
Abstract
Abstract
Background:
Risk factors for staple line bleeding (SLB) during and after sleeve gastrectomy (SG) are various, including patient related factors, perioperative medications, and surgical technique, although there is little clarification in the literature of the role played by blood pressure during the stapling phase. The aim of the present retrospective cohort study was to identify possible risk factors liable to cause SLB.
Materials and Methods:
Data collected prospectively from 120 consecutive patients who underwent SG were analyzed retrospectively according to age, gender, body mass index (BMI), international normalized ratio (INR) value, intraoperative systolic blood pressure (SBP), and mean arterial blood pressure (MABP).
Results:
In univariate analysis, age, stapling phase SBP and MABP, and the duration of surgery were all significantly higher in patients with SLB than those without (P < .05). In distinguishing patients with SLB from those without, the cutoff threshold for SBP during the stapling phase was 120 mmHg with a 78.9% sensitivity, 97.6% specificity, 93.8% positive predictive value, 90.9% negative predictive value, and 91.7% accuracy (AUC = 0.908, 95% CI: 0.839–0.976, and P < .001). In multivariate logistic regression analysis, independent of age and operation time, SBP >120 mmHg significantly maintained its predictive power on SLB (95% CI: 32.410–1457.896, P < .001).
Conclusion:
A SBP >120 mmHg during the division of the stomach is an independent risk factor for SLB. Maintaining intraoperative SBP ≤120 mmHg during the stapling phase does not only decrease the risk of SLB but also the need for homeostatic agents such as clips and sutures, which in turn prolong the operative time and increase cost.
Introduction
M
Reasons to prefer SG over other bariatric procedures are its easier technique which requires no anastomosis; avoidance of complications associated with malabsorptive operations such as dumping syndrome and diarrhea; less need for trace elements and vitamin supplements; and no risk of marginal ulcers or internal hernias. SG achieves a weight loss effect within the range between Gastric Banding and Laparoscopic Roux-en-Y Gastric Bypass (LRYGB).9–12 Furthermore, leakage and mortality rates after SG are comparable with LRYGB. 13
While bariatric surgeons usually focus on postoperative leaking (1%–2%) after SG, the risk of hemorrhage still remains high, ranging from 1% to 3%.14,15 Bleeding usually occurs from the dissection of the greater curve of the stomach or the staple line. Many different methods have been tried to stop staple line bleeding (SLB), including using oversewing sutures, buttressing material, and tissue fibrin sealant.16–18 However, there is no consensus in the literature as to the superiority of one option over the other.15,19–21
The aim of the present retrospective cohort study was to evaluate the possible risk factors for intraoperative SLB such as age, gender, body mass index (BMI), international normalized ratio (INR) value, systolic blood pressure (SBP), and mean arterial blood pressure (MABP).
Materials and Methods
Following approval by the Institutional Ethics Board Committee of Sakarya University, data collected prospectively from 120 consecutive morbidly obese patients who underwent SG between October 2015 and February 2017 in Sakarya University Teaching and Research Hospital were retrospectively analyzed. All operations were performed by a single surgeon. Information about patient characteristics and demographic data, including age, gender, BMI, comorbid diseases (hypertension [HT], diabetes mellitus type II, chronic obstructive lung disease), postoperative morbidity (postoperative leakage, postoperative hemorrhage), and mortality, was extracted from the patient folders. Patients with intraoperative SLB requiring hemostatic clips during the stapling phase were compared with those with no SLB according to age, gender, BMI, INR value, stapling phase SBP, and MABP. SBP and MABP were measured at the beginning of the surgery just after the anesthesia induction, during the stapling phase and at the end of the surgery just before recovery. MABP was calculated using the formula MAP = [(2 × diastolic blood pressure) + systolic blood pressure]/3.
General anesthesia protocol
Premedication of intravenous (i.v.) midazolam (0.2 mg/kg) was administered. Then, anesthesia induction was started using fentanyl (1 μg/kg), lidocaine (1 mg/kg), propofol (2 mg/kg), and rocuronium (0.8 mg/kg). Following endotracheal intubation, mechanical ventilation was continued with 50% mixed oxygen and adjusted to maintain the end-tidal CO2 (ETCO2) between 35 and 40 mmHg. The anesthesia was maintained with sevoflurane (2%) and remifentanil (0.05–0.5 μg/kg/min infusion). Hemodynamic parameters were measured every 5 minutes. Arterial HT was regulated by remifentanil dosage adjustment and addition of nitroglycerin, when necessary. In the case of hypotension, ephedrine was given, and the depth of anesthesia was controlled by the dose adjustment of remifentanil. Reversal of the neuromuscular blockage during the extubation period was assessed with bridion, and postoperative pain was relieved using contramal (1 mg/kg).
SG procedure
After anesthesia induction, CO2 pneumoperitoneum was established with a Veress needle and maintained at a pressure of 12 mmHg. A 30° viewing laparoscopic camera was introduced through a 10 mm port which was inserted on the superior-lateral left side ∼10 cm away from the umbilicus. A 15 mm port was then inserted 10 cm lateral to the right and 2 cm above the camera port. A liver retractor was inserted through a 5 mm trocar localized in the right midclavicular line, 5 cm inferior to the costal margin. Two 5 mm trocars were placed through the left midclavicular and anterior axillary lines (Fig. 3). The gastrocolic ligament was opened adjacent to the stomach at a distance of 6 cm from the pylorus. The greater omentum was carefully dissected from the stomach using 5-mm abdominal LigaSure (LigaSure®; Medtronic-Covidien, Minneapolis), along the line of the greater curvature, from the antrum toward the angle of His. Short gastric arteries and veins were coagulated near the spleen. The angle of His was protected, and the left diaphragmatic crus was revealed. A 36-French orogastric tube was inserted orally into the stomach following the curvature minor. The stomach was then divided parallel to the orogastric tube along the curvature minor using a laparoscopic linear stapler (Endo GIA® Covidien-Medtronic, Minneapolis), which was inserted through the 15 mm trocar. SG was completed after this gastric resection, using 4.8 mm staple height (green) for the first two stapler cartridges and 3.5 mm staple height (blue) for the rest. In the presence of an active continuous bleeding at the staple line, which cannot be stopped spontaneously, homeostatic metallic clips are used for hemostasis rather than oversewing for reinforcement. At the end of the staple line dissection, a surgical sponge was laid out along the staple line through the 10 mm trocar. Methylene blue was added through the orogastric tube for a leakage test; when the surgical sponge was removed from the abdominal cavity, it was checked for methylene blue staining. If no leak was seen, fibrin sealant Tisseel® (Baxter, Deerfield, IL) was sprayed along the staple line of the remaining stomach. The staple line was covered with the greater omentum, when possible. The resected stomach was extracted from the peritoneal cavity through the 15 mm trocar hole, and a drain was inserted through the left-sided 5 mm trocar. The trocars were then removed from the abdominal cavity under direct visualization after hemostasis was achieved. The aponeurosis was secured with 1/0 polyglactin 910 at port-sites with a diameter greater than 5 mm, and the skin was closed with 3/0 polypropylene single matrix sutures.
Standard protocol for postoperative follow-up
After the operation, patients were followed up in the General Surgery Clinic unless the intensive care unit (ICU) was required. An intravenous fluid replacement and anticoagulant prophylaxis with Enoxaparin-natrium (Oksapar® 0.6 iu/L, subcutaneous; Kocak, Istanbul, Turkey) were started. On the second postoperative day, methylene blue was administered orally to retest for leakage. If the drain was not stained with methylene blue, this suggested that there was no leak and a liquid diet was started. The patient was discharged on the fourth postoperative day, after checking for pleural effusion with a chest X-ray, and that patient's blood tests, including C-reactive protein, were at normal levels. If a fall in blood hematocrit levels or the external drain indicated bleeding >50 mL/hour, anticoagulant medication was stopped and blood loss was replaced with fresh frozen plasma and erythrocyte suspension when patient's hemoglobin (Hb) <9 gr/dL or a fall in Hb level more than 2 gr/dL within 24 hours. In the case of leakage, the preferred approach was to discontinue oral consumption and place an endoscopic stent. The patient's external drain was removed on discharge and patients had routine checkups throughout the first year at 3-month intervals.
Statistical analysis
The Kolmogorov–Smirnov test was used to determine normality in the distribution of continuous variables. Data are shown as mean ± standard deviation or median (minimum-maximum) for continuous variables. For categorical data, the number of cases and percentages were used. While the mean differences between patients with and without stapler bleeding were compared using Student's t-test, Mann–Whitney U test was applied for other comparisons of non-normally distributed variables. Categorical data were analyzed by Continuity Corrected Chi-square test. The optimal cutoff points for intra-op blood pressures (i.e., systolic, diastolic, and mean) to determine stapler bleeding were evaluated by receiver operating characteristics (ROC) analyses, calculating the area under the curve to give the maximum sum of sensitivity and specificity. Multiple logistic regression analysis was used to evaluate whether the effects of intra-op blood pressures were still valid after adjustment for all possible risk factors. Any variable whose univariable test had a P value <.10 was accepted as a candidate for the multivariable model, along with all variables of known clinical importance. Odds ratios, 95% confidence intervals, and wald statistics for each independent variable were also calculated. Data analysis was performed using IBM SPSS Statistics version 17.0 software (IBM Corporation, Armonk, NY). A P value less than .05 was considered statistically significant.
Results
Between October 2015 and February 2017, 120 consecutive morbidly obese patients underwent SG in Sakarya University Teaching and Research Hospital. Of these, 99 patients were female (82.5%) and 21 patients were male (17.5%). The mean BMI was 46.3 ± 4.6. Thirty-two patients (26.7%) had diabetes mellitus and/or impaired fasting glucose; 24 patients (20%) had HT; 5 patients (4.2%) had coronary artery disease (CAD); 2 patients (1.7%) had chronic obstructive pulmonary disease (COPD); and 1 patient (0.8%) had situs inversus totalis. The median INR value was 0.96 (min-max; 0.75–2.60). The median time interval from intubation to extubation was 100 min (min-max; 60–190), and duration of the surgery was 90 min (min-max; 50–180). SLB during the stapling phase occurred in 38 patients (31.7%). In all cases of SLB, hemostasis was achieved using only metallic clips. Of the 32 patients with diabetes mellitus and/or impaired fasting glucose, 11 patients had SLB and all of them had SBP over 120 mmHg during the stapling phase. One patient needed conversion to open surgery due to bowel injury during the 10 mm trocar insertion, and the SG was completed after primary repair of the perforated transverse colon. Three patients (2.5%) had postoperative hemorrhage, indicated by drain content and a fall in hematocrit levels. However, bleeding did not lead to hemodynamic instability and stopped spontaneously after a few days of conservative management with erythrocyte replacement. These three patients also had SLB during the operation where metallic clips were again used for homeostasis. None of the patients developed a gastric leak (Table 1).
Time interval from intubation to extubation.
These three patients also had SLB during the operation.
ASA, American Society of Anesthesiologists; BMI, body mass index, HT, hypertension; DM, diabetes mellitus; IFG, impaired fasting glucose; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; INR, international normalized ratio; SLB, staple line bleeding.
Descriptive statistics of SBP and MABP measured at the beginning of the surgery, during the stapling phase, and at the end of the surgery just before recovery is listed in Table 2. The mean age, intraoperative SBP, MABP, and the duration of the surgery were significantly higher in patients with SLB than those without (P < .05), (Fig. 1). However, although still within normal ranges, median INR values were significantly less in patients who developed SLB, compared to those who did not (P = .038). In contrast, no significant difference was found between the two groups regarding gender, ASA score, or preoperative BMI (P > .05) (Table 3).
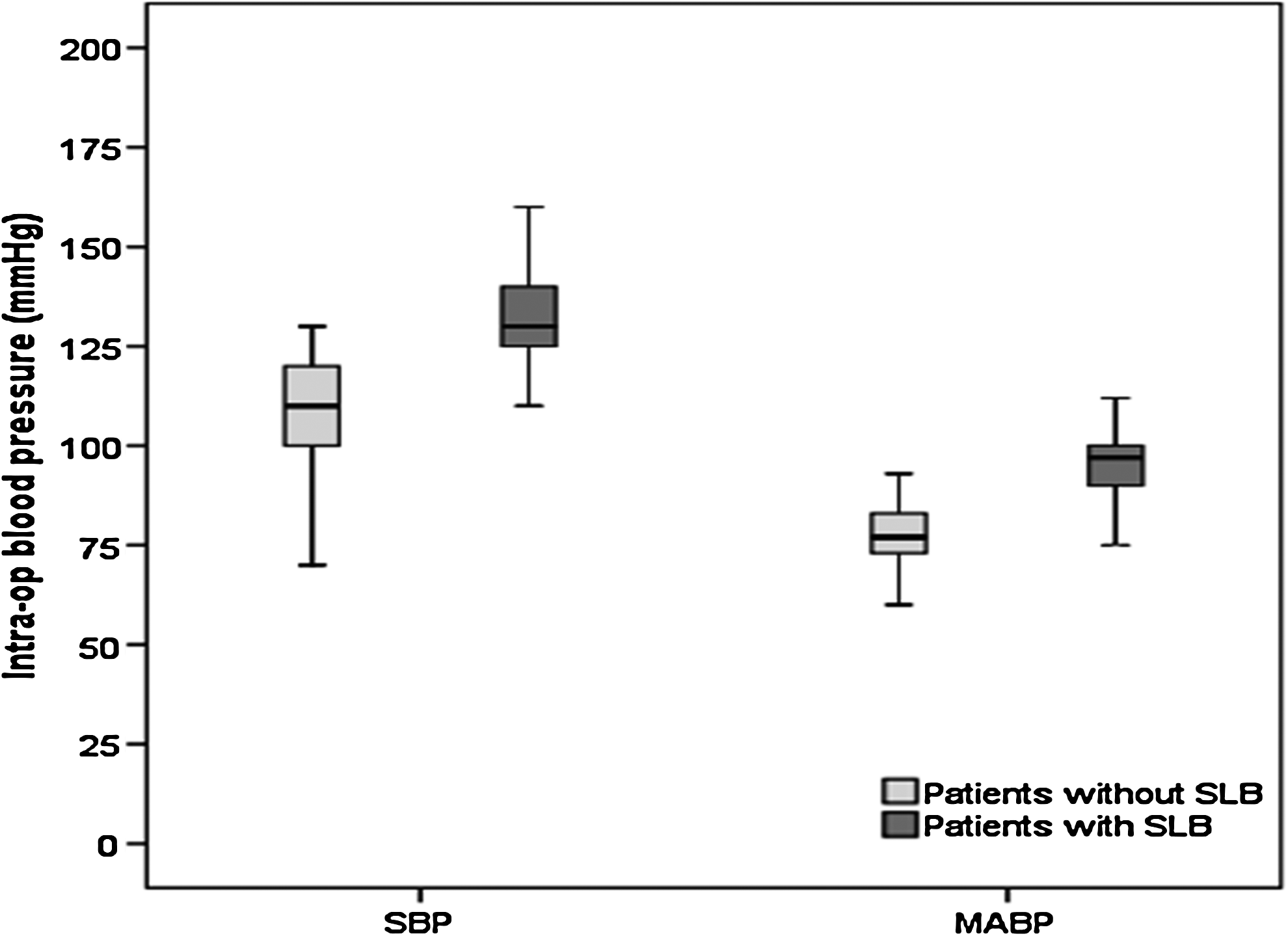
Distribution of systolic and mean arterial blood pressures in patients with and without staple line bleeding.
SD, standard deviation; min, minimum; max, maximum; SBP, systolic blood pressure; MABP, mean arterial blood pressure.
Student's t-test.
Continuity corrected Chi-square test.
Mann–Whitney U test.
Bold values are statistically significant.
BP, blood pressure.
ROC analysis for intraoperative blood pressure measurements revealed that the undercurve area was significant in distinguishing patients with SLB from those without. The cutoff threshold for this distinction was 120 mmHg with a 78.9% sensitivity, 97.6% specificity, 93.8% positive predictive value (PPV), 90.9% negative predictive value (NPV), and 91.7% accuracy (AUC = 0.908, 95% CI: 0.839–0.976, and P < .001). The cutoff threshold for MABP to differentiate SLB patients was 87.5 mmHg with 78.9% sensitivity, 89.0% specificity, 76.9% PPV, 90.1% NPV, and 85.8% accuracy (AUC = 0.901, 95% CI: 0.835–0.967, and P < .001), (Table 4 and Fig. 2).

ROC curve showing the predictive value of systolic and mean arterial blood pressures for staple line bleeding. ROC, receiver operating characteristics.
Bold values are statistically significant.
AUC, area under the curve; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value.
In multivariate logistic regression analysis, after correction for age, INR value, and duration of surgery, MABP >87.5 mmHg was seen to maintain its predictive power for SLB (95% CI: 15.123–271.297, P < .001). In addition, age (OR = 1.068, 95% CI: 1.010–1.129, P = .022) and duration of surgery (OR = 1.031, 95% CI: 1.007–1.055, P = .010) both had a significant effect on SLB. Independent from other variables (age, INR value, and duration of surgery), SBP >120 mmHg significantly maintained its predictive power for SLB (95% CI: 32.410–1457.896, P < .001), (Table 5 and Fig. 3).

Distribution of the patients with staple line bleeding over and under 120 mmHg systolic blood pressure.
Bold values are statistically significant.
OR, odds ratio.
Discussion
Hemorrhage during or after SG is a rare complication, which can sometimes be problematic in that it may trigger a series of events such as hematoma, followed by abscess formation, which will require percutaneous drainage or reoperation. Furthermore, an infected hematoma around the staple line has the potential risk to develop leaks.22,23
Risk factors for bleeding are various, including patient-related factors, perioperative medications, and surgical technique. Medical conditions that are more prone to per-operative bleeding are renal failure, nonalcoholic fatty liver, HT, smoke and alcohol consumption, super obesity, and coagulopathy. Drugs and supplements associated with increased surgical bleeding are nonsteroidal anti-inflammatory drugs, warfarin, clopidogrel, glucophage, ketorolac, and Ginkgo biloba.23–26 Risk factors related to surgical technique are the use of inadequate cartridge height for different parts of the stomach; unnecessary dissection around the cardioesophageal region, particularly around the Angle of His and phrenoesophageal ligaments; and excessive division of the distal stomach from the omentum where a point of ∼2 cm proximity to the pylorus is reached or passed. In addition, previous abdominal and gastric surgery may increase the complexity of surgery, due to adhesions that can increase the risk of bleeding.22,23,26,27
Bleeding from the staple line during and after SG represents the most frequent complication at a rate of up to 9.3% (mean rate 3.6%). 28 Previous studies have shown that use of staple line reinforcement, while playing no significant role in preventing gastric leak, seems to reduce SLB.20,29 However, it does bring an additional financial burden. Likewise, oversewing sutures can be used for the same purpose. However, in our own clinic we use neither staple line reinforcement nor oversewing sutures. Our reasoning in this study is that SG involves the longest gastric staple line of any procedure and is closest to the lesser curvature blood supply; oversewing sutures may further interrupt or diminish the blood supply at the staple line, leading to ischemia with a high probability of subsequent necrosis and leakage. Therefore, in cases of SLB we only use homeostatic metallic clips on the hemorrhaging points of the staple line, as required. Results of the present study demonstrate that the use of adequately sized cartridges and the application of fibrin sealant seem to be sufficient to achieve homeostasis when blood pressure during the stapling phase is below a certain level.
HT is usually an integral part of obesity-related diseases. One of the primary goals of bariatric surgery is to correct HT in morbidly obese patients. However, some morbidly obese patients present with intractable malignant HT and it requires serious effort to regulate their blood pressure before surgery, during anesthesia induction, and even during the surgery itself. As well as this, the stomach is an organ rich in blood supply, with a numerous and intense capillary collateral network. The thickness of the gastric wall is greatest at the distal part of the stomach and gradually decreases toward the fundus. Consequently, use of an adequate height of stapler cartridge is very important, not only for an ideal B formation at the staple line but also for homeostasis. According to recommendations, we always start dividing the stomach from the antrum, in a row, with two green cartridges, then follow with blue cartridges.23,26,27
Homeostasis at the staple line depends on the occlusion of vessels coupled with adequate clot formation. Technical faults with staplers, improper firing, disparity between cartridge size and tissue thickness, or patient related factors such as abnormal clotting can all lead to SLB. The presence of HT during the division of the stomach with stapler devices carries the potential risk of preventing clot formation at the surface of the staple line, particularly in weak capillaries with poor wall muscles incapable of sufficient vasoconstriction.
Application of fibrin sealants on the staple line is another way to prevent bleeding, achieving homeostasis by increasing the intrinsic pressure over the staple line. It has been previously shown in a randomized study that use of fibrin sealants is associated with decreased postoperative hemorrhage. 18 For this purpose, we use fibrin sealants routinely. We observed over time that patients with a higher intraoperative SBP seemed to be more prone to SLB, which give us the inspiration for the study design. Results of the present study indicate that SBP >120 mmHg during the stapling phase is an independent risk factor for SLB, which then needs homeostatic clipping or suturing and, therefore, prolongs the operation time. A multidisciplinary approach with anesthetists to keep the SBP around 100–110 mmHg just before and during the division of the stomach will decrease the risk of bleeding. We recommend homeostatic clips when an active bleeding from the staple line occurs and after a while not spontaneously stops. In this case, if bleeding is accompanied by high SBP, reducing the blood pressure also may help to control bleeding and achieving hemostasis. Despite this process, if bleeding continues, oversewing sutures may be necessary.
Another precious detection of the present study was that preoperative INR values of patients with SLB were in normal ranges. This result is extremely important to show the effect of blood pressure on SLB where INR related coagulation abnormalities are excluded. In addition, patients of a mature age show a tendency to bleeding at the staple line. There is not enough research on the effect of blood pressure on SLB in the literature. In the study by Sroka et al., 30 provocative elevation of the SBP to 140 mmHg was performed at the end of the surgery, similar to the Valsalva maneuver in thyroid surgery, to test for bleeding at the staple line. They hypothesized that SLB starts in the post anesthesia care unit due to a rise in blood pressure. In contrast to this claim, we did not observe any rebleeding in the postoperative period except the three patients with postoperative hemorrhage whose SBP during the division of the stomach was also over 120 mmHg. For these reasons, we consider a provocative test at the end of the surgery unnecessary and even possibly harmful, as this initiative could increase the risk of rebleeding. Another important point from our observations is that if homeostasis is achieved during the operation with clot formation at the staple line during and after the stapling phase, it should also continue through the postoperative period, despite the relative rise in blood pressure.
The present study has some limitations. First, it is of a retrospective nature. Second, the sample size is small. In contrast, this is the first study which focused during the stapling phase on the relationship between SBP and SLB.
Conclusion
In conclusion, hemorrhage still remains a major drawback of SG and a SBP >120 mmHg during the division of the stomach is an independent risk factor for SLB. Maintaining intraoperative SBP ≤120 mmHg during the stapling phase not only decreases the risk of SLB but also the need for homeostatic agents such as clips and sutures, which would in turn increase the operative time and cost.
Footnotes
Acknowledgment
This research received no specific grant from any funding agency or public, commercial, or not-for-profit sectors.
Disclosure Statement
No competing financial interests exist.