
Abstract
Abstract
Introduction:
Liver resection in cirrhotic patients is associated with increased morbidity and mortality. The objective of this study was to compare short-term results of laparoscopic resection (LR) and open surgery (OS) for minor liver resection in patients with hepatocellular carcinoma (HCC) hepatocellularcarcinoma on nontumor cirrhotic liver (HCC/F4) and patients with colorectal cancer liver metastases (CRLMs) colorectal liver metastases on healthy liver (CRLM/F0).
Materials and Methods:
Between January 2005 and December 2014, all patients undergoing liver resection (n = 754) were included in this study. Liver resections for cholangiocarcinoma or benign tumor, major liver resection (≥3 segments), HCC on healthy liver, CRLM on cirrhotic liver, and liver resection with technically difficult accessibility (segments I, VII, and VIII) were excluded. The primary endpoint of the study was a validated composite endpoint (CEP), which included specific liver surgery complications (Clavien ≥III), allowing comparison of the postoperative course after LR versus OR for HCC/F4 patients and CRLM/F0 patients using propensity score (PS) analysis. Secondary endpoints were major postoperative morbidity according to the Clavien–Dindo classification (≥III) and intensive care unit (ICU) length of hospital stay (LOS) and overall LOS. The test group was defined as HCC/F4 patients operated by LR, and the control group was defined as HCC/F4 patients and CRLM/F0 patients operated by OS and CRLM/F0 patient operated by LR.
Results:
Sixty patients (38.7%) underwent LR and 95 patients (61.3%) underwent OS. Surgery was performed for CRLM in 93 patients (60%) and for HCC in 62 patients (40%). No difference was demonstrated between HCC/F4 patients and CRLM/F0 patients in the LR group in terms of the CEP (7% versus 18.1%; P = .23), while a significant difference for the CEP was observed between HCC/F4 patients and CRLM/F0 patients after OS (50% versus 21%; P = .021). A higher rate of CEP was observed for HCC/F4 patients operated by OS compared to HCC/F4 patients operated by LR (50% versus 7.8%; P = .009). No significant difference in Clavien–Dindo score ≥III was observed between HCC/F4 patients and CRLM/F0 patients operated by LR (10% versus 4.5%; P = .98). A higher postoperative ascites rate was observed for HCC/F4 patients operated by OS compared to CRLM/F0 patients operated by OS (25% versus 2.8%; P = .006). This difference was no longer observed when HCC/F4 patients were compared to CRLM/F0 operated by LR (7.8% versus 2.8%; P = .09). The postoperative mortality rate was 1.8% and was not correlated with nontumor liver or surgical approach. A shorter LOS was observed for HCC/F4 patients operated by LR compared to HCC/F4 patients operated by OS (7.53 versus 17.13; P = .011).
Conclusion:
The laparoscopic approach for malignant liver tumor is associated with a lower specific complication rate. LR for HCC/F4 could eliminate excess morbidity and decrease LOS in patients with cirrhotic liver.
Introduction
S
Laparoscopic abdominal surgery for colorectal cancer or liver metastasis is feasible even in cirrhotic patients. 4 Laparoscopy for colorectal cancer is associated with a lower postoperative complication rate 5 and similar long-term oncologic results.6,7 Similar results have been reported for LR of colorectal cancer liver metastases (CRLMs). 8 LR compared to open surgery (OS) for hepatocellular carcinoma (HCC) in cirrhotic patients was not associated with increased postoperative morbidity, but decreased the rate of decompensated liver disease 9 and mortality with similar long-term oncologic results.10–12
Data concerning LR for liver tumor are derived from retrospective studies, case series, or meta-analyses. Two consensus conferences were also held in Louisville in 2008 13 and in Morioka in 2015 14 to determine the benefits of laparoscopic liver surgery, but the conclusions of these conferences were based on retrospective studies with a low level of evidence. Recently, the results of a single randomized clinical trial comparing LR to OS for left lateral sectionectomy were published, 15 but failed to demonstrate any benefit or disadvantage of LR as a result of underpowered analysis, mainly due to a change in the surgeon's preference during the study, resulting in poor recruitment. Other series evaluating LR for tumor resection would therefore be useful for surgeons to extend their use and knowledge of the results of minimally invasive techniques for liver resection. 16 A randomized trial comparing LR versus OS for resection of CRLMs (The Oslo-CoMet Study) is currently underway, and results are not yet available. 17
Since it is difficult to design a randomized clinical trial in the field of liver surgery because of the low rate of postoperative complications, we decided to analyze the benefit of LR and OS for minor liver resection in patients with HCC on nontumor cirrhotic liver (HCC/F4) and in patients with CRLMs on healthy liver (CRLM/F0) with a similar methodology to that used in basic research based on comparison between a test group (HCC/F4 patients operated by LR) and 2 control groups: CRLM/F0 patients operated by LR and HCC/F4 patients operated by OS.
Materials and Methods
Population
From January 2005 to December 2014, all patients undergoing surgery for HCC and CRLM were included in this study. This was a retrospective review of a prospective database of a group of patients who underwent liver resection. Some of these patients were entered into a prospectively designed registry (clinicaltrials.gov: NCT01715402).
Assessment of nontumor liver parenchyma
Routine examination of nontumor liver was performed to detect signs of cirrhosis. Depending on the case, examination of nontumor liver was performed on liver resection situated away from the tumor or on an associated liver biopsy also situated away from the tumor. All histological samples were examined by a pathologist specialized in hepato-pancreato-biliary (HPB) diseases.
Definition for healthy liver (F0 patients)
Healthy liver was diagnosed histologically before or during surgery in all patients. Healthy liver was defined according to the scoring proposed by Bedossa and Poynard 18 with absence of fibrosis (stage F0) or portal fibrosis without septa (stage F1).
In the presence of cirrhosis (F4 patients)
Liver cirrhosis was diagnosed histologically before or during surgery in all patients. Cirrhosis was defined according to Anthony et al. 19 as parenchymal necrosis, regeneration, and diffuse fibrosis, resulting in disorganization of the lobular architecture throughout the liver. Nontumor liver was considered to be involved by cirrhosis when fibrosis activity was graded F4 according to the METAVIR classification.
Cirrhosis was also graded according to the Child and Turcotte 20 classification modified by Pugh et al. 21 (total bilirubin, serum albumin, ascites, hepatic encephalopathy, and prothrombin time). Platelet count was also evaluated, and normal blood platelet counts were defined as values between 150,000 and 400,000 platelets per microliter.
When cirrhosis was suspected, evaluation of portal hypertension included preoperative esophagogastroscopy (portal hypertension gastropathy and gastroesophageal varices). Preoperative computed tomography (CT) scan was also systematically performed to screen for splenomegaly (longitudinal diameter >12 cm), recanalization of the umbilical vein, and esophageal varices.
Surgical procedure
The study included two periods, before and after the beginning of laparoscopic liver surgery program in our institution. Then we compared retrospectively patients operated by OS and LR.
Standardized procedure
The surgical procedure started with intraoperative liver ultrasound to locate the lesion, determine the vascular relations, and guide surgical resection. Cotton tape (Péters Surgical, Bobigny Cedex, France) was systematically placed around the porta hepatis to ensure hilar clamping when necessary. The indication for drainage at the end of surgery was left to the surgeon's discretion.
LR specificities
For the LR procedure, the patient was installed in the supine position with the surgeon between the patient's legs and a 15° head-up tilt (French position). Surgery was performed using a 30° laparoscope and 4–6 port sites, and open laparoscopy was performed routinely. Pneumoperitoneum was maintained with abdominal pressure between 12 and 14 mmHg. For lesions in the right lobe, the patient was installed in the same way using a right roll, and the port sites were shifted to the right to increase surgical exposure. Hepatic transection was performed using an energy device, and irrigated bipolar electrocoagulation was used for minor bleeding. Vascular structures larger than 3 mm were secured with clips. When left lobectomy or posterior sectorectomy was performed, the major hepatic veins were divided by a vascular linear stapler such as Endo GIA™ AVM Reload with Tri-Staple™ Technology (COVIDEN France SAS, Elancourt, France). The resected specimen was removed in a plastic bag and extracted through an enlargement of the port sites.
Open resection specificities
The OS procedure was performed using a subcostal, bi-subcostal, or midline laparotomy depending on the site of the tumors (subcostal incision for tumors in the right lobe, midline incision for tumors in the left lobe, bi-subcostal incision for bilobar tumors). Parenchymal transection was performed using an ultrasonic dissector (CUSA®—Cavitron Ultrasonic Surgical Aspirator; Valleylab, Boulder, CO) and bipolar cautery (Bipolar Forceps—Lamidey Noury Medical, Verrières le Buisson, France).
Composite endpoint
The composite endpoint (CEP) was described and validated by van den Broek et al. 22 A CEP is a combination of one or more procedure-specific complications that are considered as a single dichotomous outcome. Components of a liver surgery-specific CEP were selected on the basis of a systematic literature search and consensus among 28 international HPB surgeons. CEPs can be used to design prospective studies with smaller sample sizes, increase the statistical power of the study, enhance the comparability of trial results, thereby facilitating meta-analyses, and take into account multiple outcomes or even multiple types of outcome, thereby evaluating the overall benefit of a single intervention.
This CEP included 6 posthepatectomy events (with Clavien–Dindo scores ≥III): ascites, postresectional liver failure, bile leakage, intra-abdominal hemorrhage, intra-abdominal abscess, and operative mortality. For example, after LR in a HCC/F4 patient, we observed ascites, no intra-abdominal abscess, no liver failure, no hemorrhage, and no death, corresponding to a CEP = 1 (CEP remained 1 when the patient presented one or more items with a Clavien–Dindo score ≥III).
Definition of specific liver complications
Criteria were validated retrospectively according to validated definitions.
Ascites was defined according to Ishizawa et al. 23 as abdominal drain output of ascites fluid of more than 10 mL/kg of preoperative body weight. Clavien 3 ascites was arbitrarily defined to meet the criteria of CEP as requirement of prolonged drainage of the abdominal cavity.
Postoperative liver failure was defined according to Balzan et al. 24 as prothrombin time <50% and serum bilirubin >2.95 mg/dL on postoperative day 5 (“50-50” criteria).
Bile leakage was defined according to Koch et al. 25 as bilirubin level in drain fluid at least thrice higher than serum bilirubin level on or after postoperative day 3 or as the need for radiologic or operative intervention due to biliary collections or bile peritonitis.
Hemorrhage was defined according to Rahbari et al. 26 as a drop in hemoglobin level >3 g/dL postoperatively compared to the postoperative baseline level and/or any postoperative transfusion of packed red blood cells for falling hemoglobin and/or the need for radiologic intervention (such as embolization) and/or re-laparotomy to stop bleeding. Evidence of intra-abdominal bleeding had to be obtained by imaging or blood loss through abdominal drains when present.
Abscess was defined by intra-abdominal collection diagnosed by CT scan or ultrasonography performed in patients with postoperative pain or fever associated with increased white blood cell count.
Classification of surgical complications
Complications were classified according to the classification of Dindo et al. 27 A major complication (grade ≥III) was defined as a complication requiring surgical/endoscopic/radiologic intervention except for ascites, for which prolonged drainage of the abdominal cavity was considered to be Clavien grade ≥III.
A life-threatening complication was defined as a complication requiring ICU management or leading to the patient's death.
Inclusion and exclusion criteria
Inclusion and exclusion criteria were as follows (Fig. 1):
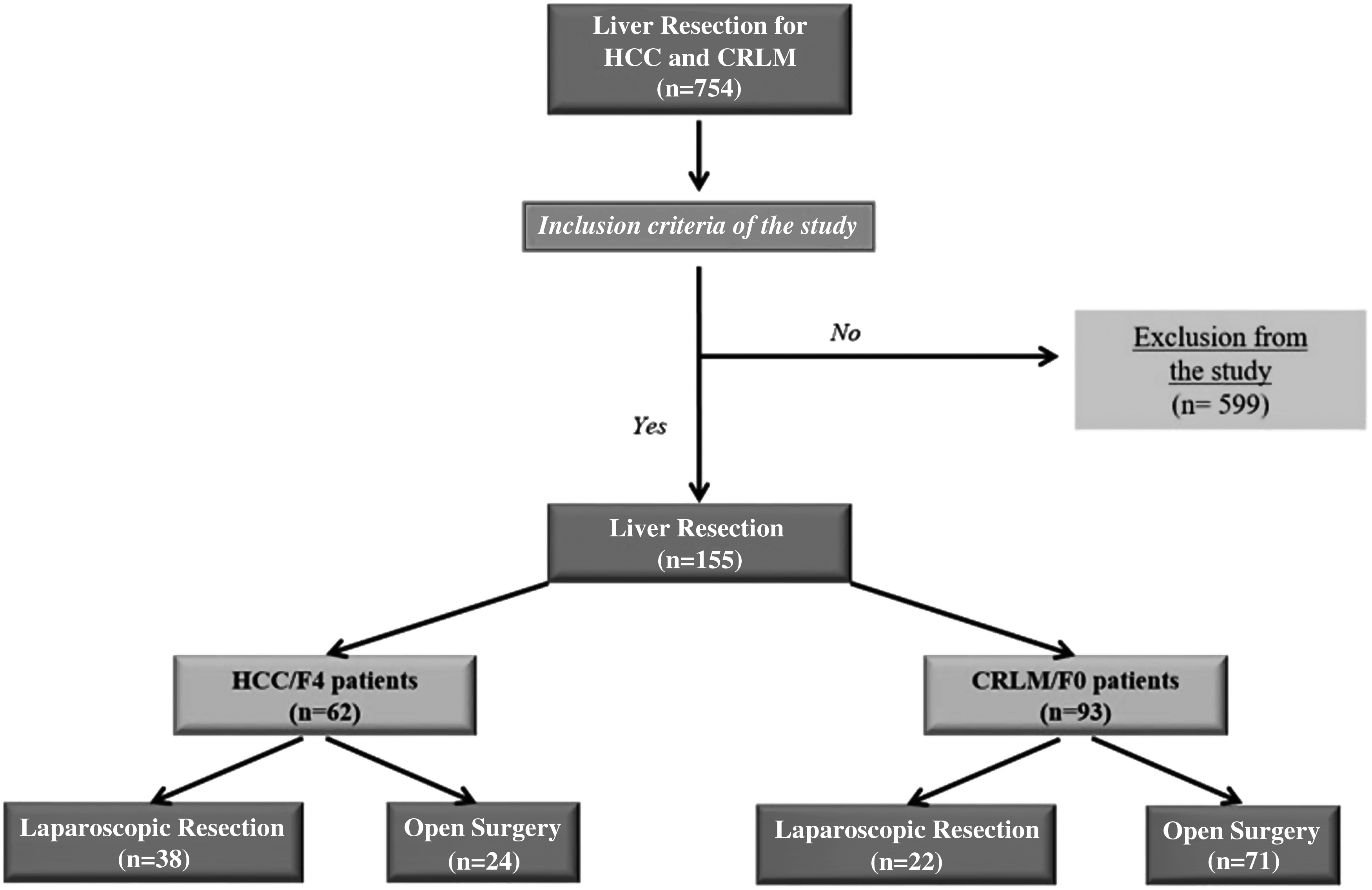
Study flowcharts. CRLM/F0, colorectal cancer liver metastases (CRLMs) on healthy liver; HCC/F4, hepatocellular carcinoma (HCC) on nontumor cirrhotic liver.
Inclusion criteria: minor liver resection (<3 segments) in HCC/F4 patients, including Child A patients ± portal hypertension, and in CRLM/F0 patients for technically accessible lesions with both surgical approaches.
Exclusion criteria: liver resection for cholangiocarcinoma, or benign tumor, major liver resection (≥3 segments), HCC on healthy liver, CRLM on cirrhotic liver, and liver resection with technically difficult accessibility (segments I, VII, and VIII). Child C HCC/F4 patients were excluded. Hepatectomies for CRLM associated with primary tumor resection in the same procedure were excluded.
Study design and endpoints
To demonstrate the benefits of LR for F4 patients, we decided to design our study according to a basic research protocol by defining 2 groups of patients:
Test group, including patients with HCC/F4 who underwent laparoscopic liver resection. Control groups, including HCC/F4 patients who underwent liver resection by OS, CRLM/F0 patients operated by LR, and CRLM/F0 patients operated by OS.
Primary endpoint
The primary objective of this study was to demonstrate the absence of difference in terms of CEP between HCC/F4 patients operated by LR and CRLM/F0 patients operated by LR to prove the benefits of LR for cirrhotic patients.
The primary endpoint was comparison based on the CEP between the test group and the control groups. The CEP was also analyzed in HCC/F4 patients operated by OS and in CRLM/F0 patients operated by OS to highlight the excess morbidity of liver resection associated with cirrhosis.
Secondary endpoints
The secondary endpoints included analysis of the various criteria of the CEP, postoperative morbidity according to the Clavien–Dindo classification, 27 and the hospital LOS.
Collected data
The following parameters were recorded:
Demographic data: age, gender, body mass index (BMI), American Society of Anesthesiology (ASA) score, cirrhosis rate, and cause of cirrhosis. Preoperative data: tumor characteristics (size, number, and site), preoperative therapy (chemotherapy and targeted therapy), and tumor markers (carcinoembryonic antigen and carbohydrate antigen 19-9 for CRLM and alpha-fetoprotein for HCC). Intraoperative data: type of liver resection, surgical approach, and combined procedure. Postoperative data: complications according to the Clavien–Dindo classification,
27
specific complications corresponding to the CEP (fistula/abscess, hemorrhage, ascites, liver failure, and death), length of hospital stay (LOS), and ICU LOS.
Statistics
Categorical variables are expressed as number (percentage) and compared by a Chi-squared test or Fisher's exact test. Quantitative variables are expressed as mean ± standard deviation (range) and compared by a Student's t test according to the application conditions. All tests were two tailed, and the limit of statistical significance was set at P < .05.
To compare the postoperative course between LR and OS for each indication, we performed a case-matched study with intention-to-treat PS analysis. The PS is defined as the probability between 0% and 100% that a patient was allocated to the LR or the OS groups due to the presence of several factors constituting a confounding bias. For calculation of the PS, univariate analysis was performed to identify confounding factors (independent variables: demographic data (age, gender, BMI, ASA score) and preoperative data (type of tumor, size, number and site of tumor(s), associated surgery, chronic liver disease, and preoperative treatment)) influencing the choice of surgical procedure (LR versus OS, dependent variable). Factors with a P value ≤.2 were included in the multivariate analysis with backward selection and factors with a P value ≤.1 were selected. Matching allowed equal distribution of confounding factors between the 2 groups. Two analyses were performed, one without matching and one after matching.
All statistical analyses were performed with SAS software (version 4.3, SAS Institute, Inc., Cary, NC).
Results
Preoperative data
During the study period, 754 patients underwent liver resections: 155 of these patients underwent liver resection for HCC and CRLM and met the inclusion and exclusion criteria. Four patients with HCC on healthy liver and 3 patients with CRLM on liver cirrhosis were excluded (Fig. 1).
Sixty patients (38.7%) underwent LR and 95 patients (61.2%) underwent OS. In this series, 62 patients (40%) had cirrhosis. Patient characteristics and preoperative data for HCC/F4 patients and CRLM/F0 patients are reported in Tables 1 and 2. At baseline, we compared HCC/F4 patients operated by LR and HCC/F4 patients operated by OS and demonstrated differences between the 2 populations in terms of the etiology of cirrhosis, tumor size and tumor site, and type of liver resection (Table 1). The same comparison was performed between CRLM/F0 patients operated by LR or OS, which revealed significant difference for CRLM/F0 patients operated by OS who had an ASA grade ≥3 and a higher rate of repeat liver resection (Table 2). All these criteria were used to construct the PS.
Bold values are statistically significant.
ASA, American Society of Anesthesiology; F, female; LR, laparoscopic resection; M, male; NASH, nonalcoholic steatohepatitis; OS, open surgery.
Bold values are statistically significant.
BMI, body mass index; CAE, carcinoembryonic antigen; CA 19-9, carbohydrate antigen 19-9.
Primary endpoint
No difference were observed between HCC/F4 patients and CRLM/F0 patients in the LR group in terms of the CEP (7% versus 18.1%; P = .23), while a significant difference in terms of the CEP was observed between HCC/F4 patients and CRLM/F0 patients after OS (50% versus 21%; P = .021) with a higher rate of the CEP for cirrhotic patients (Tables 3 and 4). A significant difference with a higher rate of the CEP was also observed for HCC/F4 patients operated by OS compared to HCC/F4 patients operated by LR (50% versus 7.8%; P = .009) (Table 5).
CRLM/F0, colorectal liver metastases on healthy liver; HCC/F4, hepatocellular carcinoma on nontumor cirrhotic liver; ICU, intensive care unit; LOS, length of hospital stay; LR, laparoscopic resection; NS, non significant.
Bold values are statistically significant.
OS, open surgery.
Bold values are statistically significant.
Secondary endpoints
No significant difference for major complications was observed between HCC/F4 patients operated by OS and CRLM/F0 patients operated by OS (41.6% versus 21.1%; P = .137), but a higher rate of ascites was observed for HCC/F4 patients operated by OS compared to CRLM/F0 patients operated by OS (25% versus 2.8%; P = .006). Comparison of HCC/F4 patients operated by LR and HCC/F4 patients operated by OS revealed a higher rate of major complications among patients operated by OS (41.6% versus 10.5% P = .027). This difference was no longer observed when comparing HCC/F4 patients and CRLM/F0 patients operated by LR (10.5% versus 4.5%; P = .98). The postoperative mortality in this series was 1.8%, with no correlation with nontumor liver or surgical approach (Tables 3–5).
Length of hospital stay (ICU LOS and overall LOS)
No significant difference for overall LOS or ICU LOS was observed between HCC/F4 patients operated by LR and CRLM patients operated by LR, and no significant difference was observed between HCC/F4 patients operated by OS and CRLM/F0 patients operated by OS (Tables 4 and 5). A significant difference was observed between HCC/F4 patients operated by LR and HCC/F4 patients operated by OS with a longer mean overall LOS in the OS group (17.13 versus 7.53; P = .011).
Discussion
This is the first study to compare LR and OS in liver surgery using a basic research methodology with a test group (HCC/F4 patients operated by LR) and control groups (HCC/F4 patients operated by OS and CRLM/F0 patients operated by OS) compared by PS analysis with the CEP as primary endpoint to highlight the potential benefit of laparoscopy in cirrhotic patients.
Improvements in surgical techniques and perioperative support have prompted the emergence of newly validated elective indications for wound surgery, 28 cholecystectomy, 29 and colon cancer surgery 30 in cirrhotic patients. In contrast, other indications in cirrhotic patients have not been validated and are still subject to debate, such as surgery for esophageal and stomach cancer 31 and for pancreatic cancer, 32 for which surgery is feasible in selected patients.
Laparoscopic liver resection was first described by Reich et al. 33 and was performed in small benign tumors of the liver edge found incidentally during laparoscopic surgery for gynecologic symptoms, and the first series of LR was reported by Cherqui et al. 34 and concerned 30 patients, including 12 patients with malignant tumors. Since this date, liver LRs have become increasingly popular, but remain reserved to specialized centers experienced in liver resection and laparoscopic procedures. There are many explanations for the difficulties encountered in the promotion of laparoscopic liver resection: long learning curve, fear of intraoperative bleeding, difficulty of exposure, vascular control, and liver mobilization, and few data on oncologic results are currently available. However, recent publications have shown that laparoscopy may be associated with decreased blood loss due to pneumoperitoneum, and laparoscopy may present the advantage of better and more accurate vision of the various elements of the liver parenchyma. 35 Some series suggest that laparoscopy could be associated with decreased postoperative morbidity especially in patients with cirrhosis. 36
Laparoscopy has made a major contribution to the changes in surgical techniques that have allowed decreased postoperative morbidity, by decreasing the postoperative complication rate, particularly by reducing the complication rate in patients with cirrhosis. LR for HCC in cirrhotic patients can be particularly useful with the development of systematic follow-up programs for HCC/F4 patients, allowing early detection of HCC, which constitutes the best indication for LR; second, LR in these patients has been shown to decrease liver-related complications 11 ; third, LR for HCC patients can be considered to be an interim treatment while waiting for liver transplantation; and finally, LR before transplantation facilitates subsequent liver transplantation compared to primary OS. 37
The primary objective of this study was to compare the postoperative course in patients undergoing liver resection by LR and OS for malignant tumor using a validated CEP, including specific complications. The results show that the CEP in HCC/F4 resection differed between the LR group and the OS group with rates of 9% and 48%, respectively. No significant difference in terms of complications was observed between these 2 groups according to intraoperative data, as also described in the series by Sposito et al., 38 analyzing the outcomes of LR and OS for HCC/F4. In a case-matched study of 36 LR versus 53 OS published in 2011, Truant et al. 10 showed lower rates of postoperative complications and ascites (with no significant differences) and a shorter LOS with 6.5 days in the LR group versus 9.5 in the OS group (P = .003).
The postoperative ascites rate was significantly different in the OS group: 24% in cirrhotic patients compared to 2.1% in noncirrhotic patients. A significant difference was also observed for the CEP with a rate of 48% in cirrhotic patients compared to 20.6% in noncirrhotic patients. No significant difference was observed for these two parameters when analyzing the LR group, suggesting that the laparoscopic approach may eliminate the excess morbidity attributable to cirrhotic liver and consequently decrease the postoperative complication rate.
Analysis of morbidity in our CRLM/F0 series demonstrated similar results to those reported in the largest series of laparoscopic liver resection for CRLM/F0 with PS analysis from Beppu et al., 8 as no significant difference was observed between LR and OS in terms of overall morbidity, while a significant difference in terms of major complications (Clavien ≥3) was observed with 3.8% in the LR group versus 27.9% in the OS group. The leading cause of the increased major postoperative complication rate was an increased incidence of pulmonary complications. Fuks et al. 39 also reported an increased rate of pulmonary complications after OS for major hepatectomy (40.5% versus 13.2%; P < .001), which would explain the absence of significant difference on analysis of the CEP, which is specific to liver surgery. In our series, no significant difference was observed between the 2 groups in terms of pulmonary complications because the study population only included patients undergoing minor liver resection.
Our results for HCC/F4 resection using LR are similar to those reported in the literature, particularly the results on intraoperative data, outcomes, and LOS of a French multicenter study published by Soubrane et al. 40 (retrieved from the databases of 9 French tertiary centers with extensive experience in OS and LR for HCC). The major complication rate after HCC/F4 resection was also decreased in the LR group (10% versus 42%; P = .011), as were the LOS and CEP, which can be explained by the fact that laparoscopy has an even greater impact on specific liver complications in the presence of cirrhosis in view of the decreased postoperative ascites rate (P = .032) (Table 5).
This study presents a number of obvious limitations. First, this single-center study was based on a small sample compared to other series. 40 Second, this was a nonrandomized retrospective study with a risk of incomplete data. Third, this study included only minor liver resections. We did not compare major resections for HCC/F4 and CRLM/F0 using LR and OS, as we have a less extensive experience in laparoscopic major resection, possibly because of a shorter experience of laparoscopy compared to laparotomy and because, over recent years, the preservation of hepatic parenchyma during resection has been promoted by the use of other techniques such as intraoperative radiofrequency ablation. 41
Conclusion
Laparoscopy for minor resection of malignant liver tumors is associated with a lower major complication rate compared to open resection. Laparoscopy for HCC with cirrhotic liver could eliminate the excess morbidity associated with cirrhotic liver compared to laparoscopy for CRLM without cirrhotic liver.
Footnotes
Disclosure Statement
No competing financial interests exist.