
Abstract
Abstract
Background:
Super obese patients remain a challenge for management because of large liver size resulting in decreased work space and associated comorbidities.
Objectives:
To study outcomes in super obese patients undergoing Laparoscopic sleeve gastrectomy (LSG).
Methods:
Retrospective data of 123 patients undergoing LSG from January 2008 to March 2015 were analyzed prospectively.
Results:
Mean age and body mass index (BMI) of 123 patients (± 2 standard deviation [SD]) were 39.9 ± 23.3 years and 55.6 ± 10.54 kg/m2, respectively. Mean percentage excess weight loss (%EWL) (± 2 SD) at 1, 3, 5, and 7 years was 63% ± 36.7%, 62.3% ± 29.0%, 56.5% ± 35.8%, and 58.6% ± 40.3%, respectively. The preoperative BMI correlated with %EWL at 1 year (r2 = 0.0397, P = .044). Staple line leak, bleeding, deep venous thrombosis, and 30-day mortality occurred in 1.6%, 0%, 0.8%, and 0% of the patients, respectively. Stricture formation and new onset gastroesophageal reflux disease (GERD) occurred in 0.8% patients each. Of the diabetic patients, 72.2% had remission and the rest required decreased dosage of oral hypoglycemic medications. Hypertension, obstructive sleep apnea, and GERD improved in 68.2%, 100%, and 25% of the patients, respectively. However, 25% of patients had worsening in GERD symptoms.
Conclusions:
Super obese patients undergoing LSG as the primary procedure have reasonable weight loss of 62% and 56% at 3 and 5 years, respectively, with significant resolution of comorbidities.
Introduction
L
Materials and Methods
Data of all the super obese patients undergoing LSG from January 2008 to March 2015 and completed their at least 1 year of follow-up were collected. The analysis was done prospectively on retrospectively collected data. All patients undergoing LSG had body mass index (BMI) of more than 50. All the procedures were performed by a single surgeon according to a standardized protocol. The patients were kept on a liquid diet (very low-calorie diet) before the surgery to reduce the liver size.
Surgical procedure
Cefuroxime was used as a prophylactic antibiotic. Pneumatic compression devices were used to prevent deep venous thrombosis (DVT) preoperatively, as well as 2 weeks postoperatively. Two 12 mm and two 5 mm were used for the procedure. Greater omentum was divided at a point 4 cm from the pylorus to the angle of His. The sleeve was created over 36 French gastric tube using a stapler (tri cartridge Medtronic). A leak test was done using methylene blue to check for the suture line of the newly created sleeve.
Weight loss
Weight was recorded in the outpatient department and at admission after liquid diet. Percentage excess weight loss (%EWL) was recorded as per Deitel et al. 5 %EWL of < 50% was considered a failure of surgery as per Reinhold. 6
Comorbidity outcome
Diabetes mellitus
Diabetes mellitus (DM) was defined as HbA1c > 6.5 or fasting blood sugar (FBS) >126 mg/dL. Remission was considered if the patient was euglycemic (FBS <100) without insulin or oral hypoglycemic agents, and improvement was defined by a decrease in antidiabetic medications. HbA1c could not be used to define remission as it was not available for all the patients.
Hypertension
Hypertension was defined as blood pressure >140/90 mm Hg. Remission was defined if the patient had normal blood pressure (≤120/80) without any antihypertensive medications, and improvement was considered if the patient required a decrease in dosage of antihypertensive medications.
Obstructive sleep apnea
Obstructive sleep apnea (OSA) was defined as apnea–hypopnea index more than 14. Polysomnography could not be done for all patients so remission was not defined in the study. An improvement was considered if the patient had a decrease in symptoms of OSA or did not require continuous airway positive pressure (CPAP) postoperatively.
Hypothyroidism
Hypothyroidism was considered in patients taking thyroxine or with abnormal thyroid function tests (TFT) before surgery. Remission was taken if the patient did not require thyroxine with normal TFT. An improvement was considered if the patient had a decrease in dose of thyroxine.
Gastroesophageal reflux disease
Gastroesophageal reflux disease (GERD) severity symptom (GERD-SS) questionnaire 7 was used to assess the presence of GERD with GERD-SS score >4 or regular use of proton pump inhibitors (PPIs) being defined as GERD. Remission was considered if the patient had no symptoms of GERD without the use of PPI. An improvement was considered if the patient required a decrease in dose of PPI or decrease in symptoms. New onset GERD was defined if the patient developed symptoms of reflux postoperatively or required to start PPIs.
Statistical analysis
The analysis was done using SPSS 20.0. Continuous variables were presented as mean with standard deviation. Continuous variables were compared using nonparametric Mann-Whitney U test and categorical variables using Chi Square test. The correlation was done using Spearman Rank Correlation Coefficient. Statistical significance was considered for P value <.05.
Results
One hundred twenty-three super obese patients underwent LSG as the primary procedure from 2008 to 2015 and completed at least 1 year follow-up in 2016. As shown in Table 1, mean age (± 2 standard deviation [SD]) was 39.9 ± 23.3 years, and the mean weight (± 2 SD) was 142.8 ± 45.0 kg, and the mean BMI (± 2 SD) was 55.6 ± 10.54 kg/m2. Percentage of females was 70.7%.
BMI, body mass index; GERD, gastroesophageal reflux disease; OSAS, obstructive sleep apnea syndrome; SD, standard deviation.
Percentage of follow-up of patients is shown in Figure 1.
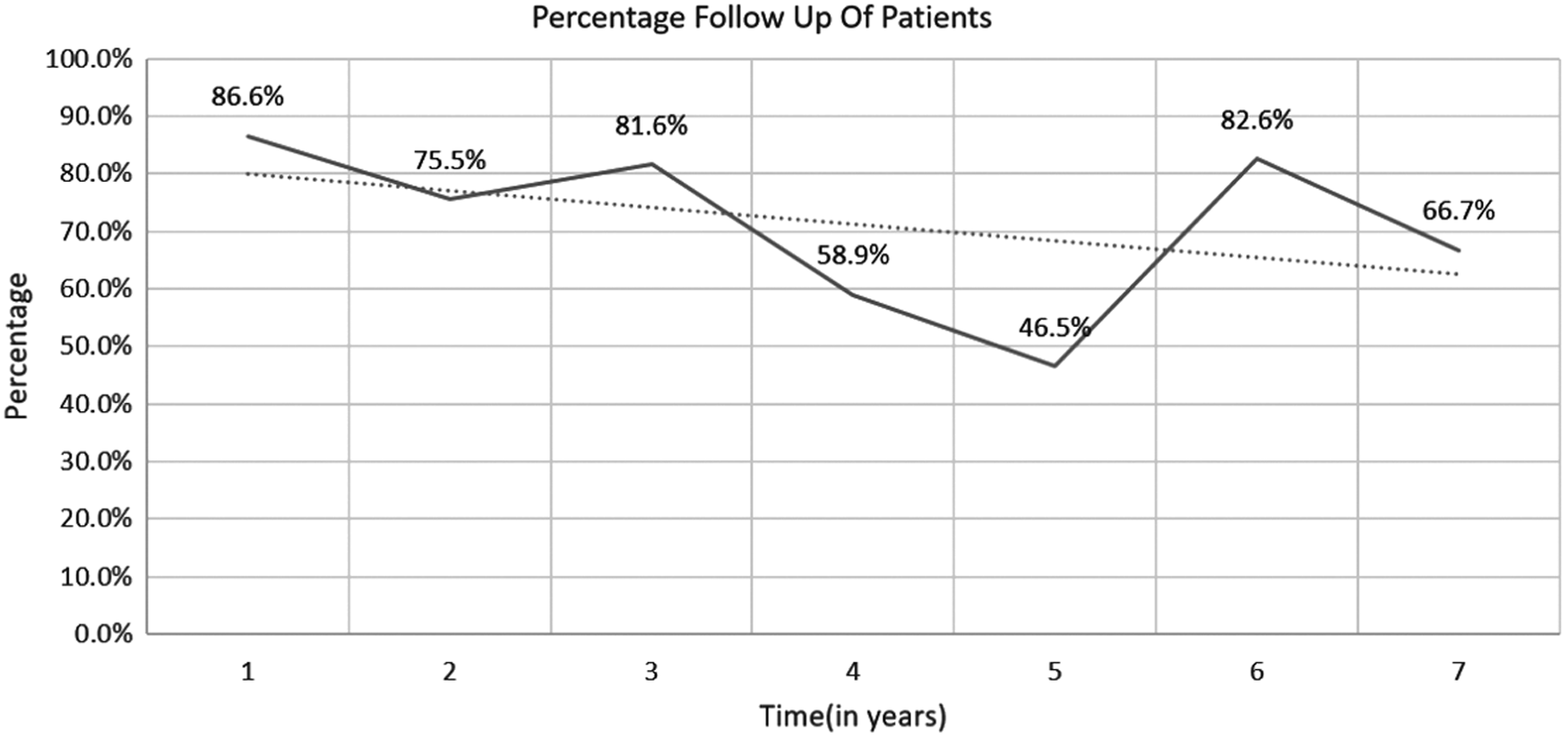
Percentage of follow-up of patients. The solid line denotes actual percentage patient follow-up. The dotted line denotes line of best fit (trend line).
Impact on weight loss
As shown in Table 2, mean EWL% at 1, 2, 3, 4, 5, 6, and 7 years was 63% ± 36.7%, 66.6% ± 42.9%, 62.3% ± 29.0%, 60.9% ± 30.9%, 56.5% ± 35.8%, 55.4% ± 38.7%, and 58.6% ± 40.3%, respectively, with P ≤ .001 for all.
%EWL, percentage excess weight loss.
The weight on liquid diet decreased from a mean of 142.82 kg to a mean of 137.72 kg as shown in the Figure 2.
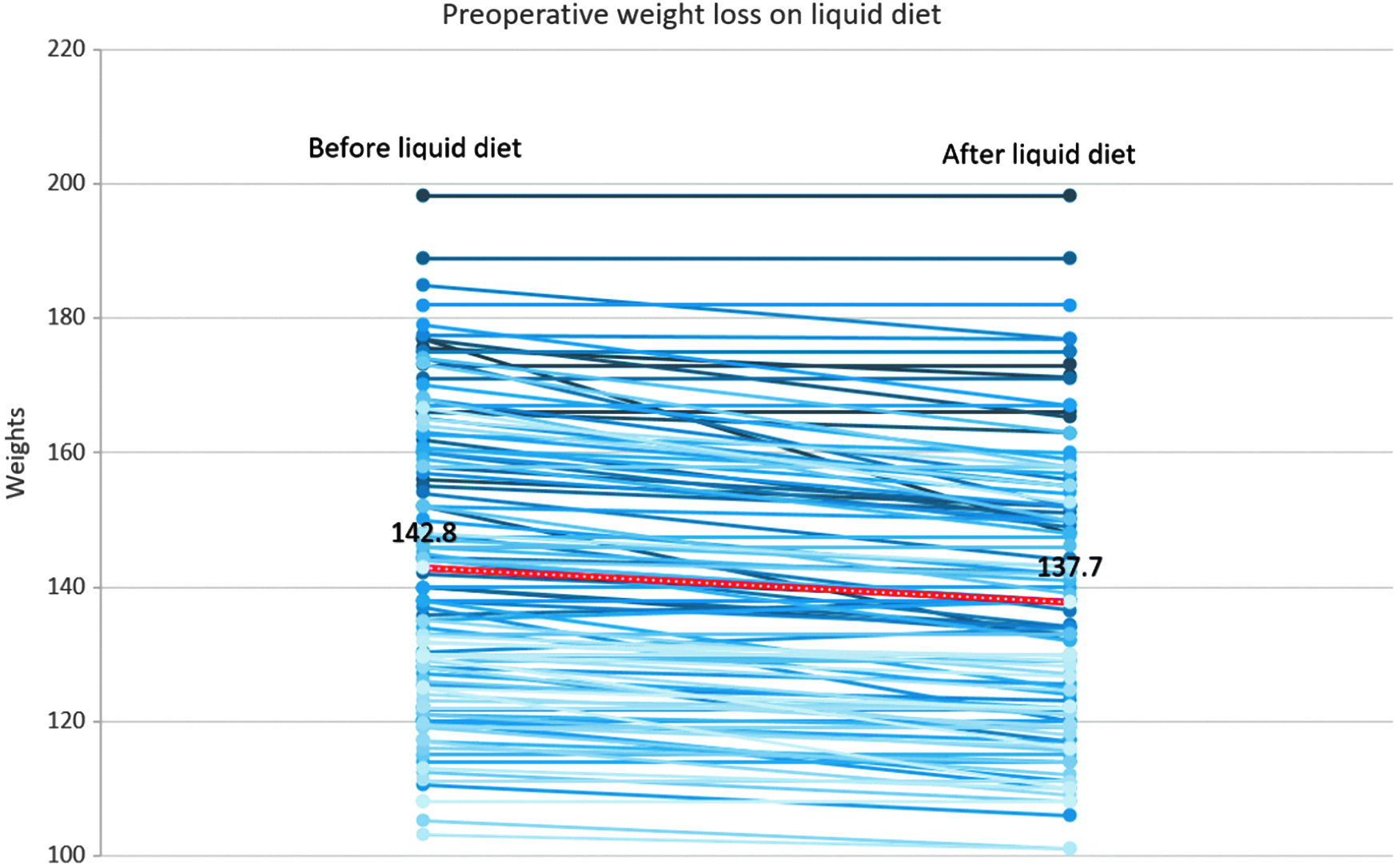
Preoperative weight loss on liquid diet. The blues lines indicate individual patient's preoperative weight loss. The red line indicates mean preoperative weight loss.
There was a significant correlation between preoperative BMI and %EWL at 1 year (r2 = 0.0397, P = .044) using multivariate regression analysis Table 3, Figure 3.

Correlation of excess weight loss at 1 year with body mass index.
Impact on comorbidities
The impact on comorbidities is summarized in Table 4.
OSA, obstructive sleep apnea.
Eighteen (14.6%) patients had DM preoperatively out of which 72.2% showed remission, while the rest showed improvement at 1 year of follow-up. Thirteen patients were available for following at 3 years of which 76.9% were in remission and rest had improvement. Twenty-two (17.8%) had hypertension preoperatively out of which 36.4% patients showed remission, 31.8% had improvement, and 31.8% had no change in their hypertensive status. Fourteen (11.38%) patients had OSA of whom 9 required CPAP therapy. Thirteen patients came at 1 year for follow-up and all showed remission in symptoms of OSA. None of the patients required CPAP postoperatively. Nineteen (15.4%) patients suffered from hypothyroidism. At 1 year of follow-up, 5.26% had remission, 68.4% had improvement, and rest had no change in their hypothyroid status. Four patients suffered from GERD of which GERD resolved in 1 patient, improved in another, and there was no change in rest of the 2 patients.
In our study 1 patient required redo surgery (gastric bypass) due to failure of the sleeve. One patient required mini gastric bypass (MGB) due to weight regain and 1 patient underwent re-sleeve and MGB due to weight regain post LSG. One patient required redo surgery due to the development of severe GERD symptoms.
Complications
Staple line leak, bleeding, DVT, and 30-day mortality occurred in 2 (1.6%), 0%, 1 (0.8%), and 0% of the patients, respectively. Stricture formation and new onset GERD occurred in 0.8% patients each.
Discussion
LSG has been an effective weight loss surgical option for patients with morbid obesity. 8 LSG has also been found to be effective as a primary weight loss surgical option for super obese patients with significant resolution of comorbidities in most of those patients. 9
In our study, we recruited 123 super obese patients with the mean age (± 2 SD) 39.9 ± 23.3 years and BMI (± 2 SD) of 55.6 ± 10.54 kg/m2, respectively. One hundred three (83.7%) patients in our study completed 1 year follow-up, 62 (50.4%) patients completed 3 years follow-up, and 20 (16.2%) patients completed their 5 years follow-up, while 7 (5.69%) patients completed 7 years follow-up. One to 3-year follow-up rates across other studies ranged from 73% to 100%.9–11
%EWL is the most important factor which equates to the success of bariatric surgery. In our study, mean EWL% at 1 year was 63% ± 36.7%, P < .001 and at 3 years was 62.3% ± 29.0%, P < .001 which declined to 56.5% ± 35.8%, P < .001 at 5 years and 58.6% ± 40.3%, P = .001 at 7 years. Our results of weight loss have been similar with results of other studies. A study done by Eid et al. on 74 super obese patients showed %EWL of 52%, 43%, and 46% at 72, 84, and 96 months, respectively. 10 Pourcher et al. in their study on 62 super obese patients showed median %EWL of 69.7% at 1 year of follow-up. 12 In a study done by Gagner et al. on 63 super obese patients, it was seen that mean BMI decreased from 68 to 58 over a period of 6 months following LSG; however, 43 patients required duodenal switch due to weight gain. 13 In a study on 71 patients undergoing LSG, Eisenberg et al. showed EWL of 61% at 22 months on an average. There was no significant difference in weight loss among morbid obese and super obese population. 9 Catheline in their study on 33 super obese patients showed EWL of 51% at a mean follow-up of 2 years. 11 Catheline et al. in a case series of 4 super obese patients with average BMI of 65 showed that mean BMI decreased by 16.3 in 6 months follow-up period following LSG. 14
Some studies have compared weight loss following LSG and other procedures. Madhok et al. compared weight loss following LSG and MGB in super obese patients. They found higher weight loss in MGB group compared to LSG group. 15 Zerrweck et al. compared weight loss between 32 super obese patients undergoing laparoscopic Roux-en-Y gastric bypass (LRYGB) and 45 super obese patients undergoing LSG. It was seen that EWL in LRYGB group was 51%, 56%, and 63% at 6, 9, and 12 months, while EWL in LSG group was 40%, 45%, and 43% at 6, 9, and 12 months, respectively. 16 Gonzalez-Heredia et al. also compared weight loss following LRYGB and LSG in super obese patients and found significantly (P < .05) more %EWL in LRYGB group compared to LSG group. 17 Serrano et al. in a study found EWL >30% in 94.5% and 100% of the patients undergoing LRYGB and LSG, respectively. 18 Although MGB and LRYGB have been found to be associated with more weight loss compared to LSG still LSG results in significant %EWL in super obese patients.
As shown in graph 1 the preoperative BMI in our study significantly correlated with %EWL at 1 year (r2 = 0.0397, P < .05). Correlation of preoperative BMI with %EWL at 3 years is shown in graph 2. Dakour Aridi et al. also showed a similar relationship between preoperative BMI and %EWL. 19 Other studies also have shown a similar relation.20–22
In our study, the failure rate increased from 22.3% at 1 year to 29% at 3 years. One patient in our study required second-stage gastric bypass due to inadequate weight loss. Two patients had to undergo MGB due to weight regain. This regain in weight may be due to neo fundus formation and increase in activity and number of ghrelin producing cells post-LSG. 23 It could also be due to improper dietary practices and lack of aerobic exercise. 24
DM resolved in 72.2% of our patients while improved in the rest (P < .001). Bariatric surgery leads to increased gastric emptying resulting in increased GLP-1 mediated insulin secretion which can result in improved glycemic control. 25
Only a few studies are available which have studied the impact of LSG on comorbidities in super obese patients. A study done by Eid et al. showed that DM resolved or improved in 77% of the patients. 10 Pourcher et al. showed remission of DM in 60% of patients after LSG. 12 Eisenberg et al. in a study found 56% resolution of DM in super obese patients undergoing LSG. 9 Zerrweck et al. found 86.6% resolution of DM in super obese patients undergoing LRYGB and LSG. 16 Serrano et al. showed that HbA1c levels decreased by 10% and 9%, respectively, in patients undergoing LSG and LRYGB, respectively, from a mean of 6.2. 18
Hypertension resolved in 36.4% of the patients, while improved in 31.8% of the patients at 1 year of follow-up (P < .001). There was no change in hypertension in 31.8% of the patients. Eid et al. found resolution or improvement of hypertension in 75% of the super obese patients. 10 A study done by Pourcher et al. showed resolution of hypertension in 65% of the patients. 12 Eisenberg et al. found 56% improvement in hypertension in super obese patients following LSG. 9 The effect on hypertension could be explained by a decrease in renin angiotensin aldosterone activity and decrease in the intra-abdominal pressure secondary to weight loss after surgery. 26
In our study we found remission in OSA symptoms in 100% (P < .001) of the patients. Nine patients required CPAP preoperatively; however, none of the patients required CPAP postoperatively at 1 year of follow-up. Eid et al. found resolution of OSA in 71% of the patients while Eisenberg et al. found resolution in 46.4% of the patients.9,10 All the bariatric procedures result in improvement of OSA symptoms in more than 75% of the patients. 27
In our study hypothyroid resolved or improved in 73.7% of the patients, while the rest of the patients had no change. To the best of our knowledge, there is no study evaluating the effect of LSG on hypothyroidism in super obese patients. However, Ruiz-Tovar et al. and a study from our center showed a decrease in TSH levels and decrease in thyroxine requirement after surgery in morbidly obese patients.28,29 The effect could be due to a decrease in hormone resistance following weight loss. 29
In our study, we had staple line leak, bleeding, DVT, and 30-day mortality in 2 (1.6%), 0%, 1 (0.8%), and 0% of the patients, respectively. Stricture formation and new onset GERD occurred in 1 (0.8%) patient each. None of the patients had port site hernia. Eid et al. reported a leak in 1 (1.3%) patient and stricture formation in 3 (4%) of the patients. 10 Pourcher et al. reported bleed in 2 (3.2%) patients, 12 while Eisenberg et al. reported bleed in 1.4% and leak in 2.8% of the patients, respectively. 9 Catheline et al. reported port site hernia in 2 (7%) of the patients.
In our study we found that GERD resolved in 25% patients, improved in 25% of the patients, while 50% of the patients had no change. One patient required redo surgery for severe reflux symptoms. However, the results were not statistically significant (P > .05). Eisenberg et al. showed that GERD improved in 25% of the patients, worsened in 17%, and did not change in 58% of the patients. 9 Eid et al. reported new onset GERD in 10.8% of the patients, while 31% patients showed resolution of symptoms. 10 The impact of LSG on GERD is still not well understood. Factors which may lead to improvement include faster gastric emptying, decreased intra-abdominal pressure secondary to weight loss. GERD could also be exacerbated due to translation in gastroesophageal junction or presence of concomitant hiatal hernia. 30
Strengths of the study are that it is the first study in Indian population regarding the impact of LSG on weight loss and resolution of comorbidities in super obese patients as a primary procedure. All the procedures were performed by a single surgeon using a standardized technique. We also had a reasonable midterm follow-up of the patients.
Limitations include poor follow-up over a long term. The procedure has very few long-term morbidities and this may result in avoidance for follow-up in patients especially who come from distant areas. Impact on comorbidities could not be optimally standardized as HbA1c was not available for all patients and polysomnography could not be done for all the patients.
Conclusion
Super obese patients undergoing LSG as the primary procedure have a reasonable weight loss of 62% and 56% at 3 and 5 years, respectively, with significant resolution of comorbidities.
Footnotes
Acknowledgment
This is to thank Mrs. Rachna Chaudhary, bariatric surgery coordinator, for providing the technical support in fulfillment of this project.
Disclosure Statement
No competing financial interests exist.