
Abstract
Abstract
Introduction:
Endoscopic anterior component separation (ECS) techniques facilitate tension-free midline closure of wide ventral hernia defects. We describe a novel approach with a precostal incision and a new cylindrical balloon trocar.
Materials and Methods:
A single-center analysis of 19 patients undergoing ECS between January 1, 2014 and August 2, 2017 was performed with regard to improvement of technique. We currently start with a lateral precostal incision. This access in a low-fat and stable area allows for easy identification of the external oblique muscle with the ribs functioning as dorsal abutment for entering the correct plane between external and internal oblique muscles. Then a trocar is inserted with a cylindrical ballon, thus providing sufficient pneumatic widening of the dissection plane. A second 5-mm port is inserted under direct vision below the 12th rib. From there a unidirectional incision of the external oblique aponeurosis is performed from subcostal to the inguinal ligament. If necessary, the cephalad muscular parts of the external oblique can be transected over several centimeters in both directions starting from the precostal incision.
Results:
We documented no procedure-related complications apart from two hematomas that required no interventions. Four procedures were carried out on one side and the remaining ones bilaterally. In one case, a conversion to conventional open component separation was required due to extensive scarring after open cholecystectomy. There were no notable abdominal bulgings or lateral hernias during a structured postoperative follow-up period of 1 year postoperatively.
Discussion:
The technique described offers advantages in terms of determination of the correct entry point for ECS, regardless of abdominal wall conditions and the precostal access allows for unidirectional dissection toward the inguinal ligament with only two trocars in total. The cylindrical shape of the balloon trocar provides adequate widening of the working space and ensures good overview for safe dissection.
Introduction
C
Ramirez took it up in 1990 to close large abdominal wall defects in adults with concomitant posterior rectus sheath release. 2 However, extensive subcutaneous dissection is necessary to reach the lateral abdominal wall compartments when starting from the midline, and wound complications, such as hematoma, skin ischemia with dehiscence up to necrosis, and infection, occur in up to nearly 50% of patients.3,4
With this issue in mind, perforator sparing 5 and minimally invasive, endoscopically assisted techniques arose to overcome these problems. Regarding the latter ones, up to now, several techniques have been described having in common an abdominal approach at least 2 cm lateral apart from the semilunar line. A balloon port is introduced and inflated subcutaneously and anterior to the EOA,6,7 or more commonly deep to8,9 the EOA (i.e., between the external and internal oblique muscles). Obesity, redundant wobbly skin, and abdominal wall laxity make anatomical orientation and identification of the correct entry point difficult. Especially in obese patients relative movements of ultrasound marks on movable skin and the real lateral border of the rectus compartment also depend on positioning of patients on the operation table. Moreover, larger incisions may be necessary to expose the EOA and to identify it by the orientation of its fibers. This in turn may lead to air leaks that complicate the procedure.
Our improvement of the technique is based first on a thoracic precostal incision over the muscular parts of the external oblique. There is less fat anterior to the ribs and no risk of entering the plane beneath the internal oblique muscle where the neurovascular bundles can be injured. The ribs act as stable corsett providing dorsal counterfort. Second, a novel cylindrical balloon port is used and provides extended widening of the working space from the subcostal area to the inguinal region with excellent overview immediately from the beginning of the dissection.
Materials and Methods
In a retrospective review of prospectively collected data from the Herniamed registry, 10 19 patients underwent elective surgical repair of symptomatic midline incisional hernias with endoscopic anterior component separation (ECS) at the Department of General Surgery Congregation Hospital, Linz, Austria between January 1, 2014 and August 8, 2017. All cases were evaluated in telephone interviews and patients were asked about body asymmetria or bulging of the lateral abdominal wall in order to not overlook long-term complications of ECS that are not listed in the Herniamed registry. This is an Internet-based English- and German-language registry for the entire spectrum of inpatient and outpatient hernia surgery; it is designed to improve the quality of patient care and provide valid data on outcome research. 10 Evaluated data were retrieved from patients' files and all patients were followed up in accordance with the regulations of Herniamed 10 —that is, postoperatively, after 1, and (scheduled) 5 and 10 years. Statistical evaluations were extended to descriptive calculations.
Technical description
We started our procedures with a retromuscular sublay mesh repair 11 using self-gripping Parietex polyester meshes (Parietex progrip mesh; Medtronic®, Vienna, Austria) without additional fixation and utilized ECS as an adjunct if required. Depending on the amount of tension necessary to bring the medial aspects of the anterior rectus sheaths together in the midline, we added an ECS “on demand.” It is important to have the arms of the patient tucked, at least for the time of ECS. The laparoscopic unit is placed at the foot-end of the operating table.
The first 20 mm transverse skin incision is made 13–15 cm away from the xiphoid depending on patient's height, and 4 cm above the costal arch (Fig. 1). Then the external oblique muscle is identified by the characteristic inferomedial direction of its fibers. Because of the origin of these fibers, ventral on the 5th–12th ribs, there is no risk of entering the plane underneath the internal oblique muscle, which inserts into the cartilages of the four lowest ribs. After blunt dissection of the external oblique muscle reaching the ribs below, the space between muscle and ribs can easily be identified and widened in the caudal direction with the surgeon's index finger. Using this technical approach, the external oblique muscle bulge can be exposed under direct vision through a small skin incision preventing leakage of air while performing the subsequent endoscopic release. Thereafter, the new cylindrical balloon trocar system (Spacemaker™ Pro Blunt Tip Trocar; Medtronic, New Haven, CT), is carefully advanced through the dissected external oblique fibers and entering the interoblique space below the costal margin. This device is the next generation of all-in-one access and dissector system for abdominal wall repair with a cylindrical dissection balloon developed for ECS (Fig. 2).

Thoracic precostal access 13–15 lateral of the xiphoid (dependent on patient's height) and 4 cm cephalad to the costal arch.

Spacemaker™, Medtronic® all-in-one access and dissector system with a cylindrical dissection balloon dedicated for endoscopic component separation.
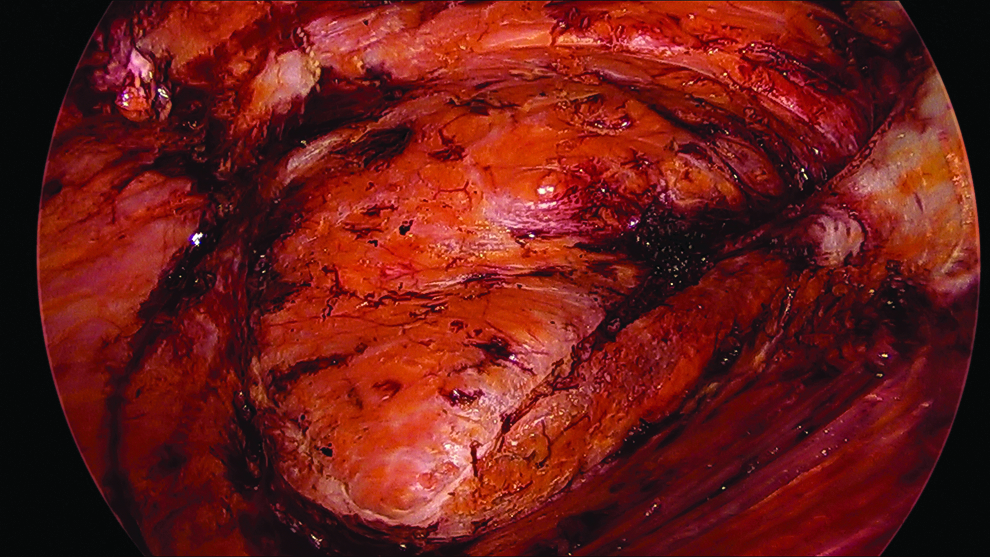
The balloon is inflated under videoendoscopic visualization (Fig. 3) using a 10 mm/30° laparoscopic optic (Fig. 4). After removal of the balloon and gas insufflation up to a pressure of 12 mm Hg, an adequate overview of the whole space between the external and internal oblique muscles is provided (Fig. 5). Thereafter, a second 5-mm port can be inserted 3–4 cm lateral to ensure starting the ECS as far cranial as practicable (Fig. 6).
Inflated cylindrical balloon under laparoscopic view using a 10 mm/30° optic.

View from outside during balloon insufflation with skin transillumination.

Overview of the space between the left external and internal oblique muscles after removal of the balloon and gas insufflation (blue arrow, external oblique muscle; black arrow, semilunar line; green arrow, internal oblique muscle).

Insertion of a second 5-mm port 3–4 cm lateral at the level of the lowest ribs to ensure starting the ECS as far cranial as practicable. ECS, endoscopic anterior component separation.
There is the advantage compared with abdominal access to work in a unidirectional caudal direction with the need of only two trocars in total, avoiding inverse dissection. The correct starting point for the ECS is at the EOA ∼2 cm lateral to the white fibrous tissue lateral to the rectus border (linea semilunaris) and medial to the muscular parts of the external oblique muscle.
After identification of the junction of the muscular and aponeurotic portions, a laparoscopic monopolar hook is used to incise the EOA from underneath. Subcutaneous fatty tissue must appear in the line of transection (Fig. 7); if muscle tissue is exposed, the starting point was chosen either too far lateral (external oblique muscle fibers) or too far medial (rectus muscle). Then the dissection extends in craniocaudal direction right to the inguinal ligament. Lateral fine fibers between the external and internal oblique layers, referred to as “spiderwebs” or “angel hair” should be dissected in a space devoid of nerves and vasculature. This means that the external oblique muscle and the underlying internal muscle are widely separated to obtain more muscle release, and additional advancement of both rectus muscles. The rectus muscles with the overlying anterior fibrotic sheath and the attached internal oblique-transversus muscle complex can be advanced ∼8–10 cm at the waistline on both sides. 2
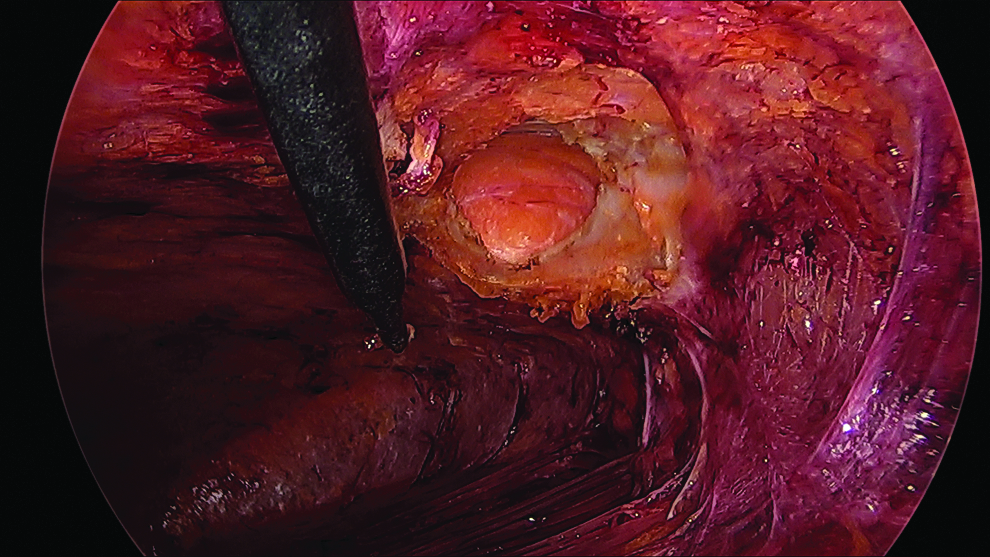
Entry point for division of the external oblique aponeurosis 2 cm lateral from the semilunar line demonstrating the subcutaneous tissue anterior to the aponeurosis.
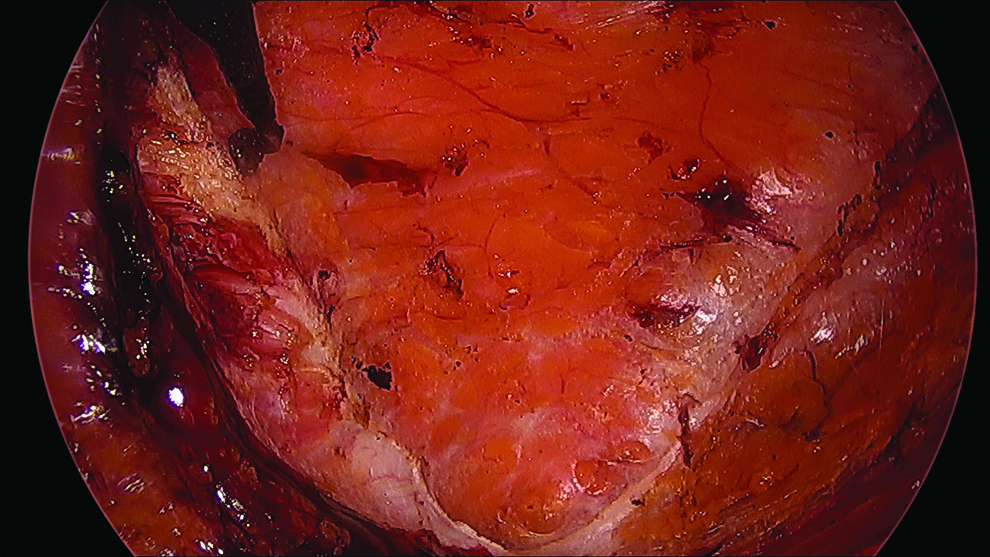
Furthermore, the subcutaneous scarpa fascia should be transected for additional tension release while particular care is taken not to injure the skin in thin patients. It is helpful to gently press against the lateral abdominal wall to bring the tissue closer to the operation field exactly to the spot where the dissection is just being carried out; by doing so, angled instruments are not necessary. Figure 8 shows the medial, and Figure 9 the lateral edges of the split and divided external aponeurosis. The endoscopic view of the eventual surgical field is depicted in Figure 10. If a wide epigastric hernia defect requires extensive detachment of the external muscles above the lower ribs this can be achieved at the end of the endoscopic procedure. After removal of the port system, an open dissection is done through the same wound for several centimeters in both directions, starting from the precostal incision by using wound retractors equipped with lights, or simply with the help of the laparoscopic light source. No drains are used, and only the skin is closed.
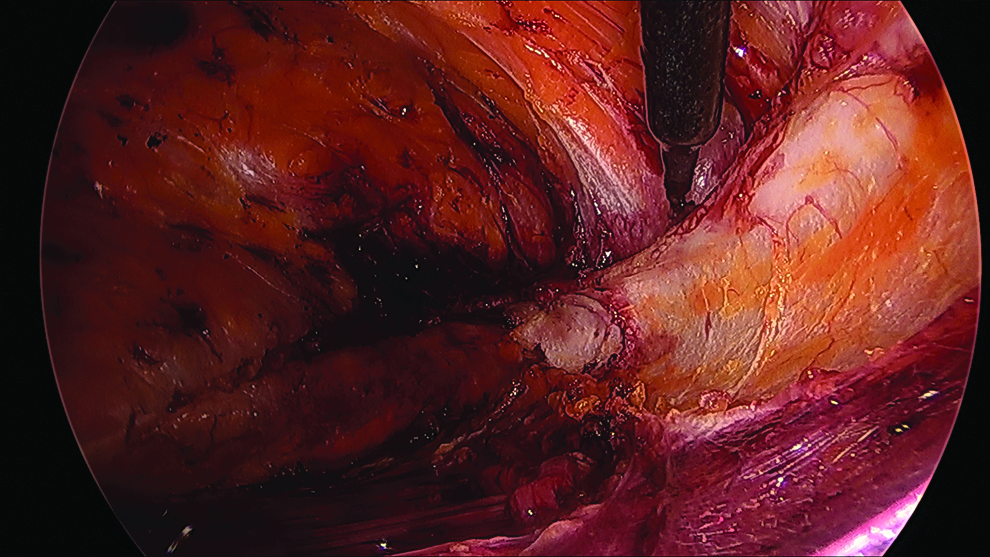
Medial edge of the divided external oblique aponeurosis.
Lateral edge of the divided external oblique aponeurosis.
Endoscopic view of the eventual surgical field.
Results
Between January 2014 and August 2017 ECS was performed in a total of 19 patients unilateral (n = 4) and bilateral (n = 15). The aforementioned technique was used only in the last three cases because of constant efforts for improvement. This series contains our learning curve with the ECS approach subdivided into two different types of surgical access (abdominal and thoracic).
During the first 16 cases, we used an abdominal subcostal approach and a trocar with a round balloon initially developed for total extraperitoneal inguinal hernioplasty was inserted. All patients were treated electively with sublay mesh repair due to midline hernias, and ECS was added to facilitate tension-free midline closure of the anterior rectus sheath. Patient demographics and disease characteristics are displayed in Table 1. For the hernia classification according to the European Hernia Society recommendations, 12 we report only on the width of the hernia defect, which is relevant for the treatment option. Relevant outcome data are presented in Table 2. 13 There were no procedure-related complications with the exception of two hematomas requiring only heparin withdrawal. In one case, conversion to open CS was required due to extensive scarring after open cholecystectomy due to gangrenous cholecystitis with consecutive wound infection of the lateral parts of the subcostal wound requiring vacuum-assisted wound therapy for 3 weeks. A total of 33 ECS procedures were performed (15 bilateral with 1 conversion = 29 and 4 unilateral). There were no late complications during a structured postoperative follow- up of 1 year. In addition, a telephone survey was carried out in which no patient reported abdominal bulging or lateral hernias.
ECS, endoscopic anterior component separation.
Discussion
ACS techniques have evolved significantly over recent years with efforts to reduce operative trauma and wound morbidity. ECS techniques aim to preserve the blood supply of the abdominal wall resulting in significantly fewer wound-healing complications 14 compared with the traditional ACS.3,4
We started off doing minimally invasive ACS in 2012 with a simple transection of the EOA 15 by using a modified Collin Hartmann retractor with lengthened arms inserted into two lateral abdominal incisions. Once introduced, traction separates the EOA from the underlying internal oblique muscle and the aponeurosis is transected with a long terminal cautery in both directions. The relatively avascular plane located between the two planes makes this “blind”separation possible. But there are concerns of limited overview to ensure staying in the right plane because entering the space between the internal and transversus abdominis muscles must strictly be avoided to not cause severe bleeding and nerve injuries. Moreover, a disrupture of the anatomical planes can entail nonmidline hernias, which are diffcult to treat. With this technique only an incision but no actual separation of the layers is possible. Only the endoscopic approach gives excellent visualization of anatomical planes and allows for complete separation of the internal and external oblique layers. We therefore changed our technique introducing a balloon trocar system 9 and started with an abdominal subcostal incision. Redundant and movable skin and excessive subcutaneous tissue masked the right entry point even after skin marking with ultrasound. Furthermore, three trocars were needed and after craniocaudal dissection we had to move the monitor to the top and continued working in the opposite direction. We initially used a round balloon trocar which creates only a small space after expansion so the insertion of a second trocar was challenging because of limited overview. It is worth mentioning that it is not sufficiently possible to dissect the requested plane with blunt technique by using a common trocar system. Gas insufflation without previous pneumatic space creation does not provide adequate overview for safe identification of the correct entry point. The round balloon system often had to be repositioned in between the layers to create more space; dissection was more time consuming and less safe. In conventional ECS with an abdominal access, dissection in-between camera and working trocars to complete the cranial release can be challenging due to back-to-front dissection with difficult triangulation and poor angulation between the laparoscopic instruments. Furthermore, the procedure can be complicated by repositioning the laparoscopic unit and the screen at the patient's head to be able to work in the cranial direction. The improved novel technique described in the methods section offers the advantages of easy and quick identification of the correct entry point, excellent overview, and unidirectional dissection. The ECS procedure-related duration of surgery could be reduced from 21 to 10 minutes for either side.
The discussion of whether to start with rectus sheath dissection or ECS remains controversial. Approaching the lateral compartment first provides the benefit of a relatively stable operating field. However, ECS takes place before evaluating its necessity. It is not only the width of the hernia defect that determines the need for CS, but it also depends on the patient's body height, visceral fat amount, and abdominal wall compliance. Overtreatment must be assumed in some cases when doing ECS first. Thus, we prefer starting the surgical procedure with a median laparotomy. Adhesions are freed from the abdominal wall and the peritoneal sac is dissected from the subcutaneous tissue; then the posterior rectus sheath is detached and the retromuscular mesh place is prepared. At this point, the need for component separation to achieve a tension-free closure of the midline is evaluated. Our practice is to perform ECS when the linea alba cannot be reapproximated in a tension-free manner. We call this strategy ECS “on demand.” 16
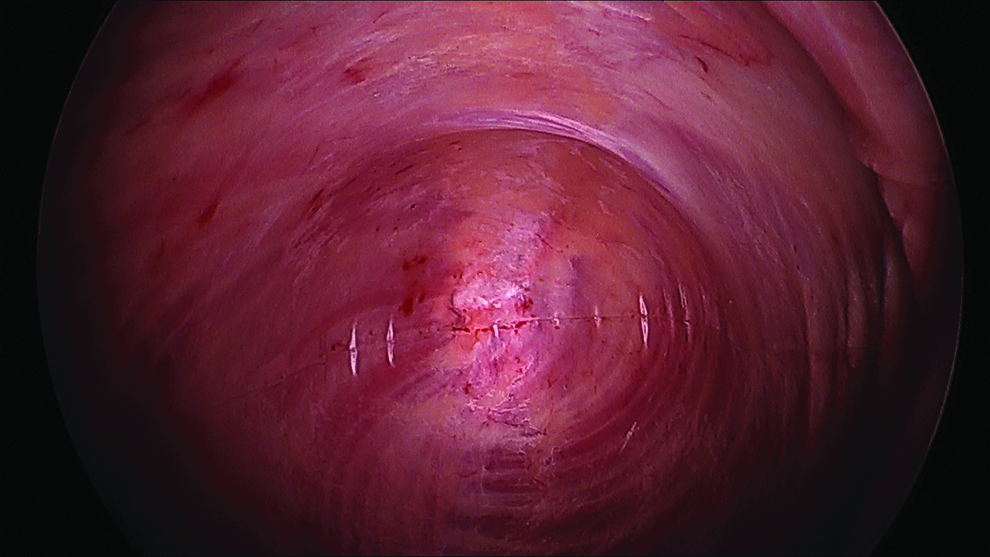
In our experience, lateral abdominal scars are not a contraindication for ECS since the inflated cylindrical balloon typically shows an hourglass configuration in these cases (Fig. 11). If there is a clear view in front of the narrowing and sometimes even behind it, it is possible to release the scar tissue safely step-by-step in most cases. This allows succeeding division of the scarry tissue in most instances. Scars from ostomy takedowns or “McBurney” incisions are usually easy to overcome, but subcostal scars can be tricky due to the close association with the desired entry point for ECS.
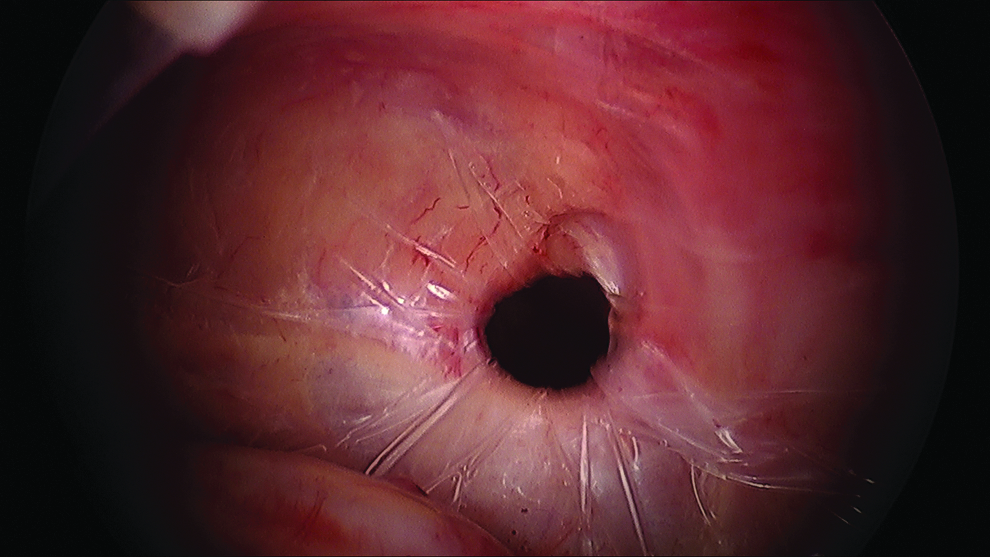
Hourglass-shaped form of the cylindrical balloon after inflation due to scarring of the lateral abdominal wall compartment.
Of note, by using the minimally invasive approach, a smaller extent of rectus medialization might be achieved compared with a formal open ACS in “Ramirez” technique. 2 Rosen et al. 9 tried to address this issue. In pigs, an average of 86% of the open anterior technique's effect in medialization could be gained with the endoscopic anterior release. To what extent these numbers are applicable for human patients remain completely unclear. In fact, the releasing effect of wide subcutaneous dissection may be underestimated. Large undermining skin flaps result in several centimeters of abdominal wall advancement. In open repair of large incisional hernias, substantial skin and subcutaneous tissue flaps must frequently be mobilized to remove redundant and/or ischemic skin and to improve cosmetic results. Furthermore, an expanded hernia sac often must be dissected far laterally, and by doing so, the medial aspect of the EOA is often exposed. Therefore, ECS is not prudent in these cases since wide skin flaps are already created. 17
In recent years, posterior component separation techniques have been popularized. Carbonell et al. described the approach outside the semilunar line between the internal oblique and transversus abdominis muscles. 18 This approach did not gain approval because this plane contains the neurovascular bundles. On the contrary, the transversus abdominis release (TAR) technique 19 received broad support. The main advantage is the possibility to put in large meshes and cover lateral and midline defects without the need for mobilizing large subcutaneous flaps, because a large retromuscular/preperitoneal plane is created. There is a study published, comparing traditional Ramirez ACS with TAR on the rate of defect closure. The percentage of tension-free midline closure was nearly equal, but the study was confounded by insignificantly larger defects (on average 60 cm2) in the ACS group compared with the TAR group. 20 In our experience, the achievable amount of rectus medialization is clearly smaller in TAR procedures.
Placement of a mesh in the sublay space does not reinforce the laterally released area. Regarding our study results, the intact internal oblique and transversus abdominis muscles seem to be sufficient to prevent lateral hernias and bulges, respectively.
In conclusion, we are convinced that the described new technique is a helpful advancement of ECS in terms of an easier and reproducible access beneath the external oblique muscle with a stable entry point, better intraoperative overview due to the cylindrical balloon design, and the advantage of unidirectional dissection because of the cranial precostal trocar position with need for only two ports.
Footnotes
Disclosure Statement
G.K. has received honorariums from Medtronic, Dahlhausen, and Bard for lectures and educational activitities. L.N.J. has received honorariums from Medtronic for lectures and educational activitities. For all other authors no competing financial interests.