
Abstract
Abstract
Background:
The role of laparoscopy for the management of various types of postgastrectomy complications has not yet been well studied. We describe laparoscopic management of postgastrectomy complications and present a comparison between laparoscopy and other modalities in terms of basic characteristics and postreoperation clinical course.
Materials and Methods:
We studied 82 patients with postgastrectomy complications (Clavien–Dindo grade ≥IIIa) at a single institution between April 2009 and November 2016. We excluded 15 patients with pulmonary, wound-related, and/or ambiguous complications and eventually studied 67 patients who were divided into nonoperative intervention (NI), laparoscopic reoperation (LR), and open reoperation (OR) groups. Clinicopathological characteristics and surgical outcomes were compared.
Results:
Among the 67 patients studied, 31, 21, and 15 belonged to the NI, LR, and OR groups, respectively. Complications included bleeding in 29, leakage in 26, intestinal obstruction in 6, and intra-abdominal abscesses in 6 patients. Among the 21 patients in the LR group, bleeding was reported in 11, leakage in 5, intestinal obstruction in 3, and intra-abdominal abscesses in 2 patients. No significant differences were observed between the groups in terms of clinicopathological characteristics. Regarding surgical outcomes, the NI and LR groups required a mean of 11 days before discharge—a period that was significantly shorter than that required by the OR group (20.5 ± 14.3 days). All patients belonging to the LR group were successfully treated and discharged 11.3 ± 6.0 days after reoperation.
Conclusions:
Laparoscopic management of postgastrectomy complications is a safe and effective procedure primarily because it is associated with a smaller incision, more rapid recovery, and shorter length of hospitalization than that associated with an open laparotomy.
Introduction
B
A major postoperative complication is usually defined as a situation when additional invasive treatment is required to resolve a difficult/complex problem that has developed. Following technological developments in endoscopic, ultrasonographic, and angiographic techniques and devices, interventional treatment is now the first choice for the management of postoperative complications because it can avoid general anesthesia. However, in patients presenting with postoperative complications needing reoperation, an open laparotomy has been the generally accepted approach. A reoperation procedure requires extreme caution and close evaluation to determine the presence and extent of postoperative adhesions, ileus, tissue friability, and wound contamination. An open laparotomy scores over a laparoscopy in that it provides a wider operative field and is therefore able to better manage complications in terms of adhesions and ileus. However, additional tissue damage and wound contamination could be primary concerns associated with a relaparotomy. A laparoscopy scores over an open reoperation (OR) owing to potential advantages: (1) fewer wound-related complications and (2) rapid access into the intra-abdominal cavity, which can facilitate early detection of lesions/sites requiring attention and help in quick decision-making in instances of bleeding or intestinal obstruction. However, laparoscopic reoperation (LR) could be dangerous in the presence of adhesions at the previous incision site, which can cause bowel injury during the insertion of the first trocar. Thus, LR has not been well established due to safety issues.
We aimed to elucidate the feasibility and safety of a LR following gastrectomy for the management of gastric cancer. We describe in detail our experiences regarding the laparoscopic management of postgastrectomy complications using explanatory figures and additionally present a comparison between this procedure and other management modalities in terms of basic characteristics and the postreoperation clinical course.
Materials and Methods
Between March 2009 and November 2016, 731 gastric cancer surgeries were performed at Yeouido St. Mary's Hospital in Korea. Among these, 82 patients who developed a postgastrectomy complication with a Clavien–Dindo grade ≥ IIIa were included in our study. Among these 82 patients, except 8 patients with pulmonary, 2 with wound-related, and 5 with other ambiguous complications, the remaining 67 patients were categorized as patients with bleeding, leakage, obstruction, or intra-abdominal abscess. Patients were divided into nonoperative intervention (NI, n = 31), LR (n = 21), and OR (n = 15) groups, and clinicopathological characteristics, surgical outcomes, and clinical course were subsequently compared. We compared the surgery-to-event period, surgery-to-intervention or reoperation period, and recovery period. Postrecovery period was defined as the duration between the day of intervention or reoperation and discharge.
Definitions and selection of the management strategy
We present definitions for the management of each type of complication. A video clip illustrating each type of complication will be displayed.
NI: Any invasive treatment performed without using general anesthesia such as endoscopy, percutaneous drainage, and/or angiography.
LR: Reoperation that was successfully performed using only a laparoscopic approach.
OR: Reoperation that required an open laparostomy to safely complete the procedure, regardless of the initial reoperation approach used.
The type of management selected was decided by a single surgeon (Dr. Wook Kim). In patients presenting with intraluminal bleeding, endoscopic intervention was the first-choice treatment. Extraluminal bleeding was typically managed via a laparoscopic approach initially if the patient's vital signs were stable. Angiography-guided coil embolization was selected in patients in whom an angiographically accessible vessel showed a definite focus of extravasation. Open conversion was chosen in patients with massive uncontrollable bleeding associated with laparoscopy. In those with anastomotic or duodenal stump leakage, ultrasonography-guided percutaneous drainage was the preferred treatment. However, laparoscopy was performed in patients in whom intervention was impossible or peritonitis was observed. Laparoscopy was the preferred strategy in patients with intestinal obstruction and an intra-abdominal abscess. However, reoperation for an intra-abdominal abscess was performed when interventional drainage was impossible or diffuse peritoneal irritation signs were observed.
Statistical analysis
Patients were divided into three groups. Continuous variables were presented as mean ± standard deviation and compared using analysis of variance. Nominal variables were analyzed using the Fisher's exact test.
Results
Baseline clinicopathological characteristics
After excluding 15 patients, 67 patients were included in our study. Among these, complications included bleeding in 29, leakage in 26, obstruction in 6, and an intra-abdominal abscess in 6 patients. The groups did not significantly differ in terms of age, sex, American Society of Anesthesiologists score, resection type, and the extent of lymph node dissection. Furthermore, no differences were observed in the proportion of pathological T and N stages (Table 1).
ASA, American society of anesthesiologists score; BMI, body mass index; DG, distal gastrectomy; EBL, estimated blood loss; LR, laparoscopic reoperation; NI, nonoperative intervention; OR, open reoperation; PG, proximal gastrectomy; TG, total gastrectomy.
The proportion of initial surgeries that were performed using the laparoscopic approach were 80.6% and 95.2% in the NI and LR groups, respectively, and a significantly lower number of patients underwent the laparoscopic approach initially in the OR group. Estimated blood loss was significantly higher in the OR group than that in the other groups (NI versus LR versus OR = 216 ± 253 mL versus 288 ± 195 mL versus 531 ± 490 mL, respectively, P = .009). Regarding the extent of resection, although there was no significant difference between the groups, a total gastrectomy was performed in 40% of the patients in the OR group (Table 1).
Types of complications
There was no significant difference in the proportion of types of complications. In the LR group, complications included bleeding (n = 11), leakage (n = 5), intestinal obstruction (n = 3), and an intra-abdominal abscess (n = 2). In the NI group, complications included bleeding (n = 11), leakage (n = 15), intestinal obstruction (n = 1), and an intra-abdominal abscess (n = 4). In the OR group, complications included bleeding (n = 7), leakage (n = 5), and intestinal obstruction (n = 3) (Table 2). Details regarding complications are provided in Table 3.
EBL, estimated blood loss; LOS, length of stay; NI, nonoperative intervention; LR, laparoscopic reoperation; OR, open reoperation.
Other includes ileocolic anastomosis in LR and Remnant stomach perforation in OR.
EJ, esophagojejunostomy; LR, laparoscopic reoperation; NI, nonoperative intervention; OR, open reoperation.
Bleeding observed in all 11 patients in the NI group was of the intraluminal type, and was managed using endoscopic treatment. Endoscopy failed to control bleeding in one patient with intraluminal bleeding, which necessitated laparoscopic reinforcement sutures along the artificial lesser curvature. Bleeding observed in 10 patients in the LR group included oozing from the remnant stomach or anastomotic staple line (n = 5), bleeding from the sites of lymph node dissection (n = 3), and bleeding from the jejunal mesentery (n = 2) following a total gastrectomy. Figure 1 shows laparoscopic hematoma evacuation and bleeding control in the area of retroperitoneal lymph node dissection.
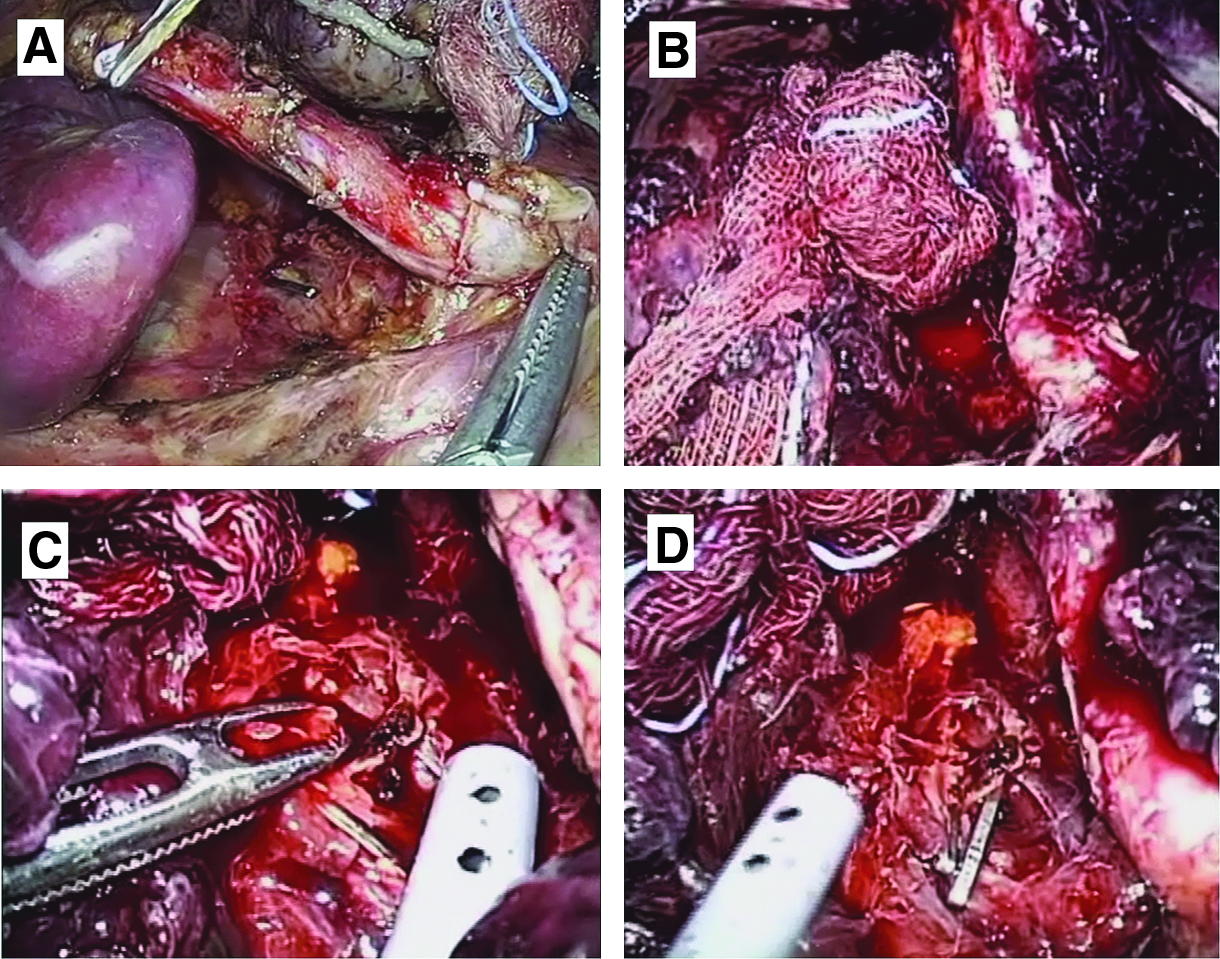
Laparoscopic bleeding control following laparoscopic distal gastrectomy.
Regarding postoperative leakage, four patients demonstrated duodenal stump leakage, and one patient demonstrated ileocolic anastomotic leakage at the site of a right hemicolectomy in the LR group. Among the four patients with duodenal stump leakage, three underwent laparoscopic Foley catheter duodenostomy insertion and drainage. A metal clip was used in one patient to seal the leakage site (needle injury) at the duodenal stump. Laparoscopic Foley catheter duodenostomy was performed using a Foley catheter of an appropriate size to fit into the defect at the site of the duodenal stump leakage (Fig. 2).

Laparoscopic Foley duodenostomy for managing duodenal stump leakage with peritonitis.
Endoscopic stent insertion was performed in one patient who developed an esophagojejunostomy obstruction secondary to kinking. All patients in the LR group who presented with obstruction demonstrated small bowel adhesions secondary to formation of an adhesive band. Laparoscopic adhesiolysis was safely performed in only those patients in whom the small bowel was not significantly dilated and therefore did not interfere with the laparoscopic procedure (Fig. 3).
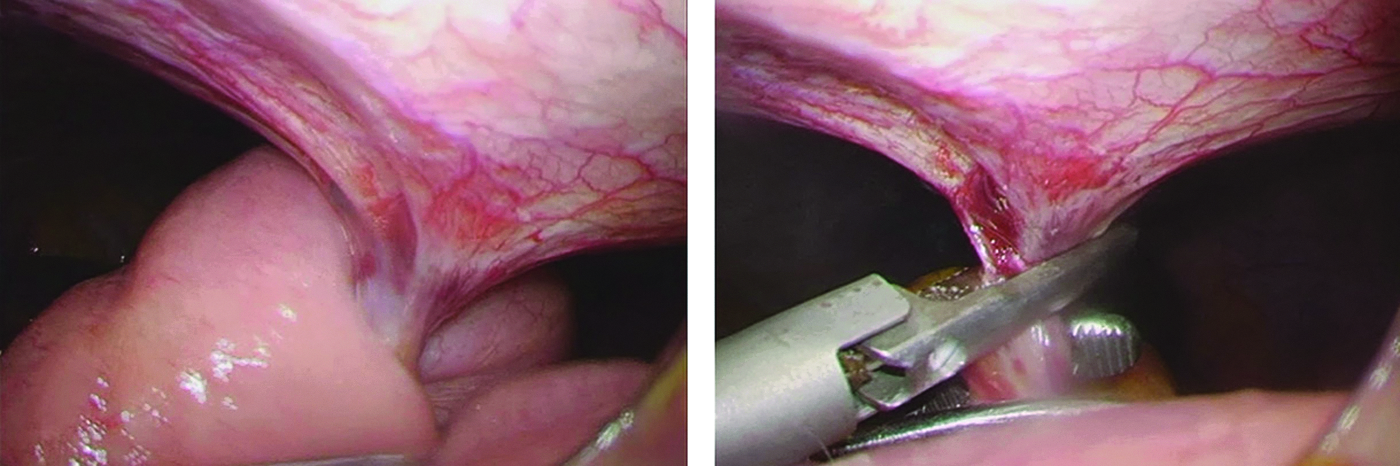
Laparoscopic adhesiolysis for the adhesive band formed between trocar site and small bowel mesentery.
Most patients with an intra-abdominal abscess were managed via use of percutaneous drainage procedures. A LR was required in two patients because of concomitant peritonitis. Figure 4 shows a laparoscopic approach used for drainage of an intra-abdominal abscess around the head of the pancreas and dirty fluid collection in the Morrison's pouch.
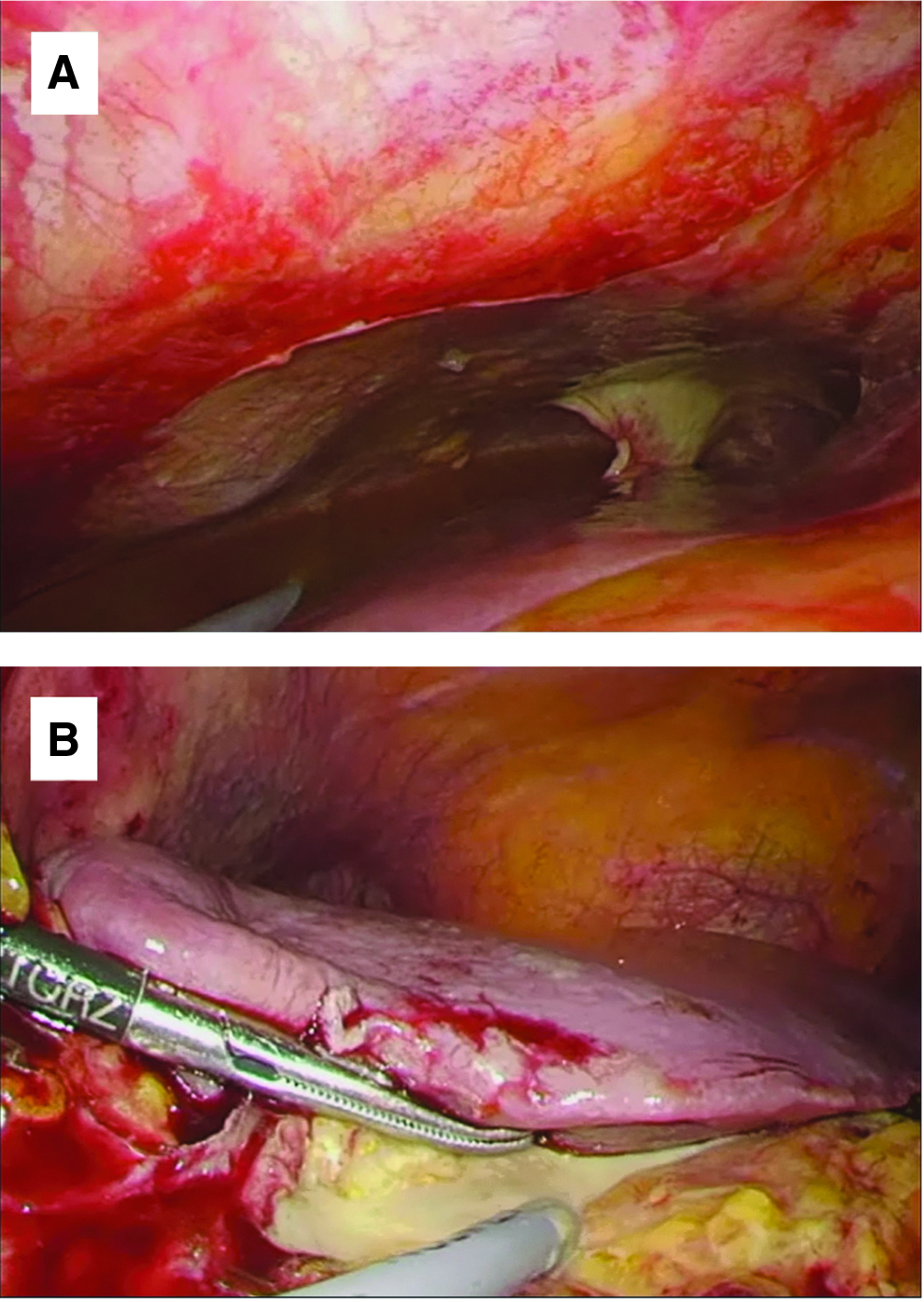
Laparoscopic abscess drainage at peripancreatic head area in patient with peritonitis.
Perireoperation clinical course
Regarding the perireoperation clinical course, a longer operation time was observed in the OR than LR group (118.2 ± 64 minutes versus 156.5 ± 69.7 minutes, P = .097). The estimated blood loss was observed to be higher in the OR than in the LR group (242.9 ± 343.8 mL versus 650.0 ± 674.8 mL, P = .045). The time period from the time of the operation to the occurrence of an adverse event (complication) or secondary management was the shortest in the LR group, but this difference was not statistically significant. The NI and LR groups demonstrated a similar length of stay (LOS) from the time of secondary management. The LOS in the OR group was significantly longer (NI versus LR = 11.6 ± 9.5 versus 11.3 ± 6.0 versus 20.5 ± 14.3, respectively, P = .011) (Table 2).
Discussion
In the present study, 21 patients underwent laparoscopic management for postgastrectomy complications, and all reoperations were successful. Because patient characteristics and situations differed with respect to each procedure performed, comparing secondary treatment results would not be useful. However, a comparison of results between the NI and LR groups in terms of the hospital stay after secondary treatment indicates the usefulness of the laparoscopic approach in the management of postgastrectomy complications. In the OR group, most patients were treated using an open approach because interventional or laparoscopic management was impossible. Therefore, it cannot be conclusively stated that LR is superior to OR in the management of postgastrectomy complications. However, we can demonstrate the feasibility of laparoscopic management. To our knowledge, this is the first study to report laparoscopic management of postgastrectomy complications in patients treated for gastric cancer.
Bleeding is a significant complication and a major cause of reoperation following gastric cancer surgery.2,5 Bleeding is of two types—intra- and extraluminal, and in some instances, both may occur concomitantly. Endoscopic procedures can be successfully used in most situations to control intraluminal bleeding.6,7 However, in patients presenting with exclusive intraluminal bleeding, endoscopic management can fail if an intragastric hematoma obscures endoscopic visualization. In such a situation, laparoscopically placed overlying sutures can be used along the artificial lesser curvature at the site of bleeding. Laparoscopic management of bleeding complications was adopted for extraluminal bleeding. Laparoscopic hemostasis can be easily achieved if and when the staple line is observed to be the site of bleeding. In addition, patients with a large hematoma and/or an unidentified site of bleeding may also be good candidates for laparoscopic management. The example presented in Figure 1 demonstrates the definitive advantages of laparoscopic exploration and hematoma removal over an open laparotomy. Gentle manipulation of a hematoma during removal is important to avoid additional tissue injury, which can cause further bleeding that may mask/obscure the site of injury/bleeding. Thus, intra-abdominal bleeding can be managed laparoscopically. However, this approach should be used cautiously in hemodynamically unstable patients because massive bleeding can obscure a good view of the operative field and prolong the time required to detect the site of bleeding and thereby delay hemostasis.
Anastomotic leakages and/or duodenal stump leakages are additional issues associated with gastric cancer treatment.2,8–10 NI techniques are highly developed and useful for the management of leakage. A temporary covered stent and drainage procedures play a key role in the treatment of esophagojejunostomy leakage. Most duodenal stump leakages are also managed with NI such as percutaneous drainage and interventional Foley duodenostomy insertion. 11 However, not every patient can be effectively managed using NI treatment. When NI treatment is impossible due to a limited percutaneous drainage route or concomitant generalized peritonitis, surgery needs to be performed, and as shown in Figure 2, laparoscopic exploration and Foley duodenostomy can be safely performed. Because of the minimally invasive nature of the surgery and a smaller incision size, as well as reduced surgical stress, patients show an early recovery following reoperation, which reduces the risk of secondary wound complications such as wound contamination or dehiscence.
Usually, laparoscopic management is widely performed for the management of small bowel obstruction secondary to adhesions.12,13 It is important to assess when a reoperation is needed for an intestinal obstruction to manage postoperative intestinal obstruction. The degree of small bowel distension and the presence/absence of adhesions determine the success of a laparoscopic procedure to treat small bowel obstruction. Severe distension of the small bowel can interfere with a laparoscopy and inadvertently precipitate bowel injury due to the limited operating space. However, if proper selection can be ensured, laparoscopy offers several advantages to patients.
As with other complications, NI treatment is the first-choice treatment for the management of an intra-abdominal abscess. However, if a percutaneous window for drainage is absent or in the presence of concomitant peritonitis, a percutaneous drainage procedure cannot be performed or is inadequate to treat each episode of an intra-abdominal abscess. In such cases, laparoscopy provides definite advantages over open procedures in terms of a shorter operative time and a lower rate of wound-related complications.
Our study did not aim to demonstrate the superiority of LR over interventional treatment or OR. However, this comparison was aimed at investigating the feasibility and safety of LR. When comparing surgical results after secondary treatment, OR demonstrated a longer operative time and postoperative hospitalization. However, LR demonstrated similar results when compared with NI treatment. Therefore, LR is a feasible and safe treatment intervention. Of note, because the OR group included patients who could not be treated using the NI or LR approach, the results observed in the OR group should not be interpreted exclusively based on the outcome of the procedure.
A certain degree of bias was associated with our study design because only a laparoscopy was chosen as the first-choice treatment when reoperation was needed. In other words, there can be a different indication in each retreatment procedure. Although treatment strategies can vary between hospitals, we propose that LR strategy can improve surgical outcomes following reoperation in hospitals that do not routinely use the laparoscopic approach.
Conclusion
Laparoscopic management of postgastrectomy complications is a safe and effective strategy in terms of minimal surgical insult and rapid postoperative recovery secondary to a smaller incision, rapid recovery, and shorter LOS than that observed with an open laparotomy approach.
Footnotes
Disclosure Statement
No competing financial interests exist.