
Abstract
Abstract
Introduction:
Nuss bar removal after minimally invasive repair of pectus excavatum in patients where bar ends are not palpable, can be a challenging procedure for the surgeon; a blind dissection toward the bar edges may lead to intercostal vessels or deep intercostal muscle injuries. In this article, we describe a fast, repeatable, low-cost technique to detect bar edge and stabilizers.
Methods:
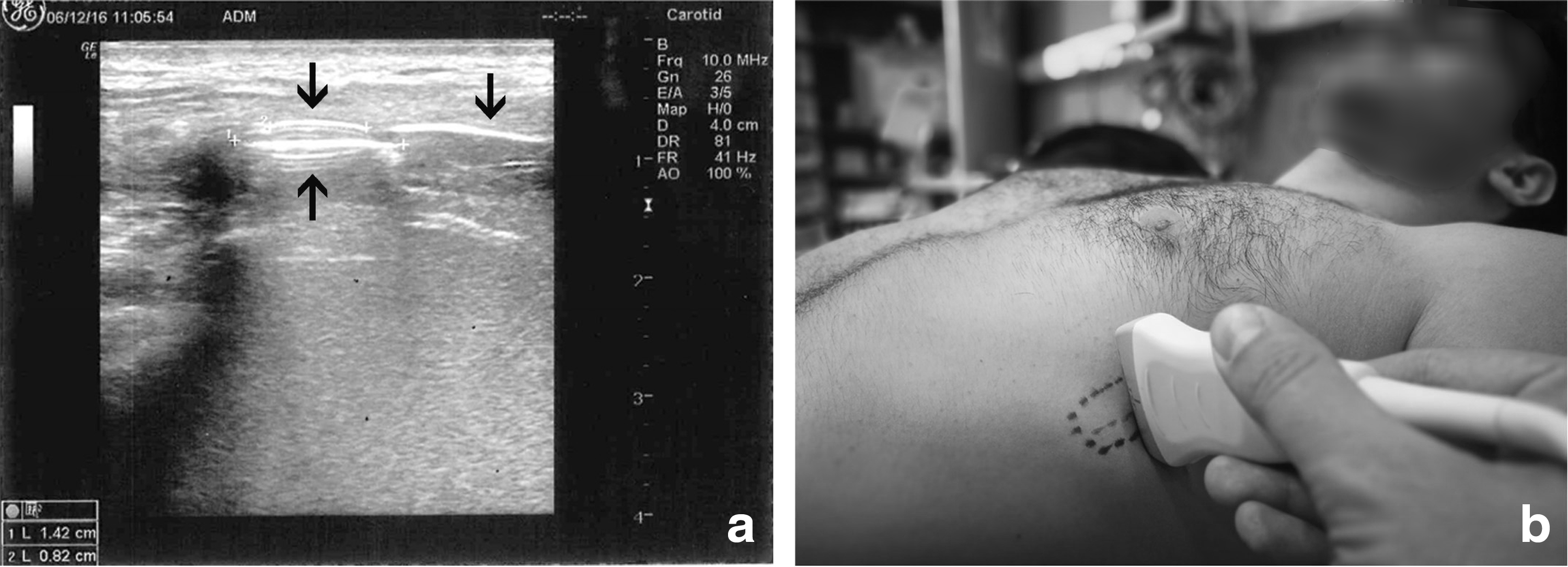
A perioperative scan is performed by means of a portable ultrasonograph a few minutes before the operation. The bar edge stabilizer is detected as a hyperechogenic image with a concentric crescent while the bar edge is detected as a hyperechogenic dashed line with net edges. The scan is performed, and the actual projection on the skin of the metal plaque bulk is then labeled on the patient's chest by an ink marker.
Conclusions:
We believe that this method may improve morbidity, operative time, and consequently, hospitalization length and costs.
Introduction
T
Ultrasound is a bed-to-side, repeatable, low-cost technique that has already been used in patients who underwent MIRPE with the purpose of evaluating compression on internal mammary arteries to assess flow obstruction and to monitor the introducer edge during the bar insertion procedure.6,7 We hypothesized that ultrasound may play a role to identify and label bar edges in the perioperative assessment to make the procedure quicker and safer; this concept may be relevant especially for those patients whose bar edges are not clearly identified at palpation. Herein we describe a strategy that allows to clearly identify bar edges in patients who undergo implant removal procedure.
Technique
A perioperative scan is performed by means of portable ultrasonograph (Logiq e - General Electric, Co., Fairfield, CT) a few minutes before the operation. The patient is recumbent, and the chest is exposed. The operator, visualizing the scar in one hemithorax, handles the chest wall looking for the bar end and the stabilizer, whenever present. The probe type is chosen according to the patient's anatomical features, skin thickness, and age. In most of the cases, especially in slender patients, a linear probe (8.0–10.0 MHz) is placed onto the scar following longitudinal, oblique, and transversal orientation. The bar edge stabilizer is then detected as a hyperechogenic image with concentric crescents, while the bar is detected as a hyperechogenic dashed line with net edges (Fig. 1a). The bar, as previously described, may be followed up to the contralateral scar even in its intrathoracic passage, with the probe kept in transverse and longitudinal position (Fig. 1a). If the operator is unable to follow up the bar from side to side, especially in the part under the sternum, for better penetration it is possible to use a convex probe (5.0 MHz), although details will appear less magnified. By means of the same technique, the procedure is repeated on the opposite side where either the bar end or the bar end stabilizer is detected (Fig. 1b). As the scan is performed, and the actual image is projected on the skin, the metal plaque bulk is then labeled on the patient's chest by an ink marker.
Discussion
To date, peri- and intraoperative localization of stabilizers is based only on palpation of the metallic bulk, which in selected cases might be difficult because it is embedded into fibrotic and osseous tissue, dislocated from the scar, and difficult to ascertain from actual ribs. 8 A safe exposure of the bar edge with minimal morbidity in some cases may be challenging for the surgeon; when a blind dissection is performed, operative time increases and dissection toward the bar edge stabilizer may lead to intercostal vessel damage or possible deep intercostal muscle injury, which in turn increases postoperative pain control and recovery.
In this article, we reported a quick perioperative strategy to promptly localize the metal implant. Moreover, within an additional few seconds, by means of the same technique it is possible to detect, at the same time, internal mammary artery flow, the presence of pleural effusion, and lung “sliding” sign as in pneumothorax.3,4
Although a double cohort prospective study is still warranted to justify this procedure as a routine approach, we believe that with such simple expedient, operative time and morbidity as in blood loss, postoperative pneumothorax, postoperative pain, and eventual hospitalization could be improved for those patients whose implant is barely detected when about to be removed.
Footnotes
Acknowledgment
We express our utmost gratitude to Stella Leng for her contributions.
Disclosure Statement
No competing financial interests exist.