
Abstract
Abstract
Objective:
To investigate the clinical effect of the laparoscopic cholecystectomy (LC) after percutaneous transhepatic gallbladder drainage (PTGD) in elder acute cholecystitis.
Methods:
The Cochrane Library, PubMed, China National Knowledge Infrastructure (CNKI), VIP, and Wanfang Databases were searched for randomized controlled trials (RCTs) on LC after PTGD in elder acute cholecystitis published from 1970 to July 2017. Two researchers selected RCTs, extracted data, and evaluated methodological quality independently, and RevMan 5.3 software was used for the meta-analysis. The chi-square test was used for heterogeneity analysis of RCTs included, and the funnel plots were used to evaluate publication bias.
Results:
A total of 9 RCTs with 1000 patients were included in this analysis. Compared with the direct LC Group, the PTGD Group has significant better effect in operative duration (minutes) [standard mean difference (SMD) = −1.37, 95% confidence interval (95% CI): −2.52 to −0.22, P = .02], the amount of intraoperative bleeding (mL) (SMD = −1.38, 95% CI: −2.11 to −0.65, P = .0002), conversion rate to laparotomy (%) [odds ratio (OR) = 0.16, 95% CI: 0.08 to 0.31, P < .00001], postoperative complication morbidity (%) (OR = 0.29, 95% CI: 0.17 to 0.51, P < .0001), and postoperative hospital stay (days) (SMD = −1.26, 95% CI: −1.94 to −0.59, P = .0003). The funnel plots were slightly asymmetric, which suggested the presence of publication bias.
Conclusion:
The PTGD before scheduled LC can effectively not only shorten operative duration, intraoperative bleeding less, and postoperative hospital stay but also decrease the rate to laparotomy and postoperative complication morbidity in elder acute cholecystitis, and it is recommended to be regarded as the preferred therapy of the elder patients.
Introduction
A
Materials and Methods
Search strategy
The Cochrane library, PubMed, China National Knowledge Infrastructure (CNKI), VIP, and Wanfang Databases were searched for RCTs on LC after PTGD in elder acute cholecystitis published from 1970 to July 2017. Tracing the references included in the literature to obtain relevant literature was not found in computer retrieval. Combination of key words included “PTGD,” “percutaneous transhepatic gallbladder drainage,” “laparoscopic cholecystectomy,” “acute cholecystitis,” and “randomized controlled trials.”
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) all patients were older than 60 years, regardless of gender, height, weight, and whether combined with other diseases; (2) all patients with preoperative diagnosis of acute cholecystitis were in accordance with the Tokyo guidelines, 6 2013, and no other major diseases affecting research; (3) the observation group received PTGD combined with LC therapy, the treatment of the control group for emergency LC patients, and the observation group that received PTGD had no severe complication during and after PTGD; and (4) the language form is Chinese or English, and the type of research is RCT, regardless of whether or not to use the double-blind method. Exclusion criteria were as follows: (1) non-RCT study; (2) combined with gallbladder polyps or chronic cholecystitis; (3) surgical methods were wrong or statistical methods were flawed; and (4) empirical summary or case reports or reviews.
Quality assessment and data extraction
The literature screening was completed by 2 researchers independently, through reading the subject, selecting the standard subject, and then reading the abstract and the full text. Hereafter, the 2 researchers cross-estimated the quality of literature according to the quality evaluation of RCTs' Jadad method, from random allocation, double-blind method setting, exit and loss to follow-up (score out of 5 points, < 2 for inferior quality literature, more than 3 points for high quality literature), and to evaluate the methodological quality of included literature refer to simple method recommended by Cochrane Review handbook. Discuss the literature on disagreement or ask other researcher to decide whether to incorporate it. The data extraction includes: (1) first author's name and publication time; (2) intervention measures and sample capacity; (3) specific treatment prescription and course of treatment; and (4) the evaluation index included operation duration (minutes), the amount of intraoperative bleeding (mL), conversion rate to laparotomy, postoperative hospital stay (days), and postoperative complication morbidity, including wound infection, pneumonia, pleural effusion, bile leakage, gallbladder effusion, and so on.
Statistical method
RevMan 5.3 provided by Cochrane collaboration was used for mate analysis, and heterogeneity among the study was analyzed by Chi-square test. If the difference between the heterogeneity among the studies was not statistically significant (I2 ≤ 50%, P > .05), the fixed effect model was used in analysis; if the difference between the heterogeneity among the studies was statistically significant (I 2 ≥ 50%, P < .05), the random effect model was used. For the dichotomous data, the combined effect sizes were evaluated using the odds ratio (OR) and 95% confidence interval (95% CI). For the continuous data, the combined effect sizes were evaluated using the standard mean difference (SMD) and 95% CI. Funnel plots were used to assess publication bias. Probability value of P < .05 was considered statistically significant.
Results
Literature search results
A total of 408 studies were included, and 128 studies among them were identified after excluding duplicates. By screening the titles and abstract, 91 studies were removed because they didn't meet the inclusion criteria. After reading the full text of the remaining 37 studies, 28 studies were removed based on study eligibility criteria, including (1) case reports or non-RCT; (2) open cholecystectomy; (3) general characteristics having significant differences; and (4) outcome evaluation indicators were incomplete. Finally, nine studies were included in this meta-analysis (Fig. 1),7–15 including 1000 patients, 476 patients in PTGD united LC groups and 524 patients in emergency LC groups. It contains 6 Chinese literatures and 3 English literatures. [Although some literature did not describe the blind method, the general characteristics of patients included in the study were described in detail. There were no significant differences in the general features, basic diseases, and examination indexes of all patients (P > .05), so incorporated].

Flowchart of identified studies. RCT, randomized controlled trial.
Characteristics and quality of studies
The quality of the selected literature was evaluated by the quality evaluation of RCTs' Jadad method. The Jadad scale consists of three elements as follows: random allocation, double-blind method setting, and exit and loss to follow-up; of these, 1–2 indicated that the test was of inferior quality, and 3–5 indicated that the test was of high quality. Details of the literature included are shown in Tables 1 and 2.
RCT, randomized controlled trial.
CG, control group; CL, conversion laparotomy; IB, intraoperative bleeding; NR, not reported; OD, operative duration; OG, observation group; PC, postoperative complications; PHS, postoperative hospital stay.
Meta-analysis results
Operation duration
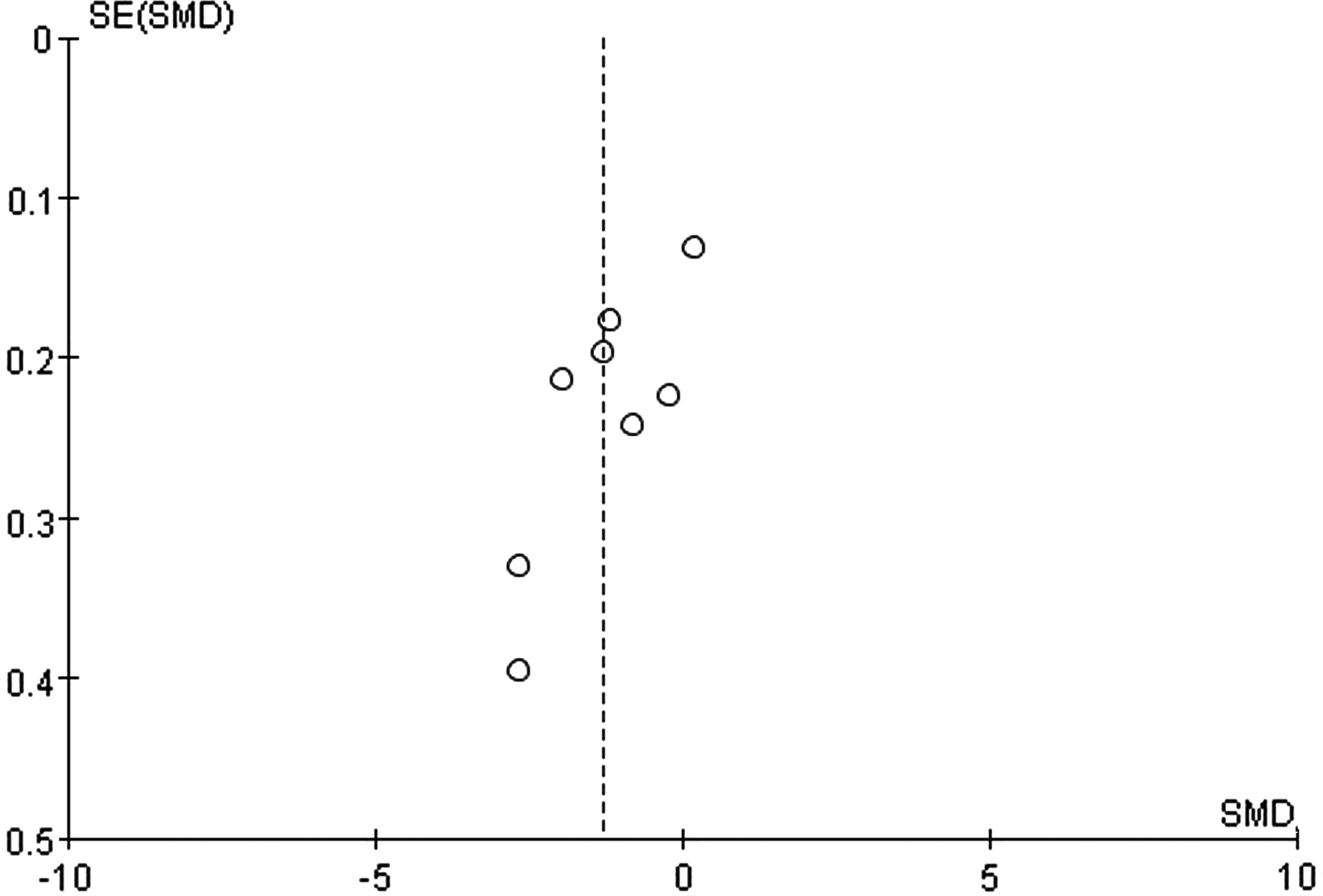
Among the six studies,7,9,11–14 a total of 803 patients were included, which reported the comparison of the time between PTGD combined with LC and emergency LC. Significant heterogeneity between these studies included in the manifest was observed (P < .00001, I2 = 98%). The reason may be surgical instruments or surgical experience or other factors, thus the random effects model was used in analysis. The results showed that the operation duration of the observation group was shorter compared with the control group, and the difference was statistically significant [SMD = −1.37, 95% CI (−2.52 to −0.22), Fig. 2]. The publication bias test showed that the symmetric of funnel plots was slightly worse (Fig. 3), and it identified that publication bias may be present.

Meta-analysis of the operative duration between the observation group and control group. 95% CI, 95% confidence interval; SD, standard deviation.

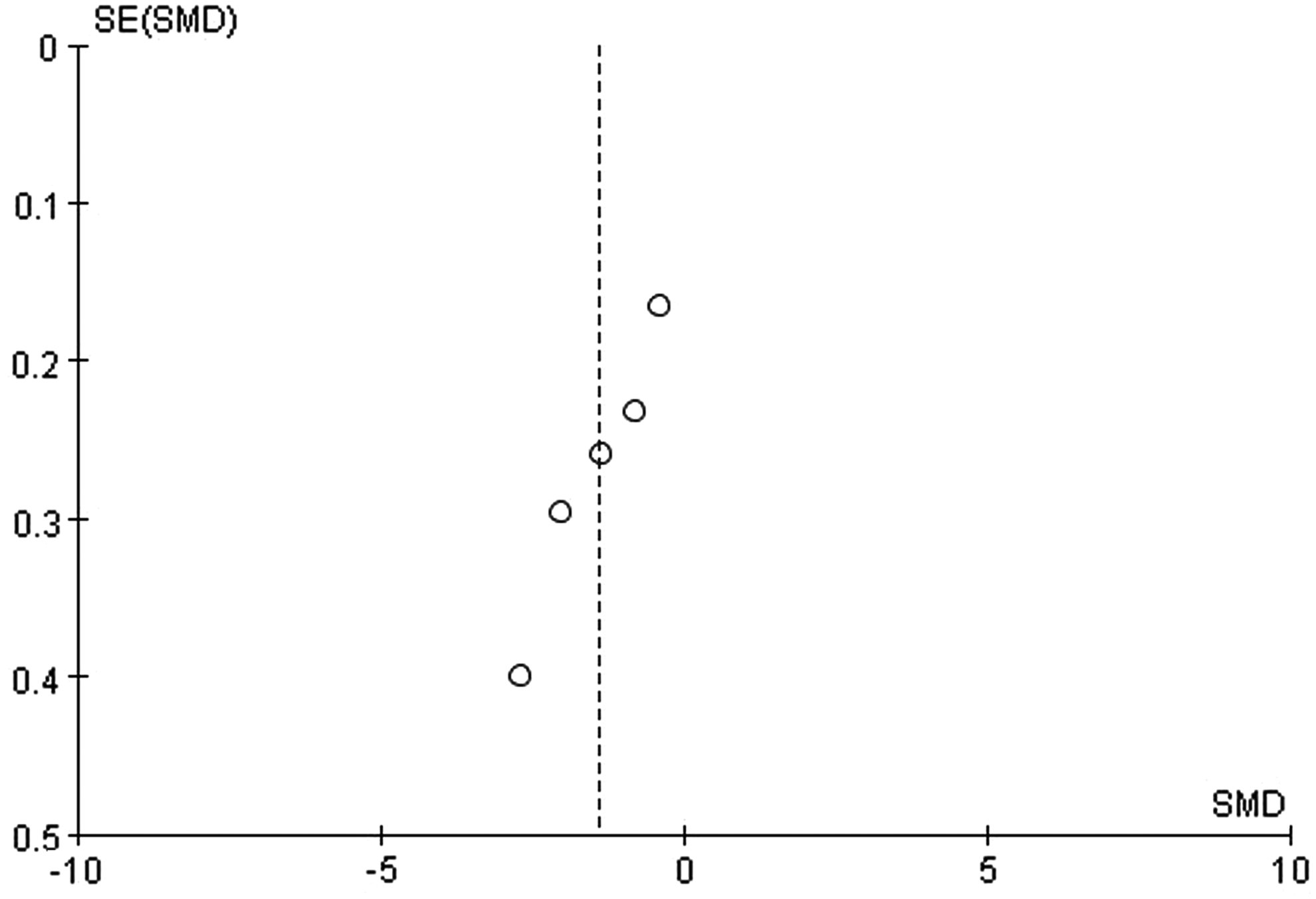
The funnel plots of the operation duration. SE, standard error; SMD, standard mean difference.
Conversion to laparotomy
Among the six studies,7,9,11–14 a total of 803 patients were included, which reported the comparison of the conversion rate to laparotomy between the observation group and the control group. There was no significant heterogeneity between these studies (P = .91, I2 = 0%), thus the fixed effects model was used in analysis. The results showed that the conversion rate to laparotomy in the observation group was lower than the control group, and the difference was statistically significant [OR = 0.16, 95% CI (0.08 to 0.31), Fig. 4]. The publication bias test showed that the symmetric of funnel plots was slightly worse (Fig. 5), and it identified that publication bias may be present.
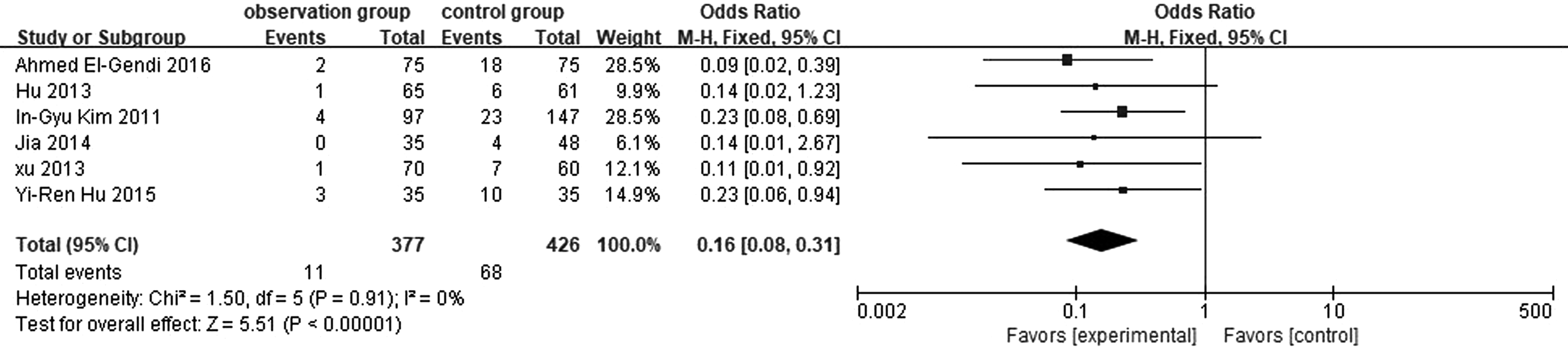
Meta-analysis of the conversion rate to laparotomy between the observation group and control group. 95% CI, 95% confidence interval.

The funnel plots of the conversion rate to laparotomy. OR, odds ratio; SE, standard error.
Intraoperative bleeding
Among the 5 studies,8,9,13–15 a total of 426 patients were included, reporting the comparison of the amount of intraoperative bleeding between the observation group and the control group. Significant heterogeneity between these studies included in the manifest was observed (P < .00001, I2 = 91%). The reason may be surgical instruments or surgical experience or other factors, thus the random effects model was used in analysis. The results showed that the amount of intraoperative bleeding in the observation group was lower than the control group, and the difference was statistically significant [SMD = −1.38, 95% CI (−2.11 to −0.65), Fig. 6]. The publication bias test showed that the symmetric of funnel plots was slightly worse (Fig. 7), and it identified that publication bias may be present.

Meta-analysis of the amount of intraoperative bleeding between the observation group and control group. 95% CI, 95% confidence interval; SD, standard deviation.
The funnel plots of the amount of intraoperative bleeding. SE, standard error; SMD, standard mean difference.
Postoperative complication morbidity
Among the eight studies,7–14 a total of 926 patients were included, which reported the comparison of postoperative complication morbidity between the observation group and the control group. There was no significant heterogeneity between these studies (P = .19, I2 = 30%), thus the fixed effect model was used in the analysis. The results showed that the complication morbidity in the observation group was lower than the control group, and the difference was statistically significant [OR = 0.29, 95% CI (0.17 to 0.51), Fig. 8]. The publication bias test showed that the symmetric of funnel plots was slightly worse (Fig. 9), and it identified that publication bias may be present.
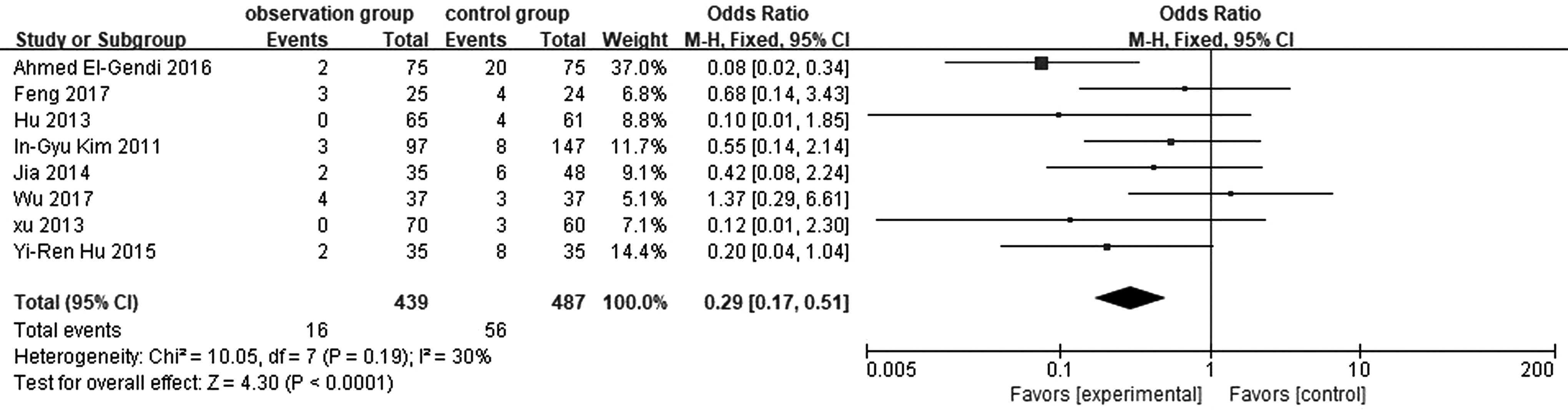
Meta-analysis of the postoperative complication morbidity between the observation group and control group. 95% CI, 95% confidence interval.
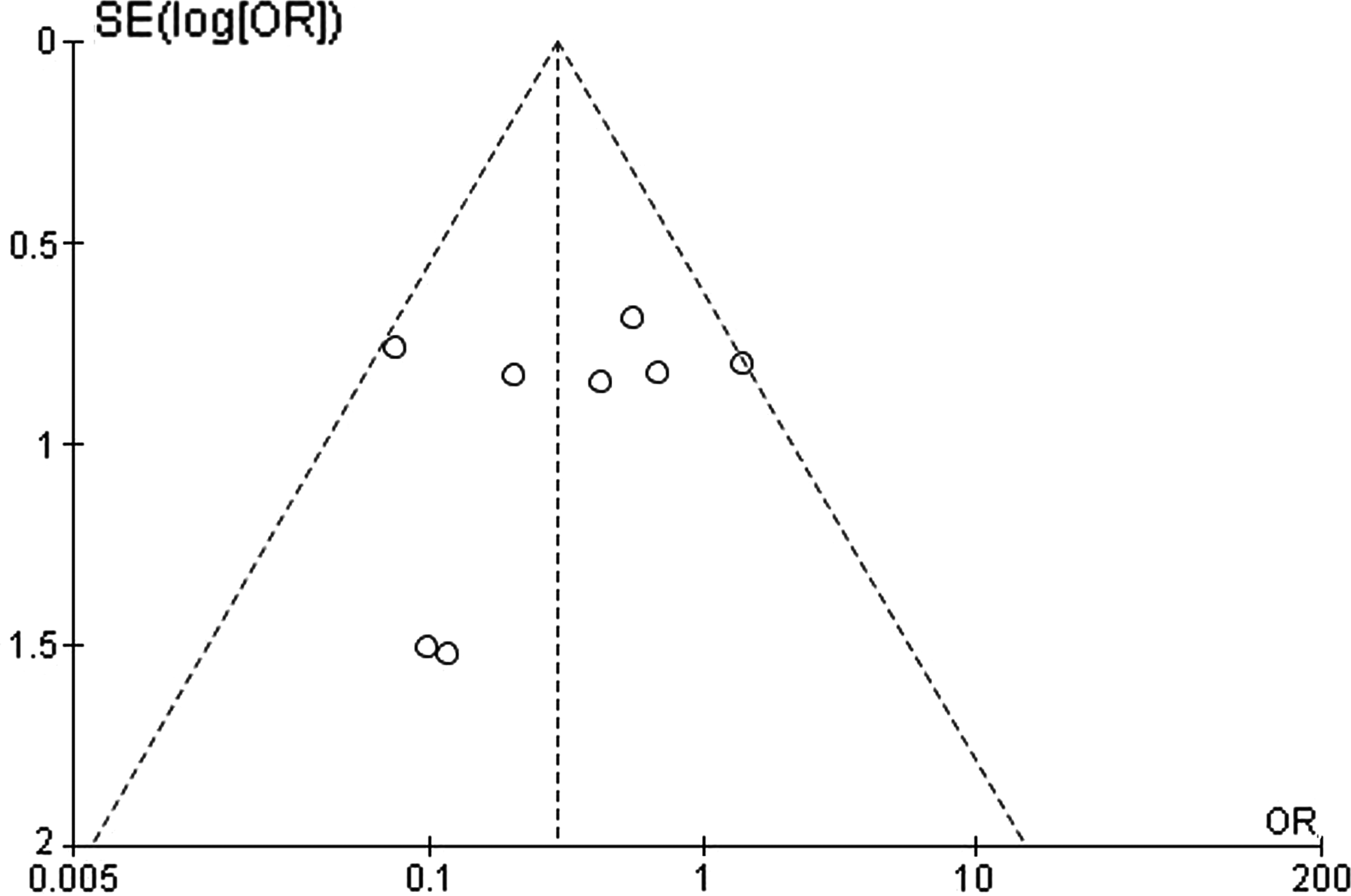
The funnel plots of the postoperative complication morbidity. OR, odds ratio; SE, standard error.
Postoperative hospital stay
Among the eight studies,7–14 a total of 926 patients were included, reporting the comparison of postoperative hospital stay between the observation group and the control group. Significant heterogeneity between these studies included in the manifest was observed (P < .00001, I2 = 95%). The reason why may be that the researchers had different evaluation standards for discharge, thus the random effects model was used in analysis. The results showed that the postoperative hospitalization time in the observation group was shorter than the control group, and the difference was statistically significant [SMD = −1.26, 95% CI (−1.94 to −0.59), Fig. 10]. The publication bias test showed that the symmetric of funnel plots was slightly worse (Fig. 11), and it identified that publication bias may be present.

Meta-analysis of the postoperative hospital stay between the observation group and control group. 95% CI, 95% confidence interval; SD, standard deviation.
The funnel plots of the postoperative hospital stay. SE, standard error; SMD, standard mean difference.
Discussion
Acute cholecystitis is an acute suppurative inflammation of the gallbladder caused by obstruction of the cystic duct and bacterial infection. It is a common surgical acute abdomen in clinic. Some studies indicated that more than 80% of patients with acute cholecystitis have gallstones and mainly affects the elderly. 16 Acute cholecystitis with gallstones is likely to develop into acute gangrenous cholecystitis or purulent inflammation, especially in the elderly population, which may be related to the elderly patients who are not sensitive to pain, lack of resistance to infection, poor compliance, and lack of attention. Most surgeons would suggest that conservative treatment of delayed surgery encountered this kind of patients and let them return to the hospital suffering from cholecystectomy in 6–8 weeks after symptomatic relief. In recent years, studies have shown that the complications, mortality, length of stay, and conversion rate to laparotomy of LC performed early in the disease are all the same as or better than delayed surgery. 17 Ohta et al. suggested that acute cholecystitis that occurred within 72 hours after emergency surgical treatment is safer and more reliable, 18 but the standard time of early LC has not yet been recognized. Meanwhile the onset time of many patients is usually more than 72 hours, which made the emergency surgery more difficult, more intraoperative blood loss, the higher rate of laparotomy, and the higher morbidity of postoperative complications, causing more pain and burden to patients. Thus, the choice of emergency surgery needs to weigh the pros and cons.
In 1980s, PTGD was used for the treatment of gallbladder empyema for the first time. 19 At present, PTGD has been widely used in the treatment of other serious diseases associated with acute cholecystitis to reduce the mortality rate of emergency cholecystectomy. The safety, effectiveness, and success rate of PTGD have reached a consensus. 3 Huang suggested that PTGD could not cure the cause, but it may effectively control acute inflammation for elderly patients. After waiting for symptomatic relief, combined with LC surgery, it may be a positive method to reduce postoperative complication diseases. 20 Studies had shown that PTGD combined with LC was able to quickly relieve gallbladder tension in acute cholecystitis, relieve inflammatory symptoms, and improve LC safety. 7 It has been proved to be of great value in the treatment of elderly patients with acute cholecystitis. Wu's recent research found that PTGD combined with LC treatment of acute cholecystitis with diabetes was safe and effective, which can significantly shorten the operation time, reduce intraoperative blood loss, and speed up patients with postoperative rehabilitation. 21
The results of this meta-analysis showed that the operation time of PTGD combined with LC group (the observation group) was shorter than direct LC group (the control group) [SMD = −1.37, 95% CI (−2.52 to −0.22)], and the difference was statistically significant (P = .02). The intraoperative blood loss of the observation group was less than the control group [SMD = −1.38, 95% CI (−2.11 to −0.65)], and the difference was statistically significant (P = .0002). The rate of conversion to laparotomy in the observation group (2.92%, 11/377) was lower than that in control group (15.96%, 68/426) [OR = 0.16, 95% CI (0.08 to 0.31)], and the difference was statistically significant (P < .00001). The complication morbidity in the observation group (3.64%, 16/439) was lower than the control group (11.50%, 56/487) [OR = 0.29, 95% CI (0.17 to 0.51)], and the difference was statistically significant (P < .0001). The postoperative hospitalization time in the observation group was shorter than the control group [SMD = −1.26, 95% CI (−1.94 to −0.59)], and the difference was statistically significant (P = .0003). However, some outcome indexes, such as the operation time, intraoperative blood loss, and postoperative hospitalization, were imprecise because of technical constraints and subjective factors' greater impact. Because the literature heterogeneity test had obvious heterogeneity, there may be some differences between the results and the theory, thus the significance of clinical guidance was limited. It requires more rigorous, large-scale, multicenter randomized controlled studies to verify.
Some limitations of this meta-analysis should also be taken into account. First, the quality of the literature is not too high, and the sample size was too small to conduct stratified analyses, which weakened the conclusions, especially in the analyses of intraoperative. As a result, the results of the analysis may be affected by publication bias. More studies need to be picked up to achieve a much more reliable conclusion. All studies did not mention economic issues, which may be a problem that has attracted the current medical workers. Not only the pain caused by the disease but also the cost of treatment should be considered. It requires more clinical researches to pay attention.
The timing of option of LC after PTGD is also a hot topic. Li reviewed 128 cases and suggested that PTGD treatment could reduce the risk of emergency surgery in elderly patients with acute calculous cholecystitis combined with severe heart and lung disease. It took about 16–60 days to relieve symptoms after PTGD. To receive surgery treatment as soon as possible after symptomatic relief could get better clinical results. It was meaningless to extend the PTGD tube time. 22 Inoue reviewed 77 cases and believed that although within 72 hours after PTGD early LC may be safe, cholecystectomy should be arranged after 216 hours. 23 Deng et al. analyzed the difference between selective operation at 1 week and 1 month after PTGD and concluded that selective operation was more reasonable at 1 month after PTGD. 3 Yi suggested that selective LC arranged at 2–4 months after PTGD could reduce surgical damage and reduce the morbidity of complications, which will help patients recover rapidly and reduce the patient's pain. It was worthy of clinical use. 24 Even so, optimal timing of cholecystectomy after PTGD also needs more clinical studies to verify to guide the clinical treatment more accurately.
Conclusion
In conclusion, our findings demonstrate that the PTGD before scheduled LC can effectively not only shorten operative duration, intraoperative bleeding, and postoperative hospital stay but also decrease the rate of conversion to laparotomy and postoperative complication morbidity in elder acute cholecystitis. It is recommended to perform this therapy for the elder acute cholecystitis patients.
Footnotes
Acknowledgments
The authors thank Mr. Zhong and Pro. Gong for reviewing an early draft of this article and giving valuable comments. We also appreciate the support from the National Science Foundation of China (No.81470899) and the Natural Science Foundation of Chongqing (No.cstc2012jjA10090).
Disclosure Statement
No competing financial interests exist.