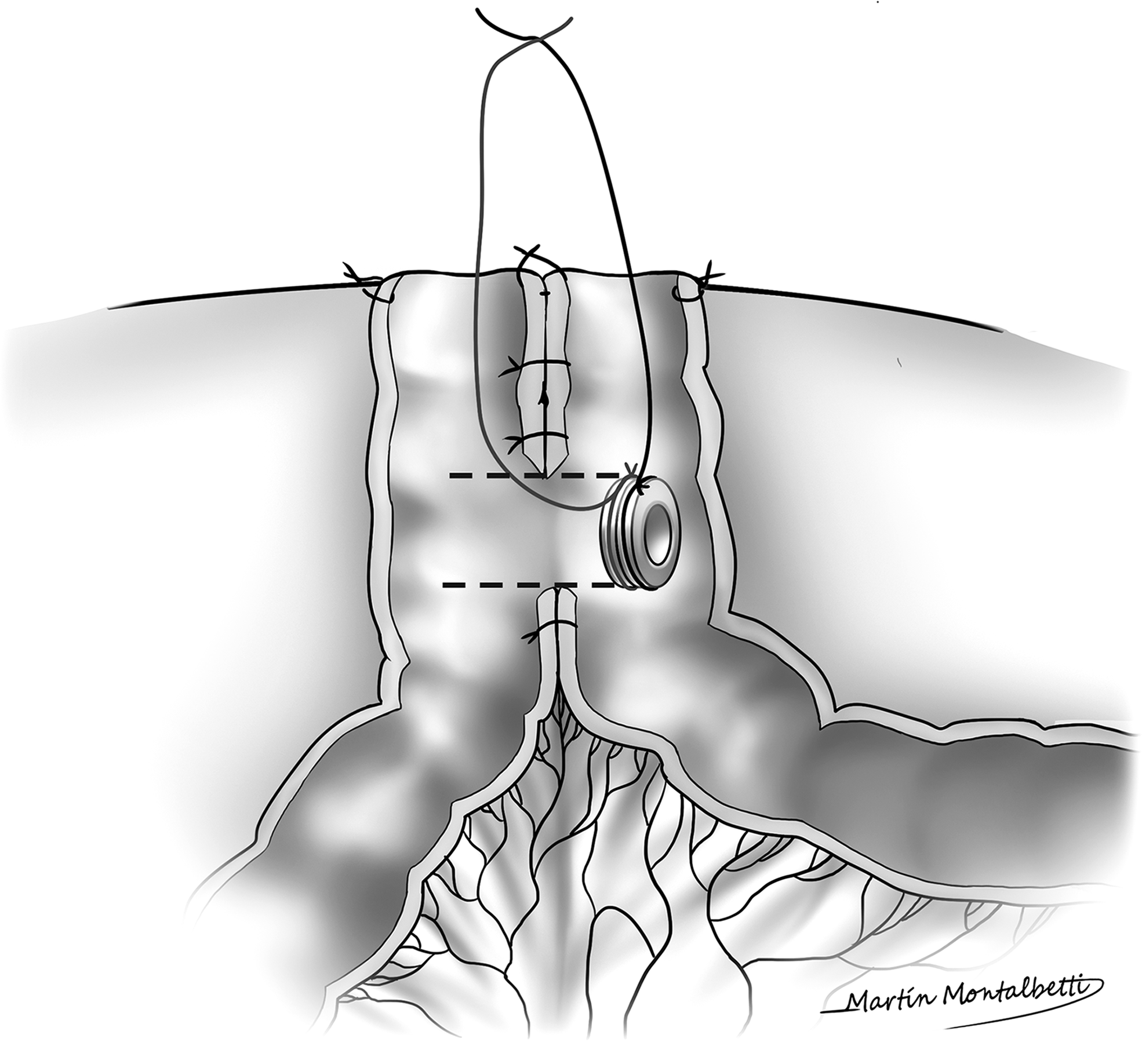
Magnamosis undiversion technique: A side-to-side small bowel ostomy is demonstrated. Sutures fix both sides of the proximal and distal bowel loops, so that mesentery is confined to one side, rather than between the two loops of the bowel. The magnetic anastomosis is created by placing two Harrison rings, tied to two nonabsorbable sutures, ∼5 cm deep from the skin. Both sutures are tied together outside of the stoma. After anastomosis formation, the Harrison magnets pass through the distal loop and can be retrieved with the string.
Results
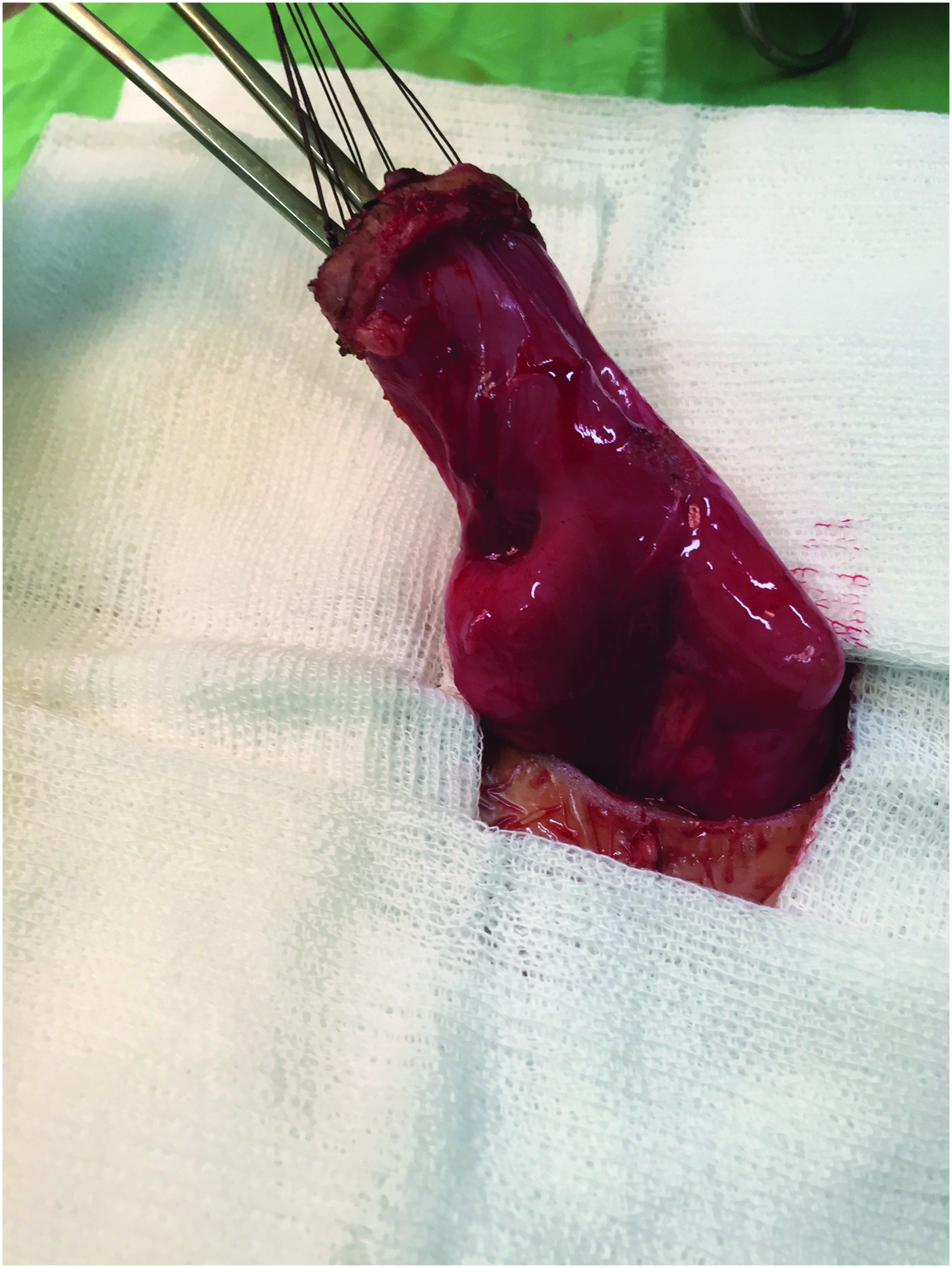
In both cases, placing and mating the magnets took less than 20 minutes, and there were no complications. They were performed under general anesthesia with X-ray guidance. Enteral feeding was initiated 24 and 6 hours postoperatively, and passage of stool through the anus occurred by the fourth and fifth days, respectively. Magnets were removed 14 and 15 days postoperatively, with no evidence of leak or any other complication (Fig. 2).

Removal of the mated magnets through one of the stomal limbs, done at the office.
In case 1, enteral nutrition was advanced and parenteral nutrition discontinued. Chemotherapy proved successful and the extrahepatic tumor disappeared, so the patient underwent cadaveric liver transplantation with a choledochal anastomosis. The magnetic anastomosis was left in situ and was closed by stitching shut the “chimney” opening. During follow-up, the patient presented with symptoms of bowel obstruction. At exploratory laparotomy, the obstruction, secondary to adhesions, was found to be well proximal to the ileal magnamosis, which remained patent. At 5 months posttransplantation and stoma closure, he remains tumor free, continues with chemotherapy, and is tolerating exclusive enteral nutrition.
In case 2, after the FUN procedure, the ostomy output decreased from 4 to 1.25 L/day. She started having 15 highly acid stools a day, so intense preventive local perineal measures were undertaken. Three months later, as the stools improved in number and quality, thanks to dietary adjustments and high-dose loperamide, the stoma was taken down (Fig. 3). She had a favorable outcome without burns in the perineal area or infections at the stoma site.
Ostomy takedown in case 2. Magnamosis is shown 5 cm deep from the stomal chimney.
Discussion
The magnamosis device has been tested in over 60 pigs in a variety of gastrointestinal sites and has proven that it generates stronger anastomoses than handsewn or stapled ones.1,5–7 After FDA approval, five adult patients have had successful magnetic compression anastomoses using the magnamosis device during bladder augmentation procedures. All had side-to-side, and functional end-to-end small bowel anastomoses without complications. 4 In this study, we describe a novel procedure: FUN of a loop ileostomy created by magnetic compression anastomosis (Fig. 4).
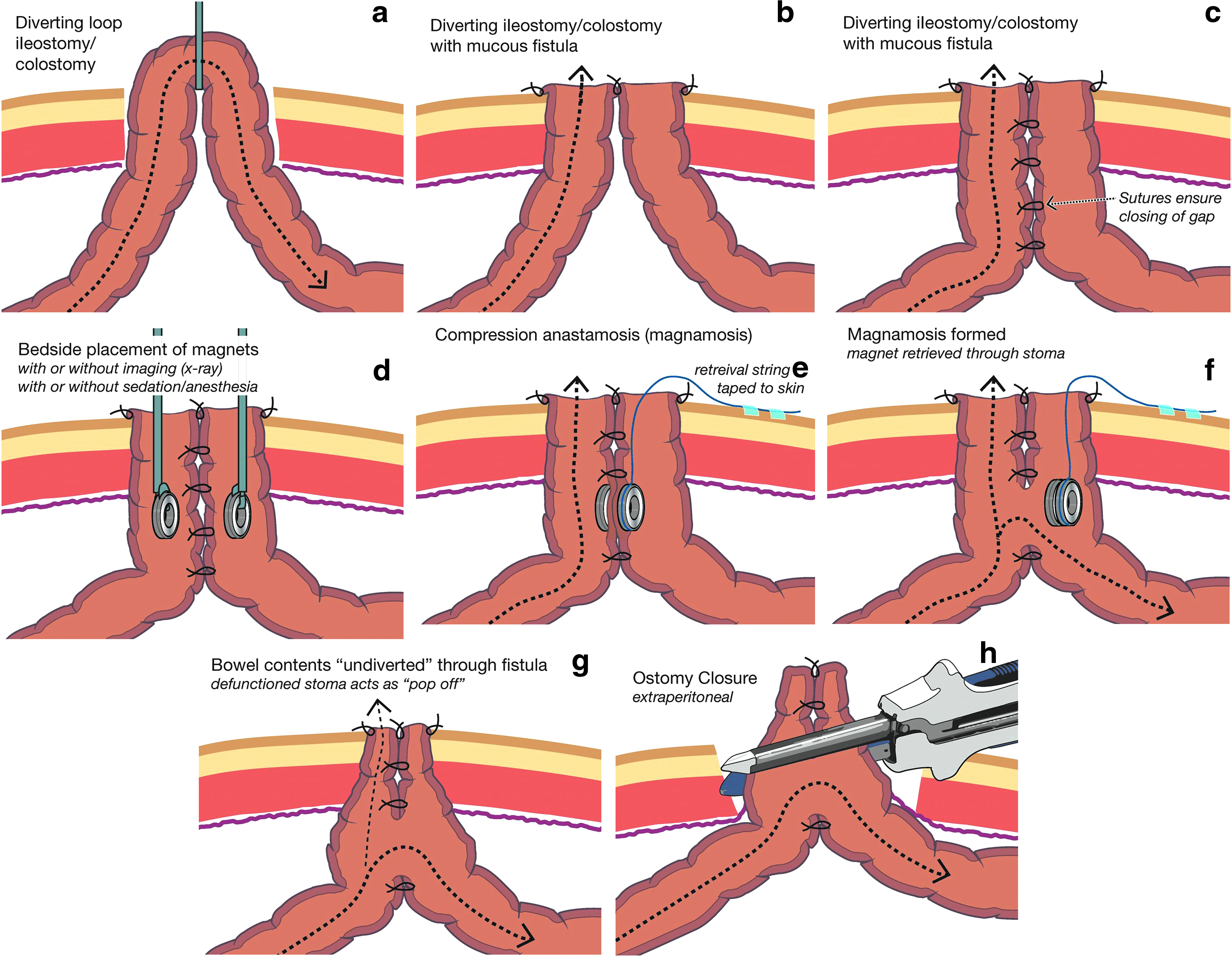
Steps of FUN procedure.
These are the first reported cases of magnetic undiversion of an ostomy in either humans or animals. This procedure can be compared with others designed to allow distal bowel functionalization like Bishop-Koop or Santulli procedures. All these techniques have the advantage of permitting distal passage of content while maintaining a “pop-off valve” if the bowel does not function properly. In our practice, we sometimes opt for functional ostomies in patients in whom we think closure might have complications, so magnamosis is an interesting option to consider in these cases. In the first patient, we did the FUN procedure only a month after the stoma creation, and we did not trust the large bowel to be completely patent. On the other hand, it became necessary to consider refunctionalization of the excluded bowel (i.e., defunctionalization of the ostomy) to optimize the patient's poor nutritional status. Magnetic compression anastomosis became a very attractive option since we could increase bowel absorptive surface while keeping a pop-off valve, and without requiring tissue dissection and surgical handling of the ostomy. In the months after the magnetic undiversion, fecal matter tended to pass through the anastomosis rather than out of the ostomy and allowed for resumption of enteral nutrition. In the second patient, FUN allowed for a gradual refunctionalization for a transient short bowel syndrome caused by extensive resection of rectum, colon, and distal ileum. It was a less invasive way to facilitate adaptation to her new intestinal absorptive condition.
These are also the first pediatric cases of magnamosis. We have proved the procedure is feasible in children, and we had no complications. Although the 23 mm magnets were appropriate for use even in a 4-year-old child, it is unlikely that younger children are amenable for those magnets in terms of diameter. We have developed a variety of magnamosis sizes from 8 to 30 mm diameter to accommodate essentially any surgical indication.
Although studies in swine of the magnamosis device, the anastomoses were formed and the rings excreted after 5–7 days on average, it appears that it takes longer to pass the mated magnets in these first human cases, about 12–15 days. These time lapses have proven the same both in children and in adults. We are exploring the use of stronger magnets to achieve more rapid anastomosis formation.
Regarding technique, if magnamosis undiversion is being considered, the surgeon should tack the antimesenteric serosal surfaces of the stomal limbs together when constructing the diverting loop ostomy. This preventive measure would eliminate the possibility of having mesentery trapped between the two limbs when the magnets are placed. However, failure to do this should not be limiting, since the rings are applied manually, and their final location can be determined by the surgeon by palpation and X-ray. Although in our cases we deployed the magnets in the operating room with general anesthesia to achieve adequate abdominal muscle relaxation, we think bedside deployment of the magnets may be possible if the patient is relaxed, since the procedure is painless.
We conclude that Magnetic FUN is a safe, minimally invasive procedure that gradually refunctionalizes the excluded distal bowel after previous diverting ostomy. These are the first pediatric cases of undiversion using the magnamosis device.
Footnotes
Disclosure Statement
M.H. is the inventor of the Magnamosis system and founder of Magnamosis, Inc.