
Abstract
Abstract
Background:
Off-clamp robot-assisted partial nephrectomy (RAPN) is associated with increased intraoperative blood loss compared with on-clamp technique. Our aim was to demonstrate our surgical technique and to determine which tumors are ideally suited for this technique.
Methods:
Sixty-two patients who underwent off-clamp RAPN for renal tumor between 2006 and 2016 were retrospectively analyzed. Increased estimated blood loss (EBL) volume was defined as more than 75 percentile. receiver operating characteristic (ROC) analysis was used to determine exact cut-off tumor size and the preoperative aspects and dimensions used for an anatomical (PADUA) score that are associated with increased EBL. Risk factors for increased EBL >400 mL and chronic kidney disease (CKD) upstaging were evaluated using logistic regression analysis.
Results:
The median follow-up period was 20 months (interquartile range [IQR]: 12–84). Patient's mean age, mean tumor size, and mean body mass index were 53.5 ± 12.2 years, 2.6 ± 1.5 cm, and 25 ± 4.1 kg/m2, respectively. Median EBL volume was 200 mL (IQR: 100–400). ROC analysis showed that tumor size of 3.2 cm (area under the curve [AUC] = 0.82, P < .001) and PADUA score of 9 (AUC = 0.79, P = .001) were cut-off values for increased EBL >400 mL. Patients with tumor size >3.2 cm had longer operative time (116 versus 163 minutes, P = .002), more EBL (150 versus 575 mL, P < .001), and higher blood transfusion rate (0% versus 18.8%, P = .015), with increased tendency of conversion to radical nephrectomy (0% versus 12.5%, P = .063) compared with tumor size ≤3.2 cm. Overall CKD upstaging was present in 22 patients (35.4%). Multivariable logistic regression analysis showed that EBL >400 mL was the only predictor of CKD upstaging (odds ratio: 6.704, P = .009).
Conclusions:
Our study showed that the risk of intraoperative bleeding and transfusion rate during off-clamp RAPN is increased if tumor size >3.2 cm and/or PADUA complexity score ≥9. Moreover, EBL >400 mL was a risk factor of CKD upstaging, despite zero ischemia. Further larger prospective studies are warranted to validate our results.
Introduction
R
Before performing off-clamp RAPN, the potential risk of increased EBL during surgery, which may affect the intraoperative patient's safety and/or postoperative patient recovery, should always be kept in mind. In a recent research, off-clamp RAPN for small renal tumors was associated with higher EBL and increased risk of conversion to radical nephrectomy (RN) compared with on-clamp RAPN. 6 Increased EBL >250 mL following PN might predict the incidence of postoperative hemorrhagic complications, such as blood transfusion, decrease in hemoglobin >3 g/dL, and/or arteriovenous fistula formation. 9 Moreover, increased bleeding during PN surgery is not only associated with increased risk of perioperative complications, but also has a negative impact on the postoperative renal function.10–12
Previous off-clamp RAPN studies have recommended its application in small-sized and peripherally located renal tumors, and some surgeons have reported its feasibility even in more complex tumors. 13 However, no standardized cut-off tumor size or complexity score has yet been determined.
Thus, we aimed to describe our off-clamp RAPN surgical technique, to determine tumor size and characteristics associated with increased intraoperative bleeding, as well as, to identify predictors of chronic kidney disease (CKD) upstaging.
Patients and Methods
From September 2006 to January 2016, data of 309 patients underwent RAPN at a high-volume institution were revised and extracted from our prospectively maintained database (institutional review board number: 2014-0091-001). Sixty-two patients who received off-clamp RAPN were included in the present study. All patients were fully informed with regard to the off-clamp RAPN surgical approach and its possible complications.
Patients' clinical and demographic characteristics were extracted (age, gender, body mass index [BMI], American Society of Anesthesiologists [ASA] score, Charlson's comorbidity index [CCI] score, preoperative estimated glomerular filtration rate [eGFR], and preoperative CKD), as well as tumor characteristics (tumor size, the preoperative aspects and dimensions used for an anatomical [PADUA] score, and surgical margin status). Perioperative data (operative time [OT], EBL, length of hospital stay [LOS], blood transfusion rate, and intraoperative complications) and early postoperative complications (within 30 days according to Clavien–Dindo classification) were analyzed.
Renal function assessment was determined by regular serum eGFR measurements at 1, 3, 6, 12 months, then yearly. The stage of CKD was based on the National Kidney Foundation Kidney Disease Outcome Quality Initiative Classification. 14 CKD upstaging was defined as a change in one class of CKD or more. 15
Off-clamp RAPN surgical technique
All RAPN procedures were performed by a single-expert surgeon using da Vinci Si and Xi Surgical Systems (Intuitive Surgical, Inc., Sunnyvale, CA) through the transperitoneal approach. The choice of therapy was determined through consultation between the surgeon and the patients.
Anesthesia
General anesthesia.
Patient position
The patient is placed in the lateral flank position with no table flexion (Fig. 1), secured to the table with adhesive tape, and gel support with padding is applied to all pressure points.

Patient positioning in lateral flank position with no table flexion.
Port placement
We establish the pneumoperitoneum with a Veress needle. In patients with previous abdominal surgery, we use an open method (Hasson) to obtain the pneumoperitoneum (Fig. 2a–c). We start with pressure of 20 mmHg, and then decrease it to 15 mmHg after port docking. Port sites are different according to the da Vinci model (either Si or Xi). For da Vinci Si (Fig. 2a) we insert a midline supraumbilical 12-mm camera port, two 8-mm robotic ports in the midclavicular line at an 8–9 cm distance from the camera port, and an 8-mm robotic port at 10–12 cm from the lower robotic port directed toward the anterior superior ischial spine. A 12-mm assistant port is placed in the midline below the umbilicus and at an 8 cm distance from the lower robotic port. For right-sided renal tumors, we insert an additional 5-mm port for liver retraction. In the da Vinci Xi model, we used our modified port placement technique which is similar to Si port sites (Fig. 2b), instead of the universal linear port placement (Fig. 2c). 16

Ports placement with da Vinci Si
Robotic instruments
We use the following robotic instruments: a laparoscopic 30° downward lens, ProGrasp® forceps, Hot Shear™M Monopolar curved scissors, two large needle drivers, and Fenestrated Bipolar Forceps (Intuitive Surgical, Inc.).
Surgical steps
A detailed video illustrating step-by-step off-clamp RAPN is combined with the article (watch the supporting Supplementary Video S1; Supplementary Data are available online at www.liebertpub.com/lap).
Study outcome measurements
The primary endpoint of our research was to demonstrate our off-clamp RAPN surgical technique. The secondary endpoint was to identify the optimum tumor size and complexity which are associated with risk of increased intraoperative bleeding > 400 mL; as well as, factors associated with overall CKD upstaging.
Statistical analyses
EBL percentiles were calculated for all patients who underwent off-clamp technique and the upper quartile, that is, 75th percentile (400 mL) was chosen as the threshold for defining increased EBL. Receiver operating characteristic (ROC) curve analysis was used to identify cut-off value of tumor size and PADUA complexity score for the prediction of increased EBL. Univariable and multivariable logistic regression models were used to identify the variables which predict the increased EBL (> 400 mL) and overall CKD upstaging. We compared the 2 groups of patients (tumor size ≤3.2 and >3.2 cm) using an independent t-test or Mann–Whitney U-test for comparing continuous variables, specified as mean and standard deviation or median and interquartile range (IQR), whereas Chi-square test or Fisher's exact test were used for comparing categorical variables, specified as frequency (%). A P value of <.05 was considered statistically significant. The statistical analysis was performed using IBM SPSS version 23 statistical package (SPSS, Inc., Chicago, IL).
Results
Sixty-two patients underwent off-clamp RAPN. Their mean age, mean tumor size, mean BMI, and median follow-up period were 53.5 ± 12.2 years, 2.6 ± 1.5 cm, 25 ± 4.1 kg/m2, and 20 (12–48) months, respectively. Median EBL was 200 (IQR: 100–400).
ROC curve analysis (Fig. 3) showed that 3.2 cm was an optimal tumor size threshold with 70% sensitivity and 87% specificity for the prediction of EBL > 400 mL (95% confidence interval [CI]: 0.70–0.93, area under the curve [AUC] = 0.82, P < .001), and PADUA score of 9 was an optimal threshold with 75% sensitivity and 71.7% specificity for the prediction of EBL > 400 mL (95% CI: 0.63–0.94, AUC = 0.79, P = .001). A significant linear correlation between EBL volume and tumor size (R2 = 0.160, P = .001) is as shown (Fig. 4a). Similarly, increase in PADUA score is associated with increase in EBL volume (R2 = 0.14, P = .003) as shown in Figure 4b.

ROC curves and cut-off values of tumor size and PADUA score for EBL more than 400 mL. AUC, area under the curve; EBL, estimated blood loss; PADUA, the preoperative aspects and dimensions used for an anatomical; ROC, receiver operating characteristic.
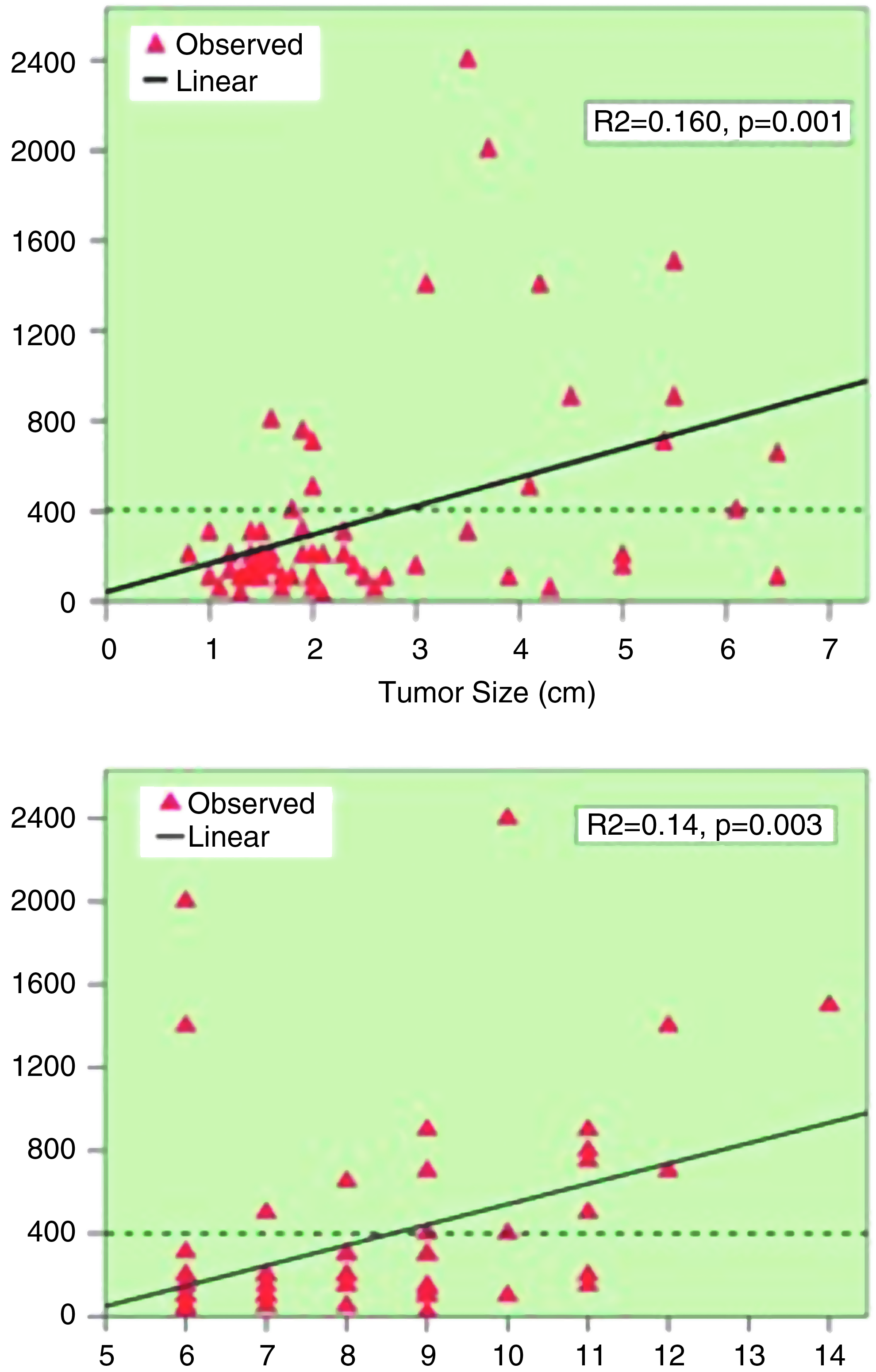
Graphs showing a significant linear correlation between the tumor size
Univariable analysis of factors associated with increased EBL (> 400 mL) showed that increased tumor size (odds ratio [OR]: 2.159, 95% CI: 1.392–3.346, P = .001) and higher PADUA score (OR: 2.022, 95% CI: 1.335–3.063, P = .001) were predictors. Regarding PADUA nephrometry parameters analysis, tumors between the renal sinus lines (OR: 6.852, 95% CI: 1.969–23.844, P = .002) and tumors invading the urinary collecting system (OR: 9.545, 95% CI: 2.553–25.693, P = .001) were risk factors of increased EBL >400 mL as shown in Table 1. Unfortunately, we could not perform the multivariable analysis due to small number of events (16) in relation to significant variables (4).
Numbers shown in bold denote statistical significance.
ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson's Comorbidity Index; CI, confidence interval; eGFR, estimated glomerular filtration rate; OR, odds ratio; PADUA, the preoperative aspects and dimensions used for an anatomical.
Table 2 summarized baseline characteristics and perioperative outcomes among off-clamp patients with tumor size ≤3.2 cm (group I) and tumor size >3.2 cm (group II). Group I had significantly larger mean tumor size (4.8 versus 1.7 cm, P < .001) and higher mean PADUA score (9.8 versus 7.7, P < .001). The median OT was longer (group II 163 minutes versus group I 116 minutes, P = .002) and median EBL was higher (group II 575 mL versus group I 150 mL, P = .004) on comparing both groups. There was no intraoperative organ injury or serious complications. There was increased tendency to conversion to RN in group II (12.5% versus 0%, P = .063) due to uncontrolled bleeding after tumor resection. All RN conversions were completed successfully using the robot. Three patients (18.8%) with tumor size >3.2 cm group were transfused, compared with 0% in patients with ≤3.2 cm (P = .015). Causes of blood transfusion were intraoperative hypotension (1 patient), and drop of hemoglobin postoperatively (2 patients). There was no statistically significant difference regarding LOS (P = .279), positive surgical margin rate (P = .597), and Clavien–Dindo complications ≥grade 3 (P = .611) between both groups.
Numbers shown in bold denote statistical significance.
ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson's comorbidity index; CKD, chronic kidney disease; EBL, estimated blood loss; eGFR, estimated glomerular filtration rate; IQR, interquartile range; OT, operative time; PADUA, the preoperative aspects and dimensions used for an anatomical; PSM, positive surgical margin; RN, radical nephrectomy; SD, standard deviation; WIT, warm ischemia time.
Regarding the renal function outcomes in our study, overall CKD upstaging was present in 22 patients (35.4%). Univariable logistic regression analysis showed that tumor size >3.2 cm (OR: 7.00, 95% CI: 1.994–24.569, P = .001) and EBL >400 mL (OR: 10.80, 95% CI: 2.854–40.873, P < .001) were risk factors for overall CKD upstaging, whereas multivariable analysis showed that EBL >400 mL (OR: 6.704, 95% CI: 1.597–28.146, P = .009) is the only predictor in Table 3.
Numbers shown in bold denote statistical significance.
ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson's Comorbidity Index; CI, confidence interval; EBL, estimated blood loss; eGFR, estimated glomerular filtration rate; OR, odds ratio; PADUA, the preoperative aspects and dimensions used for an anatomical.
Discussion
Recently, off-clamp RAPN is becoming widespread among urologists due to its potential advantages on renal function preservation.4,5 However, off-clamp RAPN is a surgically demanding procedure associated with risk of increased intraoperative bleeding than on-clamp RAPN.4–8 Most surgeons recommend off-clamp RAPN application for small, exophytic, and low-complex tumors.1,4,5,8,17 However, the cut-off values of tumor size and tumor complexity that are associated with increased risk of intraoperative bleeding remain uncertain. To the best of our knowledge, this is the first study that conducted to identify which patients are ideally suited for this technique. Our ROC curve analysis showed that a cut-off tumor size of 3.2 cm and PADUA score of 9 were optimal thresholds for increased EBL > 400 mL. Patients with tumor size >3.2 cm had significantly longer OT, higher EBL volume, more transfusion rate, and increased tendency of conversion to RN compared with tumor size ≤3.2 cm. In addition, EBL > 400 mL was a predictor of overall CKD upstaging. When performing off-clamp RAPN, surgeons should always put in consideration the potential risk of increased intraoperative EBL, which may negatively affect the intraoperative patient's safety, postoperative patient recovery, and renal functional preservation.
In a multi-institutional data analysis of 886 RAPN performed by high-volume surgeons across 5 academic institutions, the mean EBL was significantly higher 228 versus 157 mL (P = .009) in matched off-clamp and on-clamp RAPN cohorts, respectively. 4 In another multicenter matched-pairs case–control study (26 off-clamp versus 104 on-clamp RAPN), EBL was higher in the off-clamp group (266.4 versus 284.6 mL, P = .048) and so was the rate of conversion to RN (0% versus 7.7%, P = .04). 6 White et al. in a prospective observational study reported their initial experience with off-clamp RAPN technique. They concluded that for selected small renal cortical masses, RAPN without renal hilar occlusion was associated with higher median EBL compared with RAPN with hilar control (569 versus 220 mL, P = .018). 8 Similarly, Ener et al. reported significant differences in mean LOS (3.8 versus 3.0 days, P = .02) and amount of mean EBL (85.9 versus 183.3 mL, P = .01) between the on-clamp and zero-ischemia RAPN, respectively. 7
Of note, increased EBL during PN may be associated with undesirable consequences in the recovery period. In a recent analysis of 199 patients who underwent PN, the authors identified the predictive factors of hemorrhagic complications (i.e., hematoma requiring blood transfusion, an arteriovenous fistula, a false aneurysm, or a postoperative decrease of hemoglobin >3 g/dL). Operative EBL >250 mL was the only predictor (P < .001). 9 In our study, the median EBL volume in patients with tumor size >3.2 cm was 575 mL and blood transfusion rate was 18.8%.
In the present study, PADUA score of 9 was a cut-off value for increased EBL >400 mL, and high PADUA score together was positively proportional to increase in EBL volume. Recently, Kim et al. evaluated off-clamp RAPN in the treatment of high-complex renal tumors. They concluded that it could be safely performed with complex tumors, but is associated with higher mean EBL compared with noncomplex tumors (403 versus 193 mL, respectively). 13 Of note, our analysis revealed that PADUA complexity score has no influence on the postoperative renal function status at last follow-up. Similarly, Kim et al. found no significant difference between high-complex and low-complex group in eGFR change following off-clamp RAPN. 13
A subanalysis of PADUA components showed that tumors invading the collecting system and tumors between the sinus lines are relevant risk factors for increased EBL >400 mL. We believe that totally endophytic tumors can be hardly treated with the off-clamp technique and certainly is associated with more blood loss; unfortunately, in our analysis only 3/62 patients (4.8%) had totally endophytic mass, so we could not reach to a meaningful result regarding this, and we do not recommend performing it on such a tumor.
Regarding the renal function at the last follow-up, the overall CKD upstaging was present in 22 patients (35.4%), despite zero ischemia application. Interestingly, EBL > 400 mL was the only predictor of overall CKD upstaging. This finding is supported by previous researchers. Wiener et al. 10 studied the predictors of postoperative decline in eGFR rate among 122 patients who underwent RAPN. EBL >200 mL was a relevant potential factor and they had to study its impact in a larger patient population and longer follow-up. In addition, Colli et al. 11 evaluated the surgical factors affecting early and late return of renal function after PN in 141 patients; they found that% change in hematocrit significantly affected the creatinine clearance at 1 and 6 months postoperatively. They concluded that an increase in intraoperative EBL adversely affects the postoperative renal function. Recently, proportional GFR change of the operated kidney was examined using preoperative and postoperative renal scintigraphy in 73 patients; the authors found that higher EBL has negative impact on postoperative proportional GFR. 12 Several mechanisms may explain the impact of increased intraoperative EBL on postoperative renal function. Walsh et al. 18 found that a decrease of 1.1–2.0 g/dL and >4.0 g/dL of hemoglobin was associated with an increased risk of kidney injury development 1.5 times and 4.7 times, respectively. Presumably, larger decrements in hemoglobin will reduce the oxygen-carrying capacity of blood to renal tubules. Furthermore, it may represent bleeding (subclinical or overt) with subsequent reduction of renal perfusion pressures and result in more perioperative blood transfusions that may carry additional risk of renal injury. There is increasing evidence that transfused red blood cells may precipitate organ injury, owing to red blood cell changes that occur during storage. 19 Notably, perioperative blood transfusion was a risk factor of postoperative acute kidney injury occurrence. 20 Future researches are needed to exactly determine the actual relation between EBL volume and postoperative renal function.
The main drawbacks of our study are its retrospective study design and relatively small number of patients. Nevertheless, to our knowledge, this represents the first report of zero ischemia RAPN, which identified the ideal tumor size and complexity that are associated with less intraoperative bleeding. Of note, our results with a single expert surgeon and a tertiary referral institution might not be representative of other centers with early robotic experience. Another limitation was renal function assessment based on eGFR, and not renal scan, which would represent the most reliable tool to use in this setting. The present study was not designed to compare off-clamp RAPN with other clamping techniques, but rather to describe our surgical technique and outcomes to identify how far we shall proceed.
In conclusion, off-clamp RAPN is a technically demanding operation, associated with more blood loss and increased risk of intraoperative complications if performed in large size and complex tumors. For maximal patients' safety, it should only be carried out with a high-volume robotic team, and each patient should be selected carefully for optimal perioperative and functional outcomes. Our findings suggest that tumors >3.2 cm and PADUA score ≥9 are associated with risk of increased intraoperative blood loss and perioperative blood transfusion. In addition, EBL volume of >400 mL is associated with CKD upstaging despite of zero ischemia application. Further prospective studies with larger cohorts are warranted to validate our findings.
Ethical Standards Statement
Our study was approved by the Ethics Committee Review Board of the Yonsei University College of Medicine. Ethical approval number is 2014-0091-001. All patients were fully informed with regard to the off-clamp RAPN surgical approach and its possible complications.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.