
Abstract
Abstract
Background:
Perforation of the esophagus is the most severe complication of transesophageal echocardiography (TEE) and can lead to mediastinitis, pleural empyema, or peritonitis. Currently, the majority of patients receive operative treatment with only 6% treated endoscopically. We report our experience with endoscopic and conservative approaches.
Methods:
We retrospectively reviewed all patients treated for esophageal perforation and included all patients with perforation caused by TEE. All patients with perforation of the esophagus by TEE probe underwent conservative or endoscopic treatment, drainage of pleural and mediastinal retentions, and adjusted to antibiotic therapy.
Results:
From January 2004 to December 2014 a total of 109 patients were treated for esophageal perforation in our department. In 6 patients (5.5%) the perforation was caused by TEE. Location was cervical and midthoracic in 2 and 4 cases, respectively. All patients underwent successful endoscopic treatment and no further surgical procedure, such as esophageal suture or resection was necessary. The mean time between TEE and therapy of the perforation was 7.3 days. In all patients closure of the leakage could be achieved within 30 days. Mortality rate was 0%.
Conclusions:
Esophageal perforations caused by TEE are typically small, in the cervical and mid esophagus, and minimally contaminated. These are good prognostic factors for successful endoscopic treatment with preservation of the esophagus. Operative treatment should only be considered in cases of failed endoscopic treatment.
Introduction
T
Until now, alternative therapeutic endoscopic approaches are rarely used with 5.7%. 4 However, modern technical innovations such as endoscopic vacuum therapy (EVT), stenting, and clipping devices (OTSC®) could alter management of esophageal perforation due to TEE and ultimately reduce the need for more invasive surgery in a large proportion of patients. In our institution, we started performing endoscopic treatment for esophageal perforation in 2002. In this retrospective single-center study, we report our initial experience with endoscopic treatment of esophageal perforations caused by TEE and report characteristics of esophageal perforation and predisposing factors. We suggest an algorithm for therapeutic management.
Methods
We retrospectively reviewed all patients with esophageal perforation who were treated at our institution. All patients with perforation caused by TEE were included in further analysis.
All patients underwent standard diagnostic evaluation, including laboratory testing, endoscopy (Fig. 1) and computed tomography (CT) scan with oral contrast (Fig. 2). The perforation was inspected and the mediastinal wound was cleaned endoscopically. If necessary, additional stenting (covered SEMS) or endoluminal vacuum therapy (Eso-SPONGE®) was used.
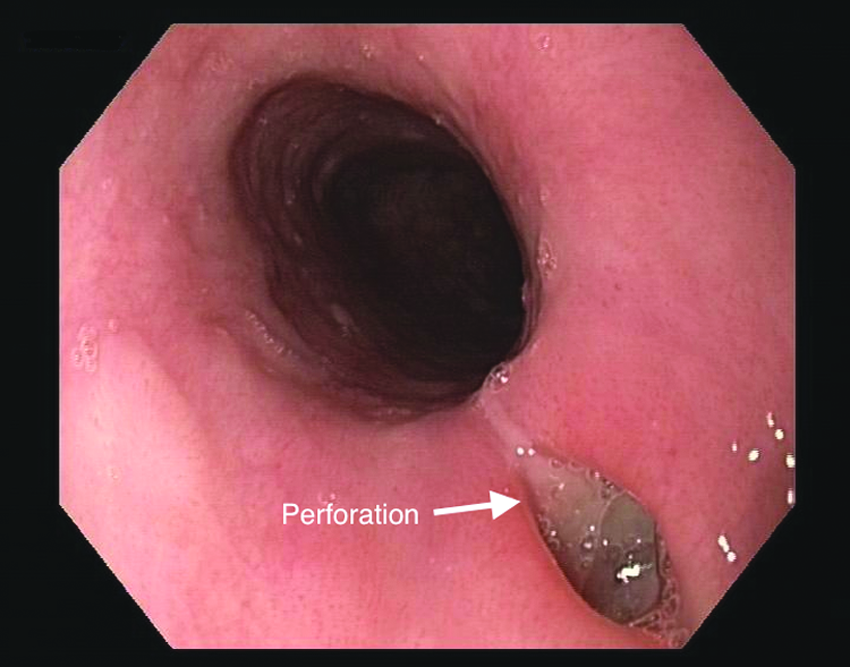
Endoscopy of an iatrogenic perforation of the thoracic esophagus by TEE. TEE, transesophageal echocardiography.

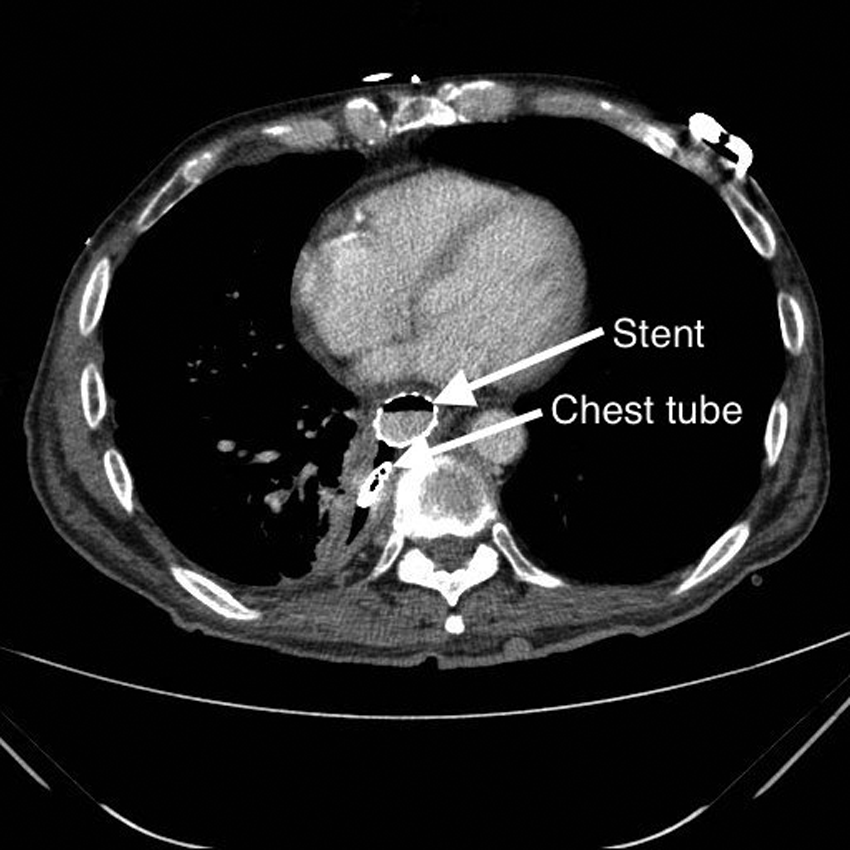
CT scan of an iatrogenic perforation of the thoracic esophagus by TEE. CT, computed tomography; TEE, transesophageal echocardiography.
Perforations of the thoracic esophagus were treated with an esophageal stent (Niti-S™ esophageal fully covered stent, length 100 mm, lumen 20 mm, flares 28 mm, proximal release delivery system; TaeWoong Medical, South Korea) (Fig. 3). Stent application was conducted with a proximal release delivery system under visual control with a flexible endoscope (GIF-Q180/H180 upper gastrointestinal endoscope; Olympus Europa GmbH, Hamburg, Germany). The proper localization of the stent was confirmed during endoscopy and by contrast radiography, including CT scan (Fig. 4). One patient received EVT, endoscopic vacuum-assisted closure with Eso-SPONGE (B. Braun, Aesculap AG, Tuttlingen, Germany) to clean the mediastinal wound. Four days later, the Eso-SPONGE was replaced by an esophageal stent. In addition to endoscopic treatment, pleural and mediastinal effusion was drained by surgical or CT-guided tube placement if necessary (Fig. 4). A broad-spectrum antibiotic (Acylaminopenicillin or carbapenem) and antimycotic (Fluconazole or caspofungin) therapy was given. Blood parameters, such as C-reactive protein (CRP), procalcitonin (PCT), and leucocytes were evaluated. Oral food intake was allowed after sufficient closure of the leakage was confirmed in the contrast radiography (Fig. 5). Stent removal was performed within 4–6 weeks with a grasping forceps in an endoscopic maneuver. Complete closure of the perforation was confirmed in gastroscopy (Fig. 6) and contrast radiography or CT scan with oral radiopaque material.

Endoscopic stenting of the esophagus.
CT scan of an iatrogenic perforation of the thoracic esophagus by TEE. CT, computed tomography; TEE, transesophageal echocardiography.
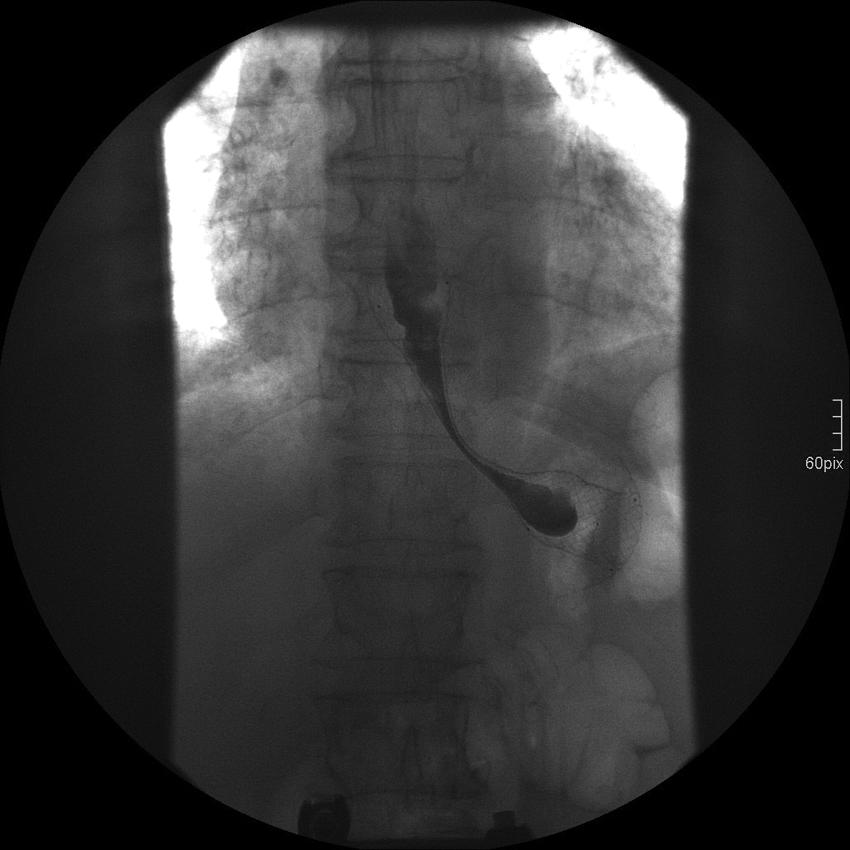
Contrast radiography with oral radiopaque material after stenting of the esophagus.
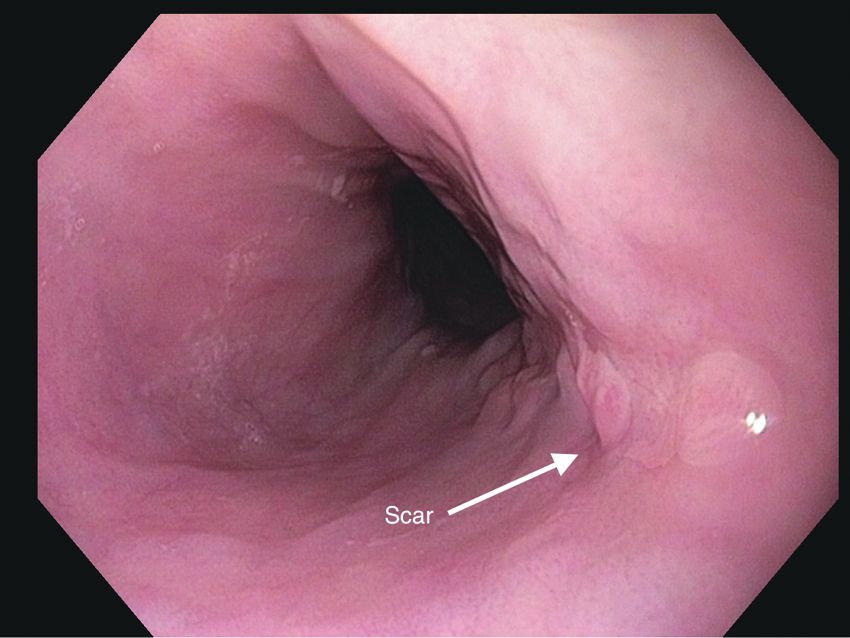
Endoscopy of the esophagus after removal of an esophageal stent.
Perforations of the cervical esophagus were inspected and endoscopically cleaned. If the perforation did not penetrate the pleural cavity, no further endoscopic treatment was necessary. The perforation was treated conservatively with parenteral nutrition under antibiotic and antimycotic therapy. Healing was controlled by periodical endoscopy and control of laboratory values. A contrast radiography or CT scan with oral radiopaque material was performed to evaluate sufficient closure of the perforation before oral food intake was allowed.
Results
From January 2004 to December 2014 a total of 108 patients with perforation of the esophagus were treated in our department. Six (5.5%) cases of iatrogenic perforation of the esophagus caused by TEE occurred. In this time period, a total of 17,620 TEEs were performed in the University Clinic of Cologne. In 3 patients (0.0017%) the perforation developed in an intraoperative setting (2 × transcatheter aortic valve implantation, 1 × open replacement of the aortic valve). In 3 patients, the esophageal perforation occurred during diagnostic TEE in an outpatient setting. All patients were female. Mean age was 75 (43–92) years. Two patients had risk factors for increased risks of esophageal injury, specifically scleroderma, cortisone therapy, and reflux esophagitis. Further characteristics are shown in Table 1.
EVT, endoscopic vacuum therapy.
Patient 1 was an 82-year-old woman without any risk factors for esophageal perforation. She underwent TEE in an ambulatory setting in conscious sedation with Disoprivan and a local anesthetic spray. After the procedure, she had dysphagia and a light cervical pain for 2 days before the perforation was diagnosed endoscopically.
Patient 2 was a 43-year-old woman with reflux disease. She underwent TEE in an ambulatory setting in conscious sedation with disoprivan and a local anesthetic spray. After the procedure she developed chest pain and developed seropneumothorax on day 1 after the intervention. Diagnosis was confirmed by CT scan.
Patient 3 was a 92-year-old woman with scleroderma and cortisone therapy as risk factors. She got a TEE in an intraoperative setting in endotracheal anesthesia. During the operation (transcatheter aortic valve implantation) the patient needed a stabilization of circulation with catecholamine therapy. The patient developed a septic shock on the intensive care unit. Fifteen days after the operation, the perforation of the esophagus was detected in a CT scan.
Patient 4 was an 84-year-old woman without any risk factors for esophageal perforation. TEE was performed in an intraoperative setting in endotracheal anesthesia. During the operation (transcatheter aortic valve implantation) the patient needed stabilization of circulation with catecholamine therapy. The patient developed septic shock on the intensive care unit. On postoperative day 13, perforation of the esophagus was detected in CT scan.
Patient 5 was an 84-year-old woman without any risk factors for esophageal perforation. She underwent TEE in an intraoperative setting in endotracheal anesthesia. During the operation (open replacement of the aortic valve) the patient needed stabilization of circulation with catecholamine therapy. The patient developed a septic shock on the intensive care unit. On postoperative day 13, perforation of the esophagus was detected in CT scan.
Patient 6 was a 64-year-old woman without any risk factors for esophageal perforation. She received TEE in an ambulatory setting in conscious sedation with disoprivan and local anesthetic spray. After the procedure she suffered from dysphagia, cervical pain, and emphysema. An immediate endoscopy showed perforation of the esophagus.
The perforations were located in the middle of the thoracic esophagus at the level of the heart valves in 4 (67%) patients. All of these occurred in an intraoperative setting. Two (33%) perforations were located in the cervical esophagus. These patients had TEE in sedation in an outpatient procedure. The mean time between TEE and detection and therapy was 7.3 (0–15) days. Perforations of the cervical esophagus were detected much earlier (postoperative day 0 and 2). At the time of therapy, 3 patients (50%) with delayed diagnosis of perforation were in a state of septic shock with elevated laboratory infection parameters (leucocytes, CRP, PCT), fever, organ dysfunction, and cardiovascular depression. The patients with an early diagnosis had no symptoms of sepsis. No patient underwent surgical intervention, such as resection or reconstruction of the esophagus. No migration of SEMS was observed. After therapy, all esophageal perforations healed by endoscopic or conservative treatment within 30 days. Ninety days mortality was 0%. The in-hospital mortality of all patients with iatrogenic perforations treated in our department was 3% and of all patients with perforations treated endoscopically was 2%.
Discussion
In this publication, we present the largest single-center analysis of esophageal perforations by TEE published in literature (Table 2).
Current study.
Procedure-associated complications of TEE are rare (3%). One of the most severe complications is perforation of the esophagus. With 6 cases in a series of more than 17,000 procedures, it clearly is a rarity. The increased length of the procedure especially in an intraoperative setting and the larger diameter of the endoscope might cause the higher rate of complication compared with a classical endoscopy. The risk is lower compared with iatrogenic perforation of interventional endoscopy, for example, for simple strictures (0.09%–2.2%). 5
There are predisposing risk factors for esophageal perforations. Among these are esophageal pathology, such as Zenker's diverticulum, esophageal stricture, esophageal or pharyngeal carcinoma, prior chest radiation, esophageal fibrosis, obstructing esophageal mass, esophageal atrophy or ulcerations from medications such as steroids, distorted esophageal anatomy from severe cardiomegaly, prior esophageal surgery, esophageal varices, and degenerative cervical spine diseases.4,6–8 Our data confirm previous descriptions that typically elderly women suffer from iatrogenic esophageal perforation associated with TEE. 9 The reason could be a less elastic, thinner, and more vulnerable esophageal wall in elderly woman. However, there is no absolute contraindication for TEE examination.
In our series, perforations occurred in the cervical and midthoracic esophagus, which is in concert with previous findings. 4 Perforation of the cervical esophagus results from traumatic intubation of the upper esophagus with the TEE probe by passing the upper esophageal sphincter in insufficient conscious sedation. The risk for this complication can be minimized by using a direct laryngoscope to prevent a blind insertion of the TEE probe. 4 Adequate conscious sedation, lubrication of the probe, and local anesthetic spray can be helpful to prevent excessive gagging, and to alleviate the cricopharyngeal spasm.11,12
Perforation of the midthoracic esophagus results from prolonged, continuous pressure, friction against the surrounding tissue and thermal energy released of the TEE probe to the mucosa especially in an intraoperative setting.13–16 The combination of low circulation in the esophagus wall due to cardiopulmonary bypass and underlying atherosclerosis of the esophageal vasculature facilitates necrosis of the esophageal wall. Additionally, the probe of the TEE must be held in maximal antegrade flexion to obtain left ventricular short-axis views. 11 This position may be associated with direct mechanical trauma to the esophageal wall. 17 In an intraoperative setting, the risk of perforation of the esophagus can be minimized by reducing the time of examination.
Time from traumatic perforation to diagnosis and treatment is the most important factor for the development of inflammatory reaction in the mediastinum or pleural cavity and ultimately the development of a state of septic shock, which is associated with high mortality.18–20
In our series, the length of time until detection of the perforations was striking. At the time of TEE multiple attempts of probe insertion, resistance during probe insertion, blood on the probe, or poor quality of sonographic images are alert signals for esophageal perforation. These typical alarming signs, such as retrosternal pain, emphysema of the skin, dyspnea, and dysphagia cannot be evaluated during anesthesia intraoperatively.
In our series, a delayed detection of esophageal perforation was especially found in patients undergoing coronary artery bypass grafting and valvular surgeries. 4 The residual effects of anesthesia, continued mechanical respiratory support, and early postoperative changes on imaging may have confounded and delayed detection. In addition, in case of no typical symptoms for esophageal perforation, clinical findings are often not interpreted correctly and diagnosis of esophageal perforation is easily dismissed. 4 Even minor distinctive or atypical symptoms can be symptoms of perforation. In the intraoperative group, a subacute esophageal perforation from ischemic pressure necrosis in patients with poor esophageal circulation due to vascular disease, low cardiac output, and prolonged operative duration may lead to a secondary perforation of the esophagus. Cervical esophageal injury is likely to be detected earlier, as it happens more often in the nonoperative group of patients, in whom symptoms are more easily detected. 4
Endoscopy is safe diagnostic tool and an important therapeutic component of the management of acute esophageal perforation. This minimal invasive examination provides fast information that can modify treatment. The use of carbon dioxide (CO2) insufflation can minimize the risk of emphysema and pneumothorax. In our experience, the lesion itself can be evaluated more precisely endoscopically while CT scan with oral contrast can better visualize pleural or mediastinal retention. Both diagnostic tools should always be performed in concert to evaluate perforations of the esophagus (Fig. 7).
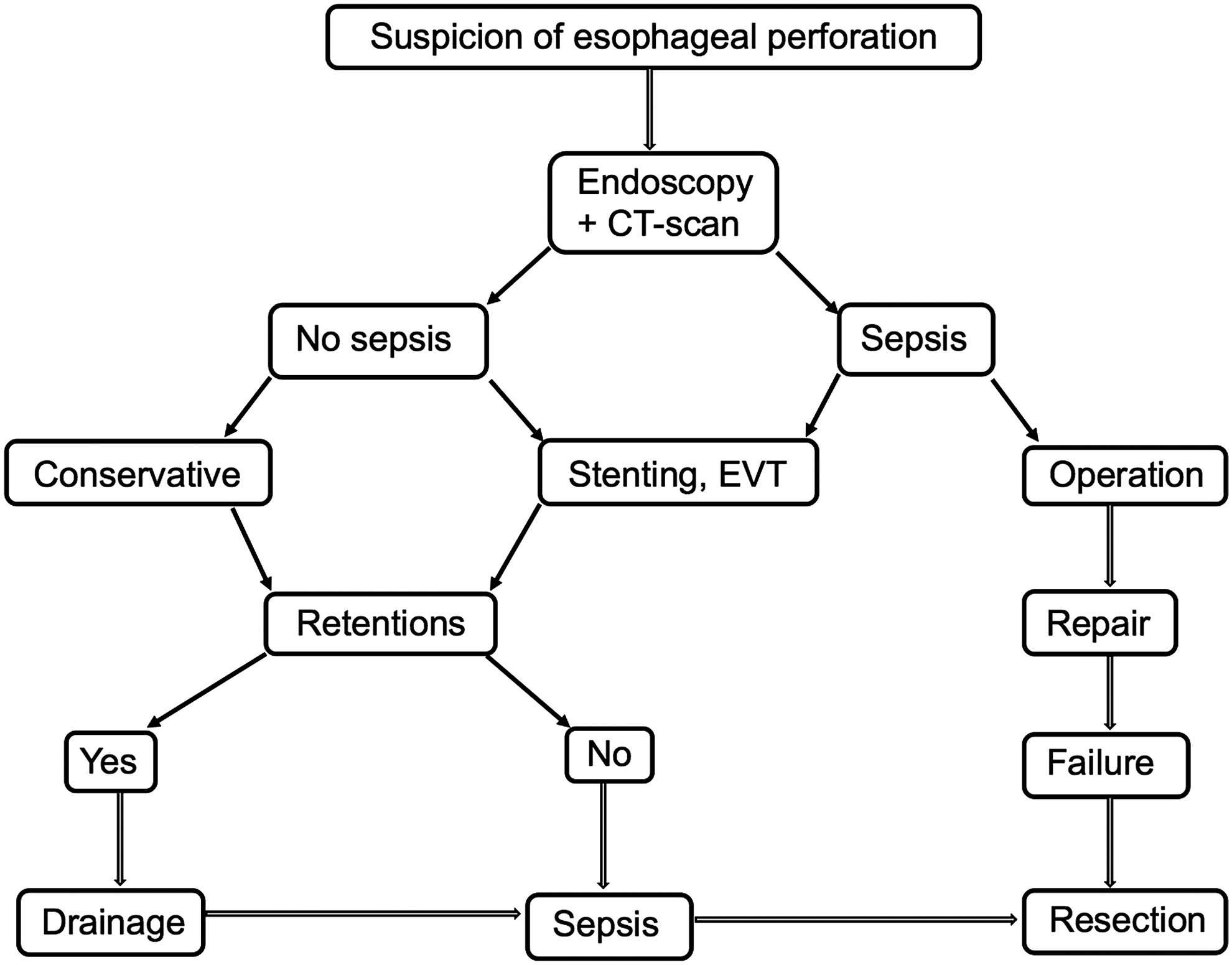
Suggested algorithm for diagnostics and treatment of iatrogenic esophageal perforations.
Ten years ago, nearly every esophageal perforation was treated surgically, including esophageal resection and diversion.19–23 In the last decade, the options of endoscopic treatment have evolved tremendously. Under certain conditions, it replaced surgical treatment for esophageal perforation dependent on etiology of perforation.21,25 Correlation between therapeutic procedure and etiology of 108 patients with perforation of the esophagus treated in our department is shown in Table 3. Traumatic penetrations of the esophageal wall with a TEE probe are ideal cases for endoscopic treatment due to the minimal bacterial contamination of the upper esophagus, the lack of contamination of the wound by stomach contents and the lack of an oral intake. Furthermore, location of the perforation in the thoracic and cervical esophagus are optimal for conservative 25 or endoscopic treatment with EVT24,26,27 or stenting.28–30 The advantage of a successful endoscopic treatment is the conservation of the esophagus in a minimally invasive procedure.
In our experience, infected cervical or mediastinal wounds should be cleaned with the endowasher or an Eso-SPONGE. The sponge continuously removes wound secretion and interstitial edema, improves microcirculation and, therefore, induces an accelerated formation of granulation tissue, resulting in closure of the infected wound.24,26,31 There are different options for closure of an esophageal defect with the endoscope. TTS clips were reported as a successful method for closing esophageal perforations ranging from 3 to 25 mm (median size 10 mm). Because of their limited wingspan they cannot be used to close larger defects. Larger esophageal perforations may be treated using clipping devices such as the OTSC. A limitation of clips is that they cannot approximate perforation edges in case of scarring or inflammation, which is seen in cases of delayed treatment or previous unsuccessful attempts. 32
Due to this rationale, we prefer endoscopic stenting with a fully covered, self-expandable nitinol stent to cover the perforation.5,29,30,33 Stent grafting has been confirmed as an effective endoscopic technique for all kinds of esophageal perforations. A successful stenting can be confirmed by contrast radiography or CT scan with oral radiopaque material. After stenting, oral intake is possible and should be recommended. Pleural or mediastinal effusions have to be drained with chest tubes.18–24,28 Mediastinal effusions that are difficult to access can be drained CT guided. All endoscopic interventions should be accompanied by a sufficient antibiotic and antimycotic therapy.34,35 The infection of the mediastinum is caused by a mixed oropharyngeal bacterial and mycotic flora.36,37 The most common infectious agents are Streptococcus, Bacteroides, Staphylococcus, Hemophilus, Prevotella, Actinomyces, Fusobacterium and Peptostreptococcus.34–38 Mycotic superinfections are found in 40% of all cases of mediastinitis. 39 A broad-spectrum antibiotic therapy with acylaminopenicillin or carbapenem in combination with fluconazole or caspofungin is indicated.
During therapy, laboratory values such as CRP, PCT, and leukocytes should be controlled. If the patient becomes unstable and septic, endoscopic treatment should be reconsidered and an operative procedure should be discussed (Fig. 7). The endoscopic removal of the stent should be performed after 4–6 weeks. 28 In this period most perforations should be healed and a safe and easy endoscopic maneuver to remove the stent is guaranteed. After removal, healing of the perforation has to be confirmed by gastroscopy and contrast radiography.
Mortality after esophageal perforation is high despite definitive surgical or conservative strategy. Analysis of 75 studies showed a pooled mortality of 11.9% (95% confidence interval 9.7–14.3; 75 studies with 2971 patients). 40 The 90-day mortality for perforations by TEE was lower than the 90-day mortality of all iatrogenic and all endoscopically treated perforations. Minimal bacterial contamination of the upper esophagus and the lack of contamination of the wound by stomach contents due to the favorable location of the perforation in the thoracic and cervical esophagus are responsible for the low mortality. Perforations of the distal esophagus are associated with a substantially higher mortality independent of medical treatment. Mortality after operative therapy of TEE-induced esophageal perforation is reported between 0% and 38% (Table 2).6,8,9,11
Modern less-invasive technical innovations in endoscopy have altered management of esophageal perforation in the last few years.
Conclusion
Iatrogenic esophageal perforation by TEE is a rare but serious complication. Perforations occur in the cervical or midthoracic esophagus. Especially in patients with an intraoperative setting or continued mechanical respiratory support, detection of perforation is often delayed. Closure of the defect, sufficient drainage of mediastinal or pleural effusions, and broad-spectrum antibiotic and antimycotic therapy are of upmost importance. In case of TEE-induced esophageal perforations, results of endoscopic treatment with preservation of the esophagus are especially favorable due to the most common location of the perforation in the upper esophagus, the small dimension, and the minimal initial surrounding contamination. With the technical improvement in endoscopy, we expect that it will become the standard approach for esophageal perforations and the need for an operative approach will become a rarity. Screening for risk factors may not eliminate the occurrence of a perforation.
Footnotes
Authors' Contributions
T.H. and J.M.L.: Study conception and design. S.-H.C., P.G., M.M., H.S., H.F., and S.B.: Acquisition of data. T.H., J.M.L., S.-H.C., P.G., M.M., H.S., H.F., and S.B.: Analysis and Interpretation. T.H. and J.M.L.: Drafting of article. M.B., C.G., W.S., and A.H.H.: Critical revision.
Disclosure Statement
No competing financial interests exist.