
Abstract
Abstract
Aim:
This meta-analysis aims at comparing laparoscopic intersphincteric resection (LISR) with conventional open ISR (OISR) for low rectal cancer (LRC) in terms of intraoperative, postoperative, pathological, and survival outcomes.
Materials and Methods:
A systematic literature search with no limits was performed in PubMed and Ovid. The last search was performed on May 27, 2017. The outcomes of interests included intraoperative outcomes: operative time and blood loss; postoperative outcomes: hospital day, postoperative hospital day, time to first flatus, time to normal diet, ileus, intra-abdominal abscess, anastomotic leakage, anastomotic stricture, wound infection, pneumonia, urinary complication, morbidity, and mortality; pathological outcomes: lymph node harvested, R0 resection rate, distance of proximal resection margin, distal resection margin and circumferential resection margin (CRM), and positive CRM; survival outcomes: 3-year overall survival (OS), 3-year disease-free survival (DFS), 5-year OS, and 5-year DFS.
Results:
Six articles and two abstracts published between 2010 and 2016 were included in our meta-analysis. When compared with OISR, LISR was associated with comparable operative time, less blood loss, shorter length of postoperative hospital day, quick time to first flatus, less incidence of morbidity, and pneumonia. Besides, the two groups were comparable in pathological and survival outcomes.
Conclusions:
Our results demonstrated that LISR had comparable operative time, less blood loss and postoperative morbidity, and comparable pathological and survival outcomes when compared with OISR. So LISR was safe and feasible in LRC surgery. Besides, more randomized clinical trials are needed to investigate the deeper effect of LISR in the future.
Introduction
R
Once upon a time, APR was regarded as a classic procedure and was widely used for LRC. 11 Nevertheless, with the development of surgical techniques and the increasing demand of anus preservation, sphincter-saving approaches were proposed and have been widely applied for LRC, including ISR, which was first reported in 1994. 12
Laparoscopic techniques have been broadly accepted for gastrointestinal surgery. 13 Several studies have demonstrated that laparoscopic surgery is safe and feasible for colon cancer in regard to short- and long-time outcomes. 14 However, as for RC, the narrow pelvic cavity can be a limitation to laparoscopy. 15 Although some studies have reported that the long-time outcomes of laparoscopic surgery were not inferior to conventional open surgery in RC, the data for specific surgical procedures are still lacking.16,17 Several studies compared laparoscopic ISR (LISR) with open ISR (OISR) for LRC, but the sample size was small and the results were not consistent.18,19 So we conducted this meta-analysis to compare LISR with OISR in terms of short- and long-time outcomes.
Materials and Methods
Study selection
We did a systematic literature search in PubMed and Ovid for studies that compared LISR with OISR for RC. The search terms included “intersphincteric resection or ISR” and “laparoscopic, laparoscopic-assisted, or laparoscopy” and “open, or laparotomy” and “rectal cancer, rectal carcinoma, or rectal adenocarcinoma.” The last search was performed on May 27, 2017. We also performed a manual search of references of articles and reviews for additional potentially eligible studies.
Inclusion and exclusion criteria
The inclusion criteria for this meta-analysis were as follows: (1) case–control study (LISR versus OISR); (2) RC; (3) studies with a total sample size more than 20; and (4) intraoperative and/or postoperative outcomes were reported. The exclusion criteria studies were as follows: (1) review articles; (2) correspondences or editorials; (3) studies including benign diseases such as inflammatory bowel disease or polys; (4) animal studies; (5) single-arm studies; and (6) abstract without detail data.
Data extraction
Two authors (X.Z. and Q.W.) reviewed all the identified articles independently. They would solve the discrepancies by discussion first, and a third reviewer (Z.W.) would be required if necessary. We extracted the following items from each study: first author's name, year of publication, country, publication type, study type, bowel preparation, number of patients in each arm, gender, age, body mass index (BMI), previous abdominal surgery (PAS), tumor stage, location to anus, tumor size, preoperative chemoradiotherapy (CRT), and outcomes of interests.
Outcomes of interests
Intraoperative outcomes: Operative time, blood loss.
Postoperative outcomes: Length of hospital stay and postoperative hospital day, time to first flatus, time to normal diet, ileus, intra-abdominal abscess, anastomotic leakage, anastomotic stricture, wound infection, intra-abdominal abscess, incidence of pneumonia, urinary complication, morbidity, and mortality.
Pathological outcomes: Lymph node harvested, R0 resection rate, distance to proximal resection margin (PRM), distal resection margin (DRM) and circumferential resection margin (CRM), and positive CRM.
Survival outcomes: Three-year overall survival (OS), 5-year disease-free survival (DFS), 5-year OS, and 5-year DFS.
Quality assessment
The methodological quality of the enrolled retrospective studies was assessed by using the revised and modified grading system of the Scottish Intercollegiate Guidelines Network. Articles achieving less than 8 scores, 8–14 scores, and more than 14 scores (total score, 20) were defined as poor quality, fair quality, and good quality, respectively. 20
Statistical analysis
All data analyses were conducted by using the Review Manager version 5.0 (The Cochrane Collaboration, Software Update, Oxford), and P < 0.05 was considered statistically significant. Weighted mean difference (WMD) was calculated for the continuous outcomes, and pooled odds ratios (OR) or risk ratios (RR) were calculated for the dichotomous outcomes. For continuous outcomes, if the study only provided means and range values or median and range values, the means and standard deviations were calculated by using methods described by Hozo et al. 21 Chi-squared test and Higgins I2 test were used for the heterogeneity test. A value of P < 0.05 and I2 > 50% was regarded as existing heterogeneity. If I2 > 50% and P < 0.05, a random-effects model was applied. Correspondingly, if I2 < 50% and P > 0.05, a fixed-effects model was applied. Begg's funnel plot was used to evaluate publication bias. The survival curves in articles were obtained by Engauge Digitizer version 4.1.
Results
The process and result of literature searching were shown in Figure 1. The initial search algorithm retrieved a total of 370 studies. There remained 227 studies after removing the duplications. After reviewing titles and abstracts, only 19 relevant studies were kept for further evaluation. Besides, no additional record was identified through manual search. Among these studies, 11 literatures were excluded due to the following reasons: 6 studies were conference abstracts without detail data; 2 studies were without data or with other issues; 2 studies were editorial or correspondence; and 1 was a review article. Finally, six articles18,19,22–25 and two abstracts26,27 published between 2010 and 2016 were included in our meta-analysis. The characteristics of the included studies were summarized in Table 1. A total of 894 patients (515 by LISR and 379 by OISR) were enrolled.
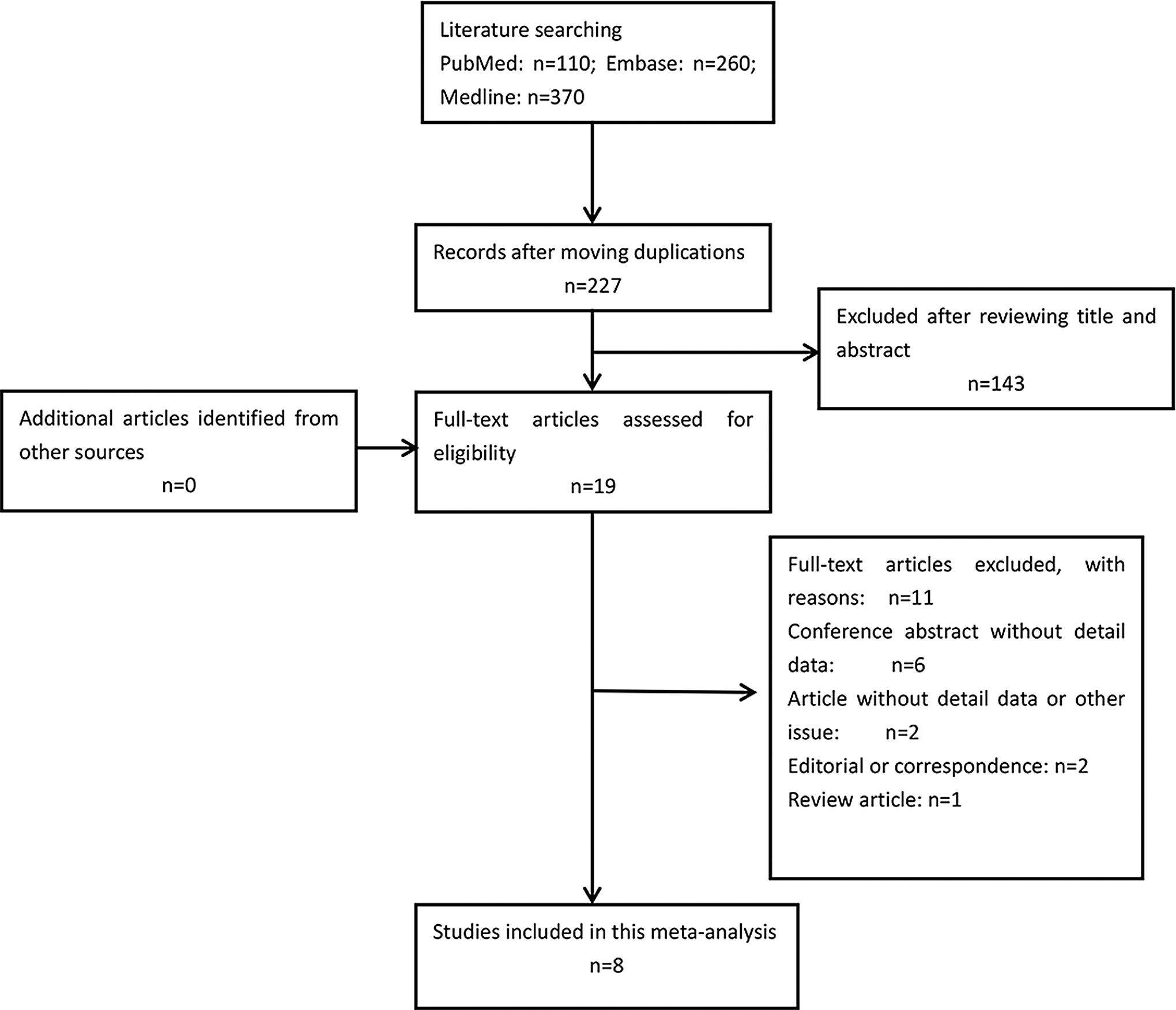
PRISMA diagram.
BMI, body mass index; CRT, chemoradiotherapy; LISR, laparoscopic intersphincteric resection; NR, not report; OISR, open intersphincteric resection; PAS, previous abdominal surgery; RCCS, retrospective case-control study.
Patient demographics
The results demonstrated that the two groups were comparable in terms of age (P = 0.61, WMD = 0.48, 95% confidence interval [CI] −1.37 to 2.34, I2 = 52%), male gender (P = 0.29, OR = 0.84, 95% CI 0.61–1.16, I2 = 0%), BMI (P = 0.13, WMD = −0.39, 95% CI −0.88 to 0.11, I2 = 0%), tumor stage (P = 0.63, OR = 1.09, 95% CI 0.77–1.54, I2 = 25%), distance to anus (P = 0.21, WMD = −0.26, 95% CI −0.68 to 0.15, I2 = 90%), tumor size (P = 0.32, WMD = −1.37, 95% CI −4.10 to 1.35, I2 = 58%), PAS (P = 0.59, OR = 0.86, 95% CI 0.50–1.48, I2 = 0%), and preoperative CRT (P = 0.12, OR = 1.47, 95% CI 0.90–2.39, I2 = 49%).
Quality of included studies
All of the six articles18,19,22–25 were retrospectively studies. Among them, one 22 was of high quality (15 scores), and the other five were of fair quality (9–13 scores) (Table 2).
Total scores, 20; <8, poor quality; 8–14, fair quality; >14, good quality.
LISR, laparoscopic intersphincteric resection.
Meta-analysis of intraoperative outcomes
We found that there was no significant difference in operative time (P = 0.17, WMD = 22.14, 95% CI −9.44 to 5.72, I2 = 92%). However, the LISR group had significantly less blood loss when compared with the OISR group (P < 0.001, WMD = −123.40, 95% CI −172.57 to −74.22, I2 = 86%) (Fig. 2).
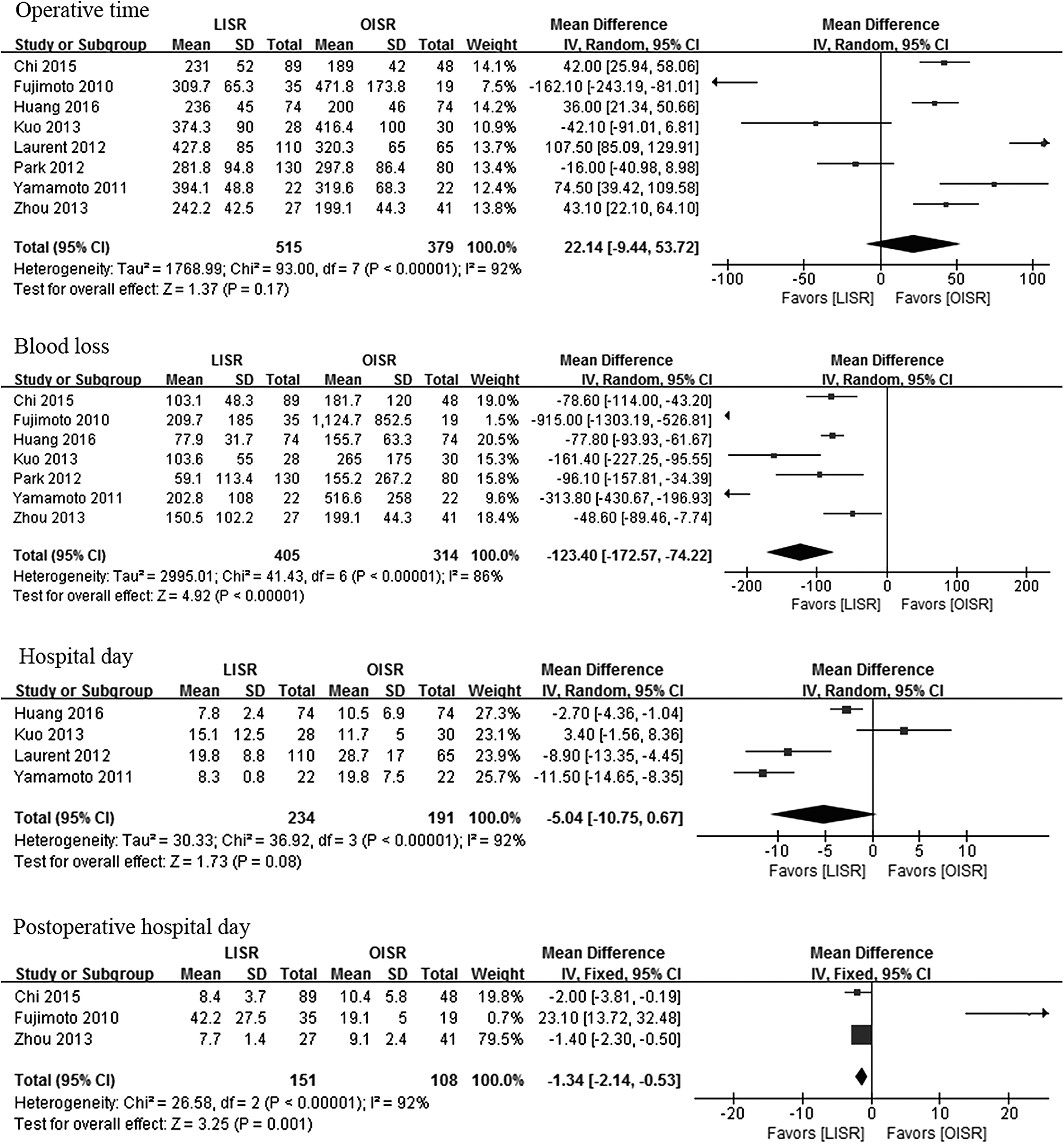
Meta-analysis of intraoperative outcomes and postoperative recovery. CI, confidence interval; LISR, laparoscopic intersphincteric resection; OISR, open intersphincteric resection.
Meta-analysis of postoperative outcomes
Although no significant difference was found in total hospital day (P = 0.008, WMD = −5.04, 95% CI −10.75 to 0.67, I2 = 92%) between the two groups, postoperative hospital day was significantly less in the LISR group (P = 0.001, WMD = −1.34, 95% CI −2.14 to −0.53, I2 = 92%). Besides, the results also revealed that patients in the LISR group had shorter time to first flatus (P < 0.001, WMD = −0.56, 95% CI −0.87 to −0.25, I2 = 8%), but time to normal diet was comparable between the groups (P = 0.47, WMD = 1.07, 95% CI −1.83 to 3.98, I2 = 98%) (Fig. 2).
When it comes to postoperative complications, the LISR group had significantly less morbidity (P = 0.01, OR = 0.64, 95% CI 0.45–0.91, I2 = 0%) and incidence of pneumonia (P = 0.01, OR = 0.33, 95% CI 0.14–0.76, I2 = 0%). In addition, there was no significant difference between the two groups in terms of ileus (P = 0.28, OR = 0.54, 95% CI 0.18–1.66, I2 = 0%), intra-abdominal abscess (P = 0.57, OR = 1.22, 95% CI 0.62–2.38, I2 = 0%), anastomotic leakage (P = 0.44, OR = 0.69, 95% CI 0.27–1.77, I2 = 0%), anastomotic stricture (P = 0.54, OR = 1.79, 95% CI 0.28–11.51, I2 = 0%), wound infection (P = 0.14, OR = 0.36, 95% CI 0.09–1.40, I2 = 0%), urinary complication (P = 0.85, OR = 1.13, 95% CI 0.32–3.98, I2 = 0%), or mortality (P = 0.33, RR = 0.21, 95% CI 0.01–5.00, I2 = not applicable) (Fig. 3).
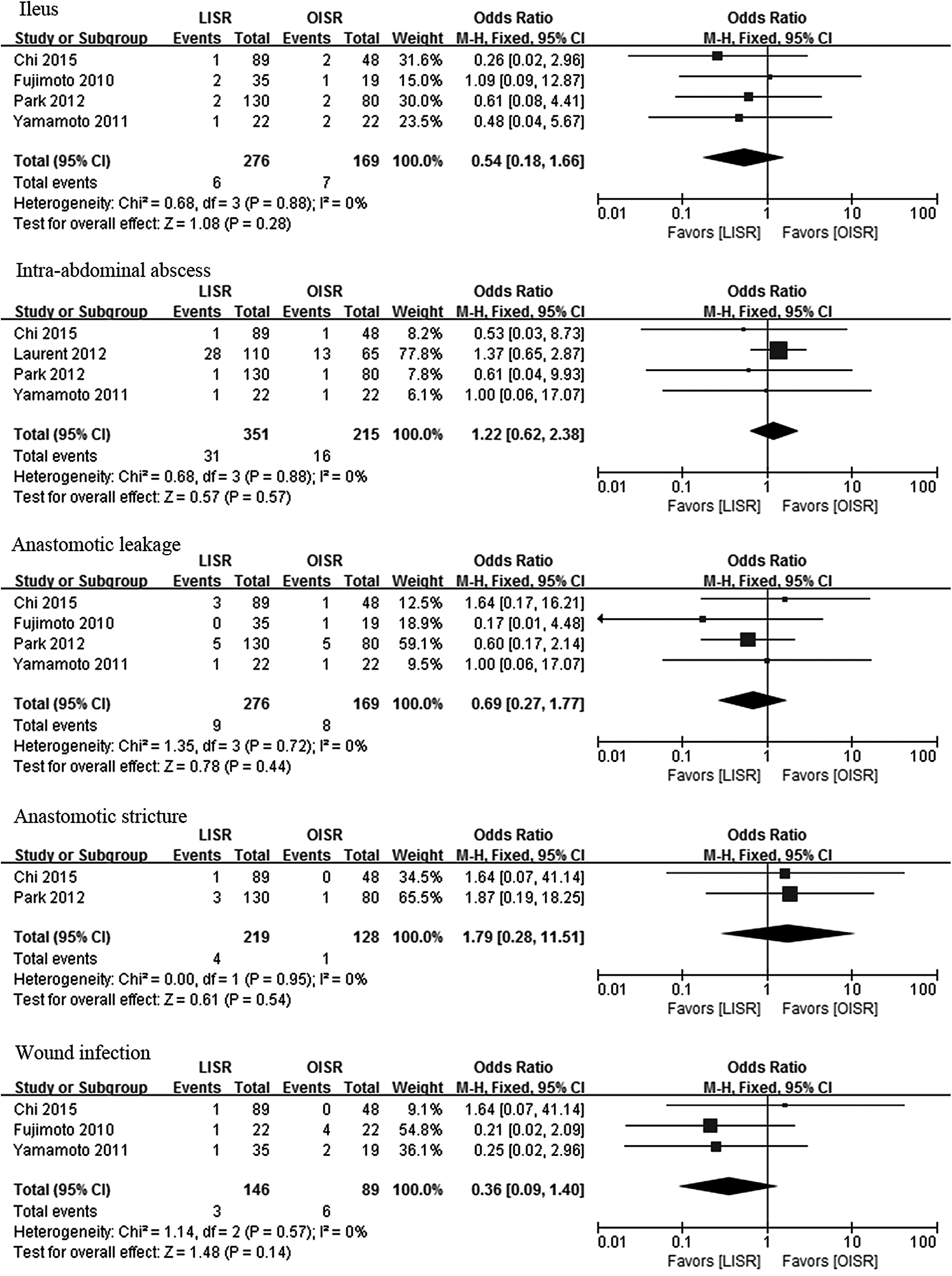
Meta-analysis of postoperative complications. CI, confidence interval; LISR, laparoscopic intersphincteric resection; OISR, open intersphincteric resection.
Meta-analysis of pathological outcomes
As for pathological outcomes, we found that the two groups were comparable in R0 resection rate (P = 0.49, OR = 1.91, 95% CI 0.30–12.25, I2 = 0%), distance of CRM (P = 0.09, WMD = 0.59, 95% CI −0.09 to 1.26, I2 = 29%) and DRM (P = 0.26, WMD = 0.07, 95% CI −0.05 to 0.19, I2 = 20%), and positive CRM (P = 0.25, OR = 1.49, 95% CI 0.75–2.95, I2 = 35%). Besides, the results also demonstrated that the LISR group had longer PRM (P = 0.006, WMD = 1.49, 95% CI 0.43–2.54, I2 = 0%) and less lymph node harvested (P = 0.02, WMD = −1.58, 95% CI −2.89 to −0.26, I2 = 0%) (Fig. 4).
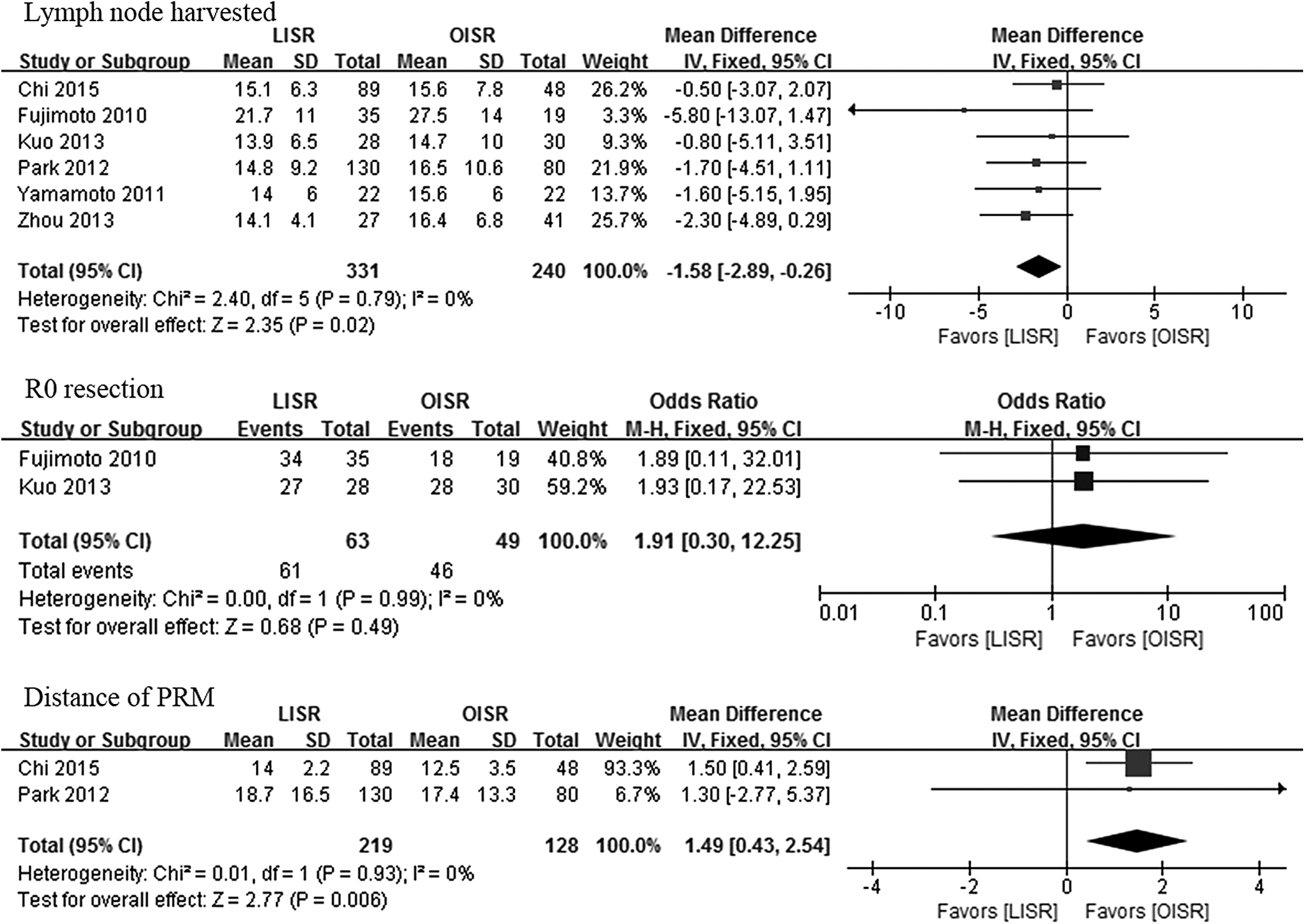
Meta-analysis of pathological outcomes. CI, confidence interval; CRM, circumferential resection margin; DRM, distal resection margin; LISR, laparoscopic intersphincteric resection; OISR, open intersphincteric resection; PRM, proximal resection margin.
Meta-analysis of survival outcomes
There was no significant difference between the two groups in terms of 3-year OS (P = 0.60, hazard ratio [HR] = 0.81, 95% CI 0.38–1.73, I2 = 0%), 3-year DFS (P = 0.79, HR = 0.93, 95% CI 0.54–1.60, I2 = 0%), 5-year OS (P = 0.94, HR = 0.96, 95% CI 0.39–2.41, I2 = 0%), or 5-year DFS (P = 0.93, HR = 0.97, 95% CI 0.52–1.82, I2 = 0%) (Table 3).
CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; LISR, laparoscopic intersphincteric resection; OISR, open intersphincteric resection; OS, overall survival.
Publication bias
A funnel plot of the studies reporting on morbidity shows that there was no obvious publication bias among the studies (Fig. 5).

Funnel plots of the studies reporting on morbidity.
Discussion
OISR for LRC was first reported in 1990s, and with the development of laparoscopic techniques, LISR was initially performed in the 2000s and has been widely used nowadays.12,28 However, compared with conventional OISR, the effect of LISR is still controversial duo to the different results of published studies. So we conducted this meta-analysis including 8 studies and 894 patients to compare LISR with OISR in terms of short-time and long-time outcomes.
Interestingly, different from previous meta-analysis,29,30 we found there was no significant difference between the two groups in operative time. This result was also supported by some other studies.22,23 On the one hand, with the development of the learning curve and accumulation of experience, surgeons can be more familiar and skillful when performing laparoscopic surgery. In addition, in the traditional process of ISR, both LISR and OISR have a similar perineal phase 25 and the long handle of laparoscopic techniques may make the operation more convenient in the deep pelvic floor. On the other hand, operative time can be affected by many factors such as abdominal adhesion, BMI, tumor location, tumor size, and intraoperative incidence. Although we did not find any difference in the factors mentioned earlier between the two groups, we cannot deny the existence of particular cases that can influence the whole results.
In line with previous meta-analysis,16,31 the LISR group had significantly less blood loss than the OISR group. With the development of surgical techniques, electrocoagulation instruments such as electrotome and harmonic scalpel have been widely used, which can greatly help reduce the blood loss in surgery. However, we believe that laparoscopic surgery has a magnified and clearer image, 32 and with the help of a long handle, surgeons can reduce the unnecessary injury to blood vessels. So, the LISR group can have less blood loss.
Laparoscopic surgery is a minimally invasive technique that has a smaller incision length and less postoperative pain when compared with conventional open surgery.33,34 So when it comes to postoperative recovery, we found that patients in the LISR group had less postoperative day and quicker time to first flatus.
As for postoperative complications, we found no significant difference in wound infection though the LISR group had a small incision length. We believe that this may be related to the wide use of antibiotics and nursing level of the hospital. Nevertheless, the LIRS group had less morbidity when compared with the OISR group. The possible reason may be that patients in the LISR group had less stress response to surgery. Besides, we also found that the LISR group had less incidence of pneumonia, which may be because patients in the LISR group can walk out of bed earlier. As for anastomotic complications, no significant difference was found in the two groups. We believe that this may be because of the use of staples.
When performing cancer surgeries, surgeons will try to conform to the principle of radical resection. So, the R0 resection rate was similar in the two groups. And in terms of distance of DRM, CRM, and positive DRM, the two groups were also comparable. These results were also supported by a previous meta-analysis.35,36 However, against from previous studies,17,36,37 we found that the LISR group had less lymph node harvested. We believe that the number of lymph node harvested was associated with preoperative CRT and tumor stage. Besides, the learning curve of different pathologists can also affect the recognition of lymph node. And in survival outcomes, LISR was not inferior to OISR in 3-year and 5-year survival.
Some limitations of this study have to be highlighted. First, there existed high heterogeneity in some analyses. Though the sensitivity analysis was conducted by removing one study each time, the outcomes remained unchanged. We believed it might be influenced by many factors, such as the learning curve of the surgeon, bowel preparation, distance to anal verge, and PAS. Second, all of the enrolled articles were retrospective studies. This might induce patient selection bias.
In conclusion, our results demonstrated that LISR had comparable operative time, less blood loss and postoperative morbidity, and comparable pathological and survival outcomes when compared with OISR. So, LISR was safe and feasible in LRC surgery. Besides, more randomized clinical trials are needed to investigate the deeper effect of LISR in the future.
Footnotes
Acknowledgment
This work was supported by the Science and Technology Support Program of the Science & Technology Department of Sichuan Province (Grant number: 2016SZ0043).
Disclosure Statement
No competing financial interests exist.