
Abstract
Abstract
Background:
Laparoscopic appendectomy is a training model for surgical residents to begin their surgical experience. However, there is concern about worse outcomes of surgery performed by inexperienced residents. We investigated surgical outcomes and patient safety in laparoscopic appendectomy performed by residents.
Materials and Methods:
This is a retrospective cohort study of all consecutive patients operated on for acute appendicitis in a single tertiary hospital. A total of 971 patients who had laparoscopic appendectomy on an emergency basis between December 2010 and 2014 were analyzed. An attending, fellow, or resident with or without supervision performed the surgery. Surgical outcomes were compared among the four groups according to operator type.
Results:
Laparoscopic appendectomy was successfully performed in 965 patients (99.4%) and was converted to open surgery in 6 patients. The conversion rate and incidence of complications were not different among the four groups. Operating time and length of hospital stay were significantly shorter in the attending group than in the fellow or resident groups, but did not differ between the fellow and resident groups. Unsupervised residents or fellows more often placed abdominal drainage than attending surgeons. Patients with drainage had a significantly longer hospital stay compared to patients without drainage (3.64 days versus 6.33 days, P ≤ .0001), as well as a longer mean time to gas passage (1.17 days versus 1.61 days, P ≤ .0001).
Conclusions:
Resident-performed laparoscopic appendectomy was safe, but was associated with significant prolongations in hospital stay and operation time. These differences were not clinically relevant with regard to complications.
Introduction
B
Appendectomy is a basic and ideal abdominal surgery for residents to perform as the operating surgeon. Laparoscopic appendectomy is now the preferred option for appendicitis and has a better outcome than open surgery.1,2 In other words, open appendectomy is not performed without a specific indication. However, laparoscopic appendectomy is associated with increased risk of intra-abdominal abscess and longer operating time compared to the open approach. 2 Although there are conflicting results, participation of residents in the surgery may affect outcomes in open or laparoscopic appendectomy.3–5 Most studies relating to this concern were limited to only open appendectomy or the selected laparoscopic approach for uncomplicated appendicitis. It is difficult to interpret data because there were differences among studies in the resident role as an assistant or as the primary surgeon.
Therefore, the purpose of this retrospective cohort study was to compare surgical outcomes in all consecutive patients who underwent laparoscopic appendectomy by a resident with or without supervision, a fellow, or an attending.
Materials and Methods
Patients and data collection
This study was performed in a single tertiary university hospital in Korea. The protocol was approved by the local institutional review board. Electronic medical records were searched for all consecutive patients undergoing appendectomy from December 2010 to 2014. Patients undergoing appendectomy for reasons other than acute appendicitis were excluded.
Our department's policy on appendicitis is to perform a laparoscopic appendectomy first unless there are absolute contraindications. Appendectomies were performed by an attending surgeon, a fellow, or a supervised or unsupervised resident. Nine attendings, four fellows, and eight residents participated in this study. The definition of an unsupervised resident is a resident operating as the primary surgeon without supervision. Operations were performed by a third or fourth year resident when the attending on call allowed operation without supervision according to the level of training. Operating surgeons were divided into four groups: attending, fellow, supervised resident, and unsupervised resident.
A total of 1004 patients visited the hospital because of appendicitis; of these, 971 patients underwent laparoscopic appendectomy on an emergency basis and were included in analysis. A total of 33 patients were excluded, including 31 patients who underwent an interval appendectomy for initially complicated appendicitis and 2 patients who had a diagnosis other than acute appendicitis on the pathologic report. A closed-suction drain device was used for abdominal drainage in all patients, and all drains were removed 1 day before discharge or on the day of discharge.
Outcome measures
Outcomes in this study included complications, operating time, and length of hospital stay. Complications included surgical site infection, intra-abdominal abscess, ileus, sepsis, pneumonia, renal failure, radiologic intervention, readmission, and reoperation within 30 days of operation. Analysis included any complication that had a clear relationship with the appendectomy during follow-up. All patients received an outpatient appointment at hospital discharge. This appointment was usually scheduled around 7–14 days after surgery.
Statistical analysis
Comparisons of baseline characteristics and postoperative outcomes were performed using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables. All categorical variables were compared using Fisher's exact test. Data are presented as the mean ± standard deviation. A two-sided P value of less than .05 was considered statistically significant. Multivariate logistic regression analysis was used to calculate the odds ratio of overall complications. A multivariate regression model was used to analyze the impact of abdominal drainage on postoperative outcomes after adjusting for age, sex, American Society of Anesthesiologists (ASA) classification, operator, and pathology. Statistical analysis was performed by IBM SPSS statistical software (version 23; IBM Corporation, Armonk, NY).
Results
During the study period, a total of 971 patients underwent laparoscopic appendectomy and were included in the analysis. Table 1 shows baseline patient characteristics. The four groups were comparable in age, sex, ASA classification, and type of operation, and they only differed in pathology. The attending group included more patients with suppurative appendicitis. Four patients underwent ileocecal resection and 1 patient underwent right hemicolectomy.
ASA, American Society of Anesthesiologists.
Laparoscopic appendectomies were successfully performed in 965 patients (99.4%) and were converted to open surgeries in 6 patients (Table 2). No patients died. There were no significant differences in Clavien-Dindo grade or overall complications among the four groups. However, operating time, abdominal drainage, postoperative hospital stay, and length of hospital stay differed between the groups. The attending group had significantly shorter operation time and placed fewer abdominal drains than other groups. The length of hospital stay was shorter in the attending group than in the other groups. There were no differences in hospital stay or drainage between the other three groups (Fig. 1).
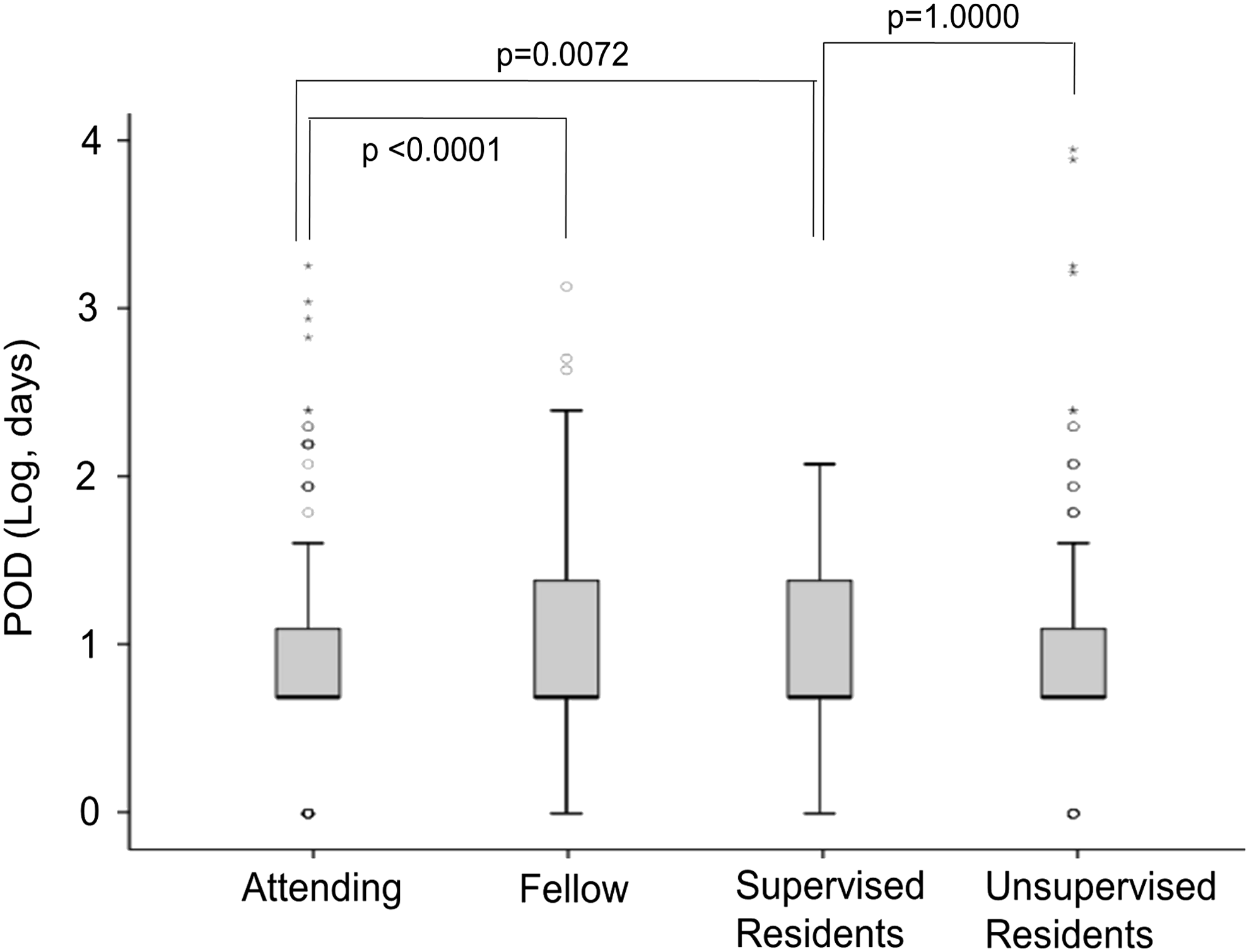
The difference of postoperative hospital stay. The length of hospital stay was significantly shorter in attending group. There were no differences of postoperative stay between three groups other than attending. POD, postoperative stay.
The odds ratios for overall complications are presented in Table 3. A gangrenous or perforated pathology and operation time were associated with increased risk of overall complications in the univariate model, but not in the multivariate model. The risk of overall complications did not vary significantly among operator groups.
ASA, American Society of Anesthesiologists; CI, confidence interval; OR, odds ratio; ref., reference.
When patients were divided according to the presence or absence of drainage (Table 4), patients with abdominal drainage had a significantly longer hospital stay compared to those without drainage (3.64 versus 6.33, P ≤ .0001). As shown in Table 1, the attending group inserted fewer abdominal drains. When patients were divided according to the severity of inflammation, there was no difference in drain insertion for complicated appendicitis. However, unsupervised residents or fellows placed abdominal drainage more frequently for suppurative appendicitis than attending surgeons. Mean time to gas passage was shorter in the group without drainage (1.17 days versus 1.61 days, P ≤ .0001). The effect of abdominal drainage on postoperative outcomes was assessed using a multivariate regression model (Table 5). Patients with abdominal drainage had significantly longer hospital stay (1.98 and 2.02 days, postoperative and total, respectively) and operation time (23.62 minutes), as well as delayed gas passage (0.34 days) after adjusting for age, sex, ASA class, operator, and pathology.
Adjusted for age, gender, ASA class, operator, and pathology.
ASA, American Society of Anesthesiologists; PE, parameter estimate; SE, standard error.
Discussion
Minimally invasive surgery is widely known by both doctors and patients. Most patients with appendicitis or other colorectal diseases often confirm before surgery if laparoscopy is available. Laparoscopy is an essential course for resident education and training and is a basic skill for the present generation of young surgeons. Surgical residents begin their laparoscopic experience with camera holding to become familiar with surgical anatomy while watching a monitor in the field of laparoscopic view. They start their role as a primary operating surgeon with basic laparoscopic procedures such as appendectomy, cholecystectomy, and inguinal hernia repair.
Laparoscopic appendectomy has shown several clinical benefits and superior outcomes to open appendectomy.6–9 It has been recognized as a preferred option in patients with uncomplicated or complicated appendicitis across all severities of illness categories. 10 Surgery for appendicitis results in a variety of surgical outcomes depending on the severity of inflammation, appendix location, and surgeon experience. It is not necessarily an easy operation.
Currently, almost all patients with suspected acute appendicitis undergo computed tomography or ultrasonography before surgery. The diagnostic accuracy of these imaging modalities has greatly improved, and the likelihood of negative appendectomy has greatly decreased. Complicated situations and the severity of inflammation can be previewed in detail before surgery. The treatment policy has also changed. For appendiceal abscess or phlegmon, which would previously require extended surgery, it is now recommended to perform nonsurgical treatment rather than immediate surgery. 11 Thus, it is possible for residents to perform laparoscopic appendectomy for properly selected patients. With laparoscopic experience, they can be challenged with even more complex procedures.
In our study, surgery performed by residents did not result in more complications or mortality than surgery performed by attending surgeons. The low morbidity rates for the resident group indicate that resident-performed laparoscopic appendectomy is safe and feasible for appropriately selected patients. In almost all outcomes except operating time and length of stay, residents showed comparable results to those of attendings or fellows.
In terms of the operating time, there was no difference between fellows and residents with or without supervision. Generally, prolonged operative time is associated with increased complications in various laparoscopic surgeries.12,13 Recent studies from the American College of Surgeons National Surgical Quality Improvement Program database found that resident involvement in surgical procedures is associated with adverse postoperative outcomes, although information on level of resident involvement was not available.4,5,14,15 They showed that resident intraoperative participation is associated with longer operative times and higher morbidity rates, but lower mortality rates. However, the authors also mentioned that resident participation is safe14,15 and that surgeons should provide appropriate supervision as needed to minimize operation time. 4 In the present study, differences in operation time and hospital stay were statistically significant, but not clinically relevant to adverse postoperative outcomes. We presume that there were no differences in complications because operation times were relatively short overall and differences were small.
In our study, length of hospitalization and postoperative stay were 4.36 and 3.18 days, respectively. These values were similar or slightly longer than western results.10,16 This likely reflects the special situation of Korean medical insurance. Other large Korean studies on laparoscopic appendectomy showed no difference in postoperative hospital stay. 17 Subgroup and multivariate analysis suggested that longer hospital stay was associated with drain insertion. Drains were more frequently placed by residents or fellows than by attending surgeons, even for suppurative appendicitis. Bowel recovery times were prolonged in patients with abdominal drainage. Due to limited experience, residents may not be sure whether they placed abdominal drainage or not, even if the surgery was performed well. Direct contact between the drainage tube and bowels could impair bowel activity. 18 However, intra-abdominal conditions requiring drainage seem to be more pertinent to delayed bowel recovery than the drainage tube itself. Even with suppurative appendicitis, drains are often placed for more inflamed bowels, which may require a longer time to recover. Moreover, most patients with drains wanted to be hospitalized as long as it was in place.
In our department, abdominal drainage after appendectomy is a common practice in complicated appendicitis although there are doubts as to whether this practice has clinical benefits.18,19 Drainage of infected areas is believed to prevent postoperative intra-abdominal abscess by evacuating infected fluids and subsequently reducing radiologic intervention. If there is significant purulent ascites or infected debris even though the appendix is not perforated, it is our policy to insert a drain tube. Our department custom emphasizes safety and could have influenced resident choices. Drain insertion and timing of its removal are largely dependent on a surgeon's preference and experience. Based on the results of this study, our policy on drain tube insertion should be improved to shorten length of hospital stay.
There are several limitations in our study. First, this study is observational and retrospective in design. Each group of operators included surgeons with a variable degree of experience. There was a significant difference in pathological findings between the four groups, reflecting the severity of inflammation. The attending group included more patients with suppurative appendicitis. Although more patients with complicated appendicitis were operated on by unsupervised attendings or fellows, surgery by residents resulted in comparable outcomes. Thus, laparoscopic appendectomy performed by residents is safe. Second, this study was conducted in a single tertiary teaching hospital. During the study period, there was no planned open appendectomy in our hospital. Individual teaching hospitals may have different training systems and surgical practices for appendectomy. The resident training system in a single tertiary teaching hospital may not be representative of the general hospital.
In conclusion, we observed that laparoscopic appendectomy performed by residents is safe regardless of supervision and did not adversely affect most outcomes. Laparoscopic appendectomy performed by residents resulted in prolonged hospital stay and longer operation time. These differences were statistically significant, but not clinically relevant to complications. Abdominal drainage was associated with a longer hospital stay and delayed bowel recovery and should be carefully considered.
Footnotes
Acknowledgment
This work was supported by a grant from Kyung Hee University in 2014 (KHU-20140706).
Disclosure Statement
No competing financial interests exist.