
Abstract
Abstract
Background:
Single-incision laparoscopic surgery (SILS) was introduced to further the enhanced outcome of conventional multiport laparoscopy (CML). We compared their short- and long-term outcomes in colorectal surgery.
Materials and Methods:
Retrospective review of patients who underwent elective laparoscopic colorectal surgery during 3-year period. Patients' data, surgery outcomes, and oncological results were compared.
Results:
Sixty-one patients (33 male, 28 female), mean age 67.4 years, underwent laparoscopic colonic resections: 28 SILS and 33 CML. Twenty-three (37.7%) patients had previous abdominal surgery. There were 19 (31.2%) right, 9 (14.7%) left, and 2 (3.3%) total colectomies, 16 (26.2%) sigmoidectomies, 13 (21.3%) anterior and 2 (3.3%) abdominoperineal resections. Colonic malignancy was a main indication for the surgery in 51 (83.6%) patients. Mean surgery time and postoperative stay were 92.0 minutes and 9 days, respectively. Pathological examination revealed stage I colon cancer in 16 (32%), stage II in 22 (44%), stage III in 10 (20%), and stage IV in 2 (4%) patients. Mean number of retrieved lymph nodes was 19 ± 13.5. No differences were found between groups in demographic data, type of surgery, surgery time and hospital stay, pathological results and tumor staging, and disease-free and overall survivals. In the SILS group, placement of additional trocar was required in 7 (25%) and conversion in 3 (10.7%) cases compared with 1 (3%) case of conversion to formal laparotomy in the CML group. Overall postoperative morbidity was 16.4%. There was no mortality in both the groups. During the study period, 3 patients from the CML group had cancer recurrence.
Conclusions:
SILS is a feasible and safe technique compared with CML in terms of surgical and oncological outcomes.
Introduction
T
The aim of this study was to compare the short- and long-term outcomes of both techniques in colorectal surgery.
Materials and Methods
A retrospective review of prospectively collected data from January 2014 to November 2016 of patients who underwent elective laparoscopic surgery for colorectal pathology was performed. Patients' data, surgery outcomes, and oncological results of SILS and CML were compared.
All cases were done by the same surgeon (B.K.) experienced in laparoscopic surgery for more than 20 years. We decided using SILS for surgery requiring organ resection and additional incision for specimen removal (gastrectomies, small bowel resections, colectomies). We performed first SILS colectomy in February 2014; however, on a regular basis we started it from March 2015, due to economical restrictions of the hospital. Herein, we summarized our first experience and learning curve using SILS in colorectal surgery and compared with CML.
CML was done by four-trocar technique. All SILS procedures were performed using the GelPOINT®device (Applied Medical, Rancho Santa Margarita, CA) using standard laparoscopic instruments. A 45° camera was used in all cases. Extracorporeal anastomosis was performed in both techniques. In cases of anterior resection, transanal end-to-end anastomosis was done. All patients with cancer were presented, followed, and treated in the Oncology Department.
All patients were followed in the outpatient clinic every 3 months during the first 2 years after surgery.
Statistics
Data were coded and stored using Microsoft Office Excel program, and analyzed with SPSS 23.0 (SPSS, Chicago, IL). Data are reported as mean ± standard deviation. We analyzed data using descriptive and analytical statistics: independent samples t-test and χ2. The comparison of groups was conducted using Pearson's chi-squared for categorical variables and Fisher's exact test for dichotomous variables when applicable. Comparison of quantitative variables was done using parametric (e.g., t-test) and a-parametric (e.g., Mann–Whitney) tests. Differences were considered statistically significant at P < .05.
Results
Patients' demographic and surgery characteristics are presented in Table 1.
CML, conventional multiport laparoscopy; SD, standard deviation; SILS, single-incision laparoscopic surgery.
Sixty-one patients (33 male and 28 female) with mean age of 67.4 years underwent laparoscopic colonic resections: 28 SILS and 33 CML. Twenty-three patients (37.7%) had previous abdominal surgeries and 3 of them had colonic resections. There were 19 (31.2%) right, 9 (14.7%) left, and 2 (3.3%) total colectomies; 16 (26.2%) sigmoidectomies; and 13 (21.3%) anterior and 2 (3.3%) abdominoperineal resections. Colonic malignancy was a main indication for the surgery in 51 patients (83.6%). Other pathology was presented by 4 colonic adenomas (6.6%), 3 patients with diverticular disease (4.9%), 1 stromal tumor, 1 sigmoid volvulus, and 1 torsion of omentum (each representing 1.7% of cases).
Five (55.5%) out of 9 patients underwent neoadjuvant chemoradiation for rectal cancer.
The mean operation time and postoperative stay were 92.0 (range 41–251) minutes and 9 (range 4–49) days, respectively.
Pathological examination revealed stage I colon cancer in 16 (32%), stage II in 22 (44%), stage III in 10 (20%), and stage IV in 2 (4%) patients (Table 2). The mean number of retrieved lymph nodes was 19 ± 13.5. One patient with liver metastasis underwent simultaneous liver resection. Another patient with metastatic disease underwent palliative resection due to significant bleeding.
CML, conventional multiport laparoscopy; SD, standard deviation; SILS, single-incision laparoscopic surgery.
There were no differences between groups in demographic data, type of surgery, surgery time and hospital stay, and pathological results and tumor staging.
In the SILS group, additional placement of trocars was required in 6 cases: anterior resection (4), total colectomy (1), and right colectomy (1). One trocar was added in each case. The main reason for using additional trocars was for better angulation and firing of stapler insertion, and retraction to improve the view and dissection. In the SILS group, conversion was needed in 3 (10.7%) cases: 1 to multiport laparoscopy due to rupture of the SILS system and 2 to a laparotomy due to severe adhesions and inability to advance in laparoscopic mode. In the CML group, 1 (3%) operation was converted to a laparotomy due to severe pelvic adhesions from previous colectomies and an inability to advance with the operation.
Overall morbidity rate was 16.4% (Table 3). According to Clavien-Dindo classification, there were 6 (9.8%) types I–II complication, namely surgical site infections (2), urinary retention, surgical wound dehiscence, intra-abdominal bleeding that did not require surgical intervention, and deep vein thrombosis; and 4 (6.6%) types III–IV complications namely small bowel obstructions (3), ischemia, and leakage of stoma and bowel necrosis, all requiring surgical interventions. There was no statistical difference between the groups. However, the complications in the SILS group were more severe and required surgical intervention. There was no wound complications observed in the SILS group. There were no deaths or anastomotic leaks reported in both groups.
CML, conventional multiport laparoscopy; DVT, deep vein thrombosis; PC, packed cells; SBO, small bowel obstruction; SILS, single-incision laparoscopic surgery; SSI, surgical site infection.
The mean postoperative follow-up was 24.9 (range 0–36) months in the CML group and 12.9 (range 1–34) months, which was statistically different (P = .00) and can be attributed to later utilization of the novel SILS technique.
Late complications in the CML group included pouchitis after total abdominal colectomy due to familial adenomatous polyposis, temporary anal incontinence after low anterior resection that resolved after 5 months, and a perineal fistula that closed spontaneously after abdominoperineal resection. During the follow-up, an incisional hernia was found on physical examination 9 months after surgery in 2 patients (1 in each group) and was repaired laparoscopically.
During the study period, 3 patients from the CML group had cancer recurrence (2 anastomotic and 1 splenic metastases). A second primary tumor was found significantly more often in the SILS group (4 patients, P = .03). Overall, there were 51 cancers found (1 case, thought to be adenocarcinoma of the cecum, turned out to be adenocarcinoma of Müllerian origin).
Disease-free and overall survivals were similar, without statistical differences (Figs. 1 and 2).

Kaplan-Meier disease-free survival curve.
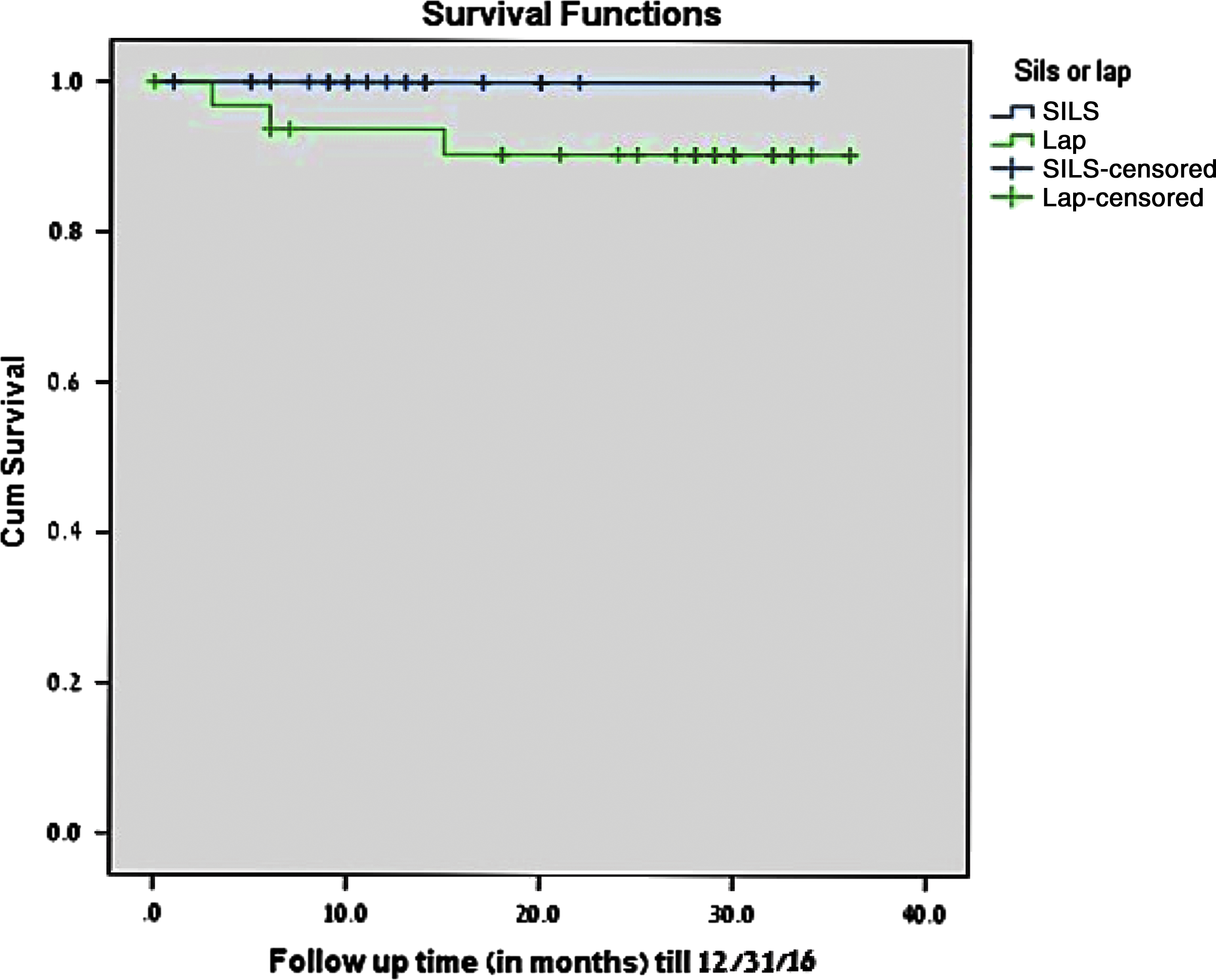
Kaplan-Meier overall survival curve.
Discussion
SILS is a relatively new approach for treating colorectal disease. Data are beginning to accumulate regarding its safety, feasibility, and short- and long-term results. Its safety and feasibility were tested and compared with CML in several case studies and case series, and it was shown and proven comparable with the added benefit of improved cosmesis. Our study did not differ in this regard and reinforced other published data.12–15 We did not find differences with regard to the surgery itself, namely, operative time, complications during the operation, conversion rate and lengths of hospital stay after the operation, postoperative complications, and number of lymph nodes harvested.
Furthermore, we did not find statistical differences with regard to oncological results as well, as shown in Table 2, and this is in accordance with other studies.9,14,16–19 The only parameter that had a statistical difference was the second primary tumor, but that is not dependent on the type of surgery, probably occurred by chance and perhaps reflects on the nonrandomized nature of our study and one of its limitations.
Studies20,21 have raised concerns regarding port site and umbilical hernias due to the site of the incision and its lengths. Some22,23 found an increased rate of port site hernia in comparison to CML, whereas others24,25 found no such difference. We did not find a difference with respect to this complication, as there was only 1 patient, in the SILS group, who developed it. Other postoperative complications were similar in both groups and were not related to SILS technique and using single port.
Conventional laparoscopy gave us a new term: triangulation, without which it would be difficult to operate, and thus conventional laparoscopic surgeries are designed to maintain it. 26 When using SILS, this triangulation is lost and, therefore, new laparoscopic tools, with a curved end, had to be created to preserve it. These instruments are expensive, and can be used mostly during SILS procedures. In our hospital we used conventional laparoscopic instruments. As shown above, the results were similar in both methods using the conventional tools. Other studies27–30 had also shown similar results with the use of conventional laparoscopic instruments in different types of operations. In our opinion, using the GelPOINT device allows good outside triangulation with enough working space inside the abdomen, compared with other single ports. The wide basis of GelPOINT helps in using conventional laparoscopic instruments. Placement of four trocars 5–12 mm through the gel basis can be used safely for changing places of working instruments and camera.
Due to limited access to the pelvis from the umbilical incision during low anterior resection, we have added an additional 12 mm trocar in the right lower abdomen for endostapler insertion during the operation. This place was used as a site for postoperative drainage insertion with good results, which is comparable to CML, and, therefore, we are validating other reports of such technique.31–33
SILS was used for other benign colorectal pathologies, including sigmoid volvulus and sigmoid diverticulosis. All of them were successful without any early or late complications. These data are comparable to other reports of benign diseases being treated by SILS with success.34,35
Data regarding the conversion rate from SILS to CML are lacking, with some authors36,37 having no conversion at all and others8,38,39 having a rate of 4%–5%. The reasons for conversion in these studies varied, for example, morbid obesity that causes excessive visceral fat, and positive air leak insufflation test following sigmoid colectomy, whereas others did not give a reason for the conversion. In our study, 1 (3.5%) operation converted to CML, and the reason for this conversion was technical, that is, rupture of the SILS system. However, whatever the reason might be for conversion, we consider it an advantage of SILS that in the case of inability to continue in this manner, a conversion to CML is easy and feasible without additional complications. The same is true for the conversion to an open surgery.
The limitations of our study include small sample size, short follow-up, and lack of randomization.
Conclusions
SILS is a feasible and safe technique comparable to CML in terms of surgical and oncological outcomes. Prospective randomized studies, including larger series with longer follow-up are needed to determine advantages of SILS technique.
Footnotes
Disclosure Statement
No competing financial interests exist.