
Abstract
Abstract
Objective:
Laparoscopic splenectomy (LS) is relatively contraindicated in cirrhotic portal hypertension (CPH) patients with complicating hypersplenic splenomegaly (HS). This study aimed to evaluate the effectiveness and safety of incorporation of iodized oil and gelatin sponge embolization to conventional splenic artery embolization (cSAE) with coiling in CPH/HS patients undergoing LS.
Patients and Methods:
Between April 2012 and March 2014, eligible CPH/HS patients (n = 56) were assigned to preoperative modified SAE (mSAE) with LS (mSAE+LS group, n = 16), cSAE with LS (cSAE+LS group, n = 20) or LS alone (LS group, n = 20). Main outcome measures included frequency of conversion to laparotomy, operative time, intraoperative bleeding, and transfusion.
Results:
The three groups had similar baseline characteristics (all P > .05). mSAE and cSAE similarly decreased LS conversion frequency (mSAE+LS versus cSAE+LS versus LS, 0.0% versus 10.0% versus 30.0%, P = .030) and operative time (155 ± 23 minutes versus 170 ± 26 minutes versus 221 ± 42 minutes, P < .001) compared with LS alone. mSAE significantly reduced bleeding (178 ± 22 mL versus 250 ± 27 mL versus 328 ± 67 mL, P < .001) compared with cSAE and LS alone. The three groups had similar postoperative recovery times and surgical morbidities (all P > .05).
Conclusions:
In CPH/HS patients, preoperative SAE reduced LS conversion frequency and reduced operative time compared with LS alone, while mSAE further decreased volume of blood loss.
Introduction
S
LS is generally thought to be absolutely or relatively contraindicated in cirrhotic portal hypertension (CPH) patients with complicating hypersplenic splenomegaly (HS), a common CPH morbidity. 2 CPH patients with complicating HS (CPH-HS) are at a high risk of bleeding due to splenic vascular remodeling caused by CPH-associated hemodynamic alterations. 8 Compared with that in noncomplicating patients, LS in these high-risk CPH-HS patients is associated with longer operative time, more frequent postoperative complications, and prolonged hospital stay.4–6 Combination of LS with azygoportal disconnection, a treatment modality alternative to LS alone, is associated with a lower risk of surgical morbidities. 9 However, LS combined with azygoportal disconnection demonstrated a highly variable perioperative outcome among previous reports, mainly depending on surgeon's expertise, experience, and case volume.10–15
Splenic artery embolization (SAE) is an effective and safe nonoperative treatment modality for traumatic and nontraumatic splenic disorders, the latter of which include hematologic diseases and hypersplenism, in noncomplicating patients. 16 It remains uncertain in current practice whether preoperative SAE can exert additional benefits on CPH patients undergoing LS for complicating HS. In the conventional SAE (cSAE) procedure, however, coiling of the splenic artery alone cannot fully occlude the splenic collateral circulation in CPH-HS patients. Therefore, we modified the technique of SAE by sequentially filling iodized oil and gelatin sponge particles into the distal splenic arteries and parenchyma, followed by cSAE and LS. The primary objective of this study was to evaluate the effectiveness and safety of the modified SAE (mSAE) in CPH patients undergoing LS for HS in comparison with cSAE and LS alone.
Patients and Methods
Patients
Between April 2012 and March 2014, a total of 59 CPH patients were retrospectively and consecutively hospitalized for elective LS due to complicating HS. The indications were as follows: aged 18–65 years; diagnosed with CPH on upper abdominal medical imaging scan (ultrasonography, computed tomography [CT], and magnetic resonance imaging) and/or histology; with complicating pancytopenia shown on the hematologic test; and with confirmed splenomegaly on plain or contrast-enhanced CT scan. The contraindications were as follows: being pregnant or lactating; with a history of upper abdominal surgery; with complicating active hepatitis (serum alanine aminotransferase >2 times of the upper limit of normal with or without total bilirubin>the upper limit of normal) or decompensated liver disease (Child-Pugh class C); with complicating active gastrointestinal bleeding on physical examination; with suspected or confirmed hepatocellular carcinoma on liver imaging scan and/or serum alpha-fetoprotein assay; with complicating massive splenomegaly (the maximum dimension >30 cm); with complicating serious cardiopulmonary/renal insufficiency or coagulopathy; or rejecting to receive SAE and/or LS. All patients volunteered to give informed consent in writing before operation. All operations, including SAE, were performed by an assigned surgical team led by the corresponding author, including resident surgeons, interventional radiologists, anesthesiologists, clinical pathologists, surgical nurses, and research staff.
mSAE and cSAE
The procedure of SAE was briefly described as below. The patient was positioned supine on the operating table, and ∼10% lidocaine (2–5 mL) was injected into the puncture site of the femoral artery for regional blockade before puncture. A Seldinger-style needle (SCW MEDICATH, Ltd., Shenzhen, China) was used to access the femoral artery through an introducer sheath. A 5F angiographic catheter (Cook Medical, Inc., Bloomington, IN) was used for angiography of the femoral artery, splenic artery, and aortic trunk (Fig. 1A) to delineate the artery diameter, spleen size, collateral circulation, and any anatomic anomaly of the splenic vessels. Use of either mSAE or cSAE was determined at the discretion of the surgeon. For mSAE, the 5F angiocatheter was maintained in the distal splenic artery to occlude the splenic parenchyma using sequential combination of additional iodinated oil (w/v 48%, 20–35 mL; Guerbet LLC, Bloomington, IN) and gelatin sponge particles (diameter 560–710 μm; Ailikang, Hangzhou, China) dissolved in 5–10 mL 0.3-g/mL iohexol (Beilu Pharmaceutical Co., Ltd, Beijing, China). Repeated angiography was performed to characterize embolizing effect of the splenic parenchyma (Fig. 1B); if a successful occlusion was confirmed, the angiocatheter was withdrawn to the middle of the splenic artery, and a coil (MWCE; 5–12 mm; Cook Medical, Inc.) was delivered to completely occlude the main trunk of the splenic artery between the distal end of the splenic artery and the greater pancreatic artery (Fig. 1C). A third angiography was performed to confirm embolization of the splenic and collateral vessels (Fig. 1D). The angiocatheter was removed, and the introducer sheath was heparinized and secured onto the skin. Splenic dimensions were measured using angiography; the splenic volume was calculated as the cube of the maximum dimension, and the change in splenic volume was expressed as the percentage of pre-SAE volume to post-SAE volume (Fig. 1E, F).
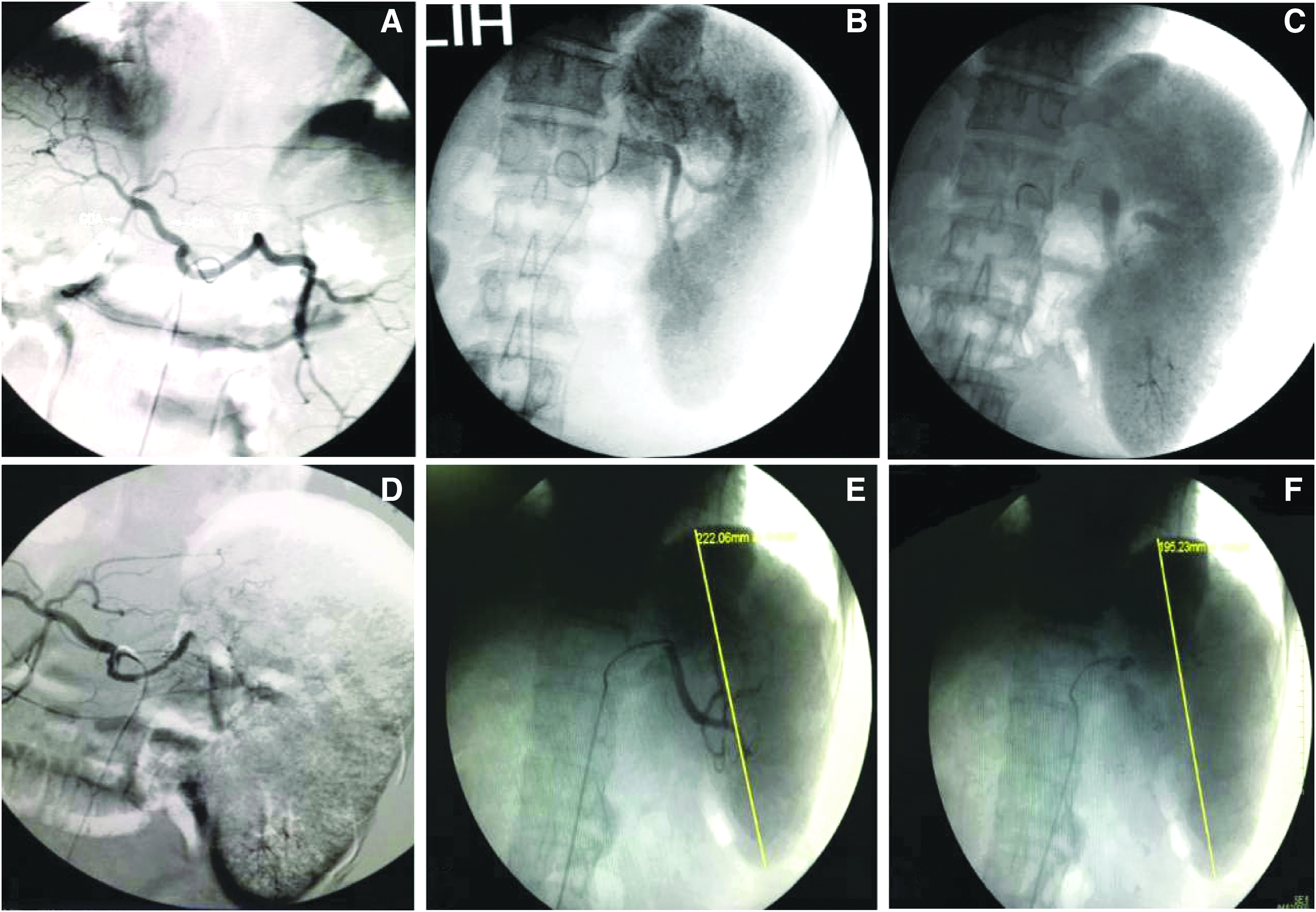
Key procedures of mSAE. Angiography of the
Laparoscopic splenectomy
One hour after SAE, under general anesthesia with endotracheal intubation, the patient was replaced in the 30° right lateral decubitus position, with the head tilted up 30° and with the chest and pelvis cushioned, to expose the left costal margins. Pneumoperitoneum was established at a pressure of 12-mmHg carbon dioxide. A standard four-port technique was used: a 10-mm port at the umbilicus for introducing a 30° laparoscope (Stryker, Kalamazoo, MI), a 5-mm port below the xiphoid process, a second 5-mm port on the left anterior axillary line below the costal margin, and a 12-mm port between the umbilicus and the left costal margin as the primary manipulation port (Fig. 2A). Following a thorough inspection of the peritoneal cavity and the spleen (Fig. 2B, C), the splenic flexure of the colon was retracted downwards using a grasper, and the splenorenal ligament was dissected (Fig. 2D); the splenocolic ligament was dissected using a Harmonic ultrasonic scalpel (Ethicon, Inc., Somerville, NJ; Fig. 2E); and the gastrosplenic ligament was dissected from the upper pole of the spleen toward the greater curvature of the stomach. The splenic pedicle was mobilized and transected using an Echelon EC60A Endopath Stapler (Ethicon, Inc.; Fig. 2F). The mobilized spleen was retracted into an endobag (LOOKMED Medical Instrument Co., Ltd., Changzhou, China) and fragmented under laparoscopic visualization. The secondary 5-mm trocar site was extended into a 3-cm incision to withdraw the resection specimen for histologic examination. Thorough peritoneal exploration was repeated to exclude any active bleeding, and a peritoneal drain was placed in the splenic fossa. All trocar sites were closed in a full-thickness manner. All patients received prophylactic vaccines, antimicrobial prophylaxis, and anticoagulation if indicated, and were followed up at our outpatient clinic using routine hematologic, clinical biochemistry, virologic, and serum oncologic examinations as well as upper abdominal imaging scan if applicable, every 3–6 months within the first postoperative year and every year afterward.
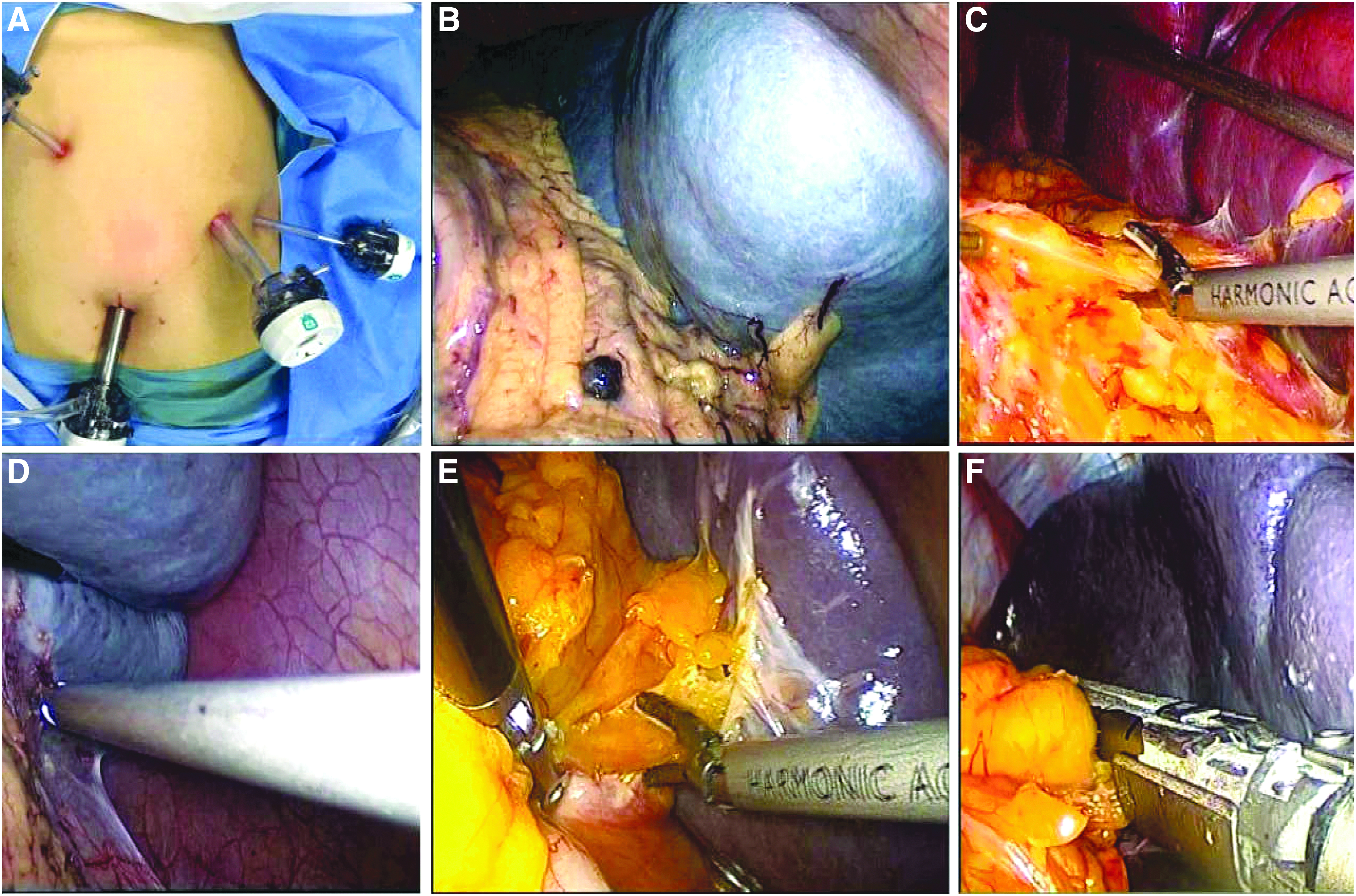
Key operative procedures of LS.
Statistical analysis
Main outcome measures included frequency of conversion to laparotomy, operative time (from establishment of pneumoperitoneum to closure of skin incision), intraoperative blood loss, postoperative recovery times, duration of postoperative hospital stay, and surgical morbidities. The statistical software package SPSS 17.0 (SPSS, Inc., Chicago, IL) was used for statistical analysis. All continuous data were expressed as mean ± standard deviation, and the means were compared using the one-way or repeated measures analysis of variance. All categorical data were expressed as n (%) and analyzed using the Fisher exact probability test. A two-tailed P value less than .05 was considered statistically significant.
Results
Baseline patient characteristics
Out of the 59 patients screened for eligibility, 56 patients were eligible for SAE and LS (mSAE+LS group, n = 16; cSAE+LS group, n = 20; LS group, n = 20), while 3 patients were excluded due to >30-cm splenomegaly. This retrospective cohort of 56 patients included 38 men and 18 women, at a mean age of 42 years (range, 21–63 years). Baseline patient characteristics are shown in Table 1. These three groups were comparable in terms of age, sex, body mass index, spleen size, liver function reserve, and comorbidities (all P > .05). Of note, all patients were positive to hepatitis B virus surface antigen but free of hepatitis C, alcoholic hepatitis, or nonalcoholic fatty liver disease. Nonhemorrhagic esophagogastric varices were observed in 17 (30.4%) patients, and well-controlled diabetes mellitus was identified in 7 (12.5%) patients. All patients received preemptive antiviral treatment as recommended by the clinical practice guideline for management of chronic hepatitis B.
ALB, albumin; ALT, alanine aminotransferase; BMI, body mass index; cSAE, conventional splenic artery embolization; DM, diabetes mellitus; EGV, esophagogastric varices; Hb, hemoglobin; LS, laparoscopic splenectomy; mSAE, modified splenic artery embolization; NS, not significant; PLT, platelet; PT, thrombin time; SD, standard deviation; TBIL, total bilirubin; WBC, white blood cell.
Operative data
After embolization, the splenic volume significantly decreased from the baseline (P < .001) but to a similar extent in mSAE+LS group and cSAE+LS group (37% ± 18% versus 32% ± 22%, P = .458). None of the patients complained of acute splenic infarction-associated fever, nausea/vomiting, or left subcostal pain after embolization.
Operative data are shown in Table 2. mSAE and cSAE resulted in a similar reduction in conversion to open splenectomy (mSAE+LS versus cSAE+LS versus LS, 0.0% versus 10.0% versus 30.0%, P = .033) and operative time (155 ± 23 minutes versus 170 ± 26 minutes versus 221 ± 42 minutes, P < .001) compared with LS alone. mSAE resulted in significantly less bleeding (178 ± 22 mL versus 250 ± 27 mL versus 328 ± 67 mL, P < .001); the frequencies of massive bleeding (>800 mL) and transfusion were similar among these three groups.
cSAE, conventional splenic artery embolization; LS, laparoscopic splenectomy; mSAE, modified splenic artery embolization; N/A, not applicable; SD, standard deviation; U, unit of whole blood (1 U = 200 mL).
Postoperative recovery and complications
Postoperative recovery times and complications are shown in Table 3. The three groups were similar with respect to postoperative recovery times, including times to resume bowel movement, oral intake, and off-bed activities as well as days of hospital stay (all P > .05). Postoperative hematological and liver biochemical profiles were similar among these three groups within postoperative 3 days (all P > .05). Surgical site infection is the major postoperative complication (25.0% versus 20.0% versus 10.0%, P = .135), including intra-abdominal abscess (6.3% versus 5.0% versus 5.0%, P = .892) and postoperative pneumonia (18.8% versus 15.0% versus 5.0%, P = .085). Another common complication was transient mild fever (<38.5°C), at a similar frequency among these three groups (18.8% versus 20.0% versus 15.0%, P = .437). No clinically significant late-onset hemorrhagic event, gastrointestinal perforation, thrombosis, or hepatorenal insufficiency was observed. No in-patient mortality occurred. Asymptomatic portal vein system thrombosis was identified in 6, 6, and 4 patients, respectively, in the first postoperative month (37.5% versus 30.0% versus 20.0%, P = .505), which remained detectable in 2, 3, and 1 patients, respectively, in the third postoperative months (6.3% versus 15.0% versus 5.0%, P = .571). All patients were followed up for 1–3 years as scheduled. Liver disease progression, including variceal bleeding, hepatocellular carcinoma, and death, occurred in 5, 4, and 7 patients, respectively.
ALB, albumin; ALT, alanine aminotransferase; cSAE, conventional splenic artery embolization; Hb, hemoglobin; HCC, hepatocellular carcinoma; INR, international normalized ratio; LS, laparoscopic splenectomy; mSAE, modified splenic artery embolization; NS, not significant; PLT, platelet; POD, postoperative day; PT, thrombin time; PVST, portal vein system thrombosis; SD, standard deviation; TBIL, total bilirubin; WBC, white blood cell.
Discussion
LS may be subject to a high risk of hemorrhagic and other nonhemorrhagic events in CPH patients with complicating HS due to underlying thrombocytopenia, coagulopathy, splenic vessel remodeling, and anatomic distortion, as well as technical complexity of manipulating a massively enlarged spleen. Uncontrollable intraoperative bleeding requires more frequent conversion to laparotomy and compromises the benefit of laparoscopy. Therefore, the European Association for Endoscopic Surgery still considers CPH as one of the major contraindications to LS and also states that massive splenomegaly is associated with a high risk of conversion to hand-assisted laparoscopy or laparotomy. 17 The primary finding of our study demonstrated that preoperative SAE could significantly downsize the HS, reduce the risk of conversion to laparotomy, and better control intraoperative bleeding. Moreover, our mSAE protocol in comparison to the cSAE technique further significantly reduces splenic bleeding.
Conversion to laparotomy is a major intraoperative incident of LS, primarily due to uncontrollable bleeding and technical difficulty in manipulation of a massively oversized spleen, especially in obese patients or those with complicating hematologic malignancies. 18 Wu et al. 19 reported in a comparative study that up to 5% of patients required conversion of LS following cSAE to laparotomy due to serious splenic bleeding, while our mSAE technique zeroed the risk of operative conversion although ours was a small sample. This might result from extensive embolization of secondary splenic arteries and parenchyma in addition to complete occlusion of the splenic artery main trunk in our mSAE protocol. Another reported benefit of preoperative SAE is reduced bleeding from LS, while most of these previous reports included noncirrhotic patients only.20,21 In previous reports regarding hematological patients with complicating HS, preoperative cSAE could downsize the splenic volume by 30%–60% within a relatively wide time frame from 2 weeks up to 4 years.21–23 Our results showed that SAE 1 hour before LS might also benefit CPH patients undergoing surgical treatment of HS, with respect to spleen downsizing, conversion frequency, operative time, and blood loss.
Intraoperative incidents, such as conversion, long operative time, and uncontrollable bleeding, may compromise the benefit of LS associated with minimal invasiveness by increasing surgical morbidity and adversely affecting patient's recovery after LS. 19 In comparison with LS alone, preoperative SAE might expedite postoperative recovery and decrease surgical morbidities, although not statistically significant in consistence with previous reports.18–21 Our results showed that the use of mSAE had no additional benefit compared with that of cSAE, although the former technique significantly decreased splenic bleeding. Portal vein system thrombosis is a major late-onset complication following splenectomy, which requires routine surveillance in CPH patients with complicating HS, especially those at a high risk and requiring medical intervention.24,25 However, LS exhibited a generally favorable safety profile even in the absence of preoperative SAE.
There were some limitations in this study. First, the sample size was relatively small, and the results might be subject to inadequate statistical power and underestimate the benefits of preoperative SAE and additional modification; however, the present cohort was the ever-largest series of CPH patients with complicating HS, a medical condition normally believed to be contraindicated to LS. Second, assignment to preoperative SAE was not randomized, possibly with the SAE+LS group favorably biased, but these groups were comparable with respect to baseline patient characteristics. Finally, time of performing SAE and “waiting” interval was excluded from the analysis of operative time; inclusion of these time intervals might mitigate the benefit of additional preoperative SAE. However, our results showed that incorporation of preoperative SAE could benefit CPH patients with complicating HS by significantly reducing conversion and splenic bleeding.
Conclusions
In conclusion, our study results showed that preceding SAE could significantly downsize the splenic volume in CPH patients with complicating HS within a very short time frame before subsequent LS. Preoperative SAE could significantly reduce the risk of conversion to laparotomy, shorten operative time, and decrease blood loss. Preceding embolization with iodized oil and gelatin sponge further significantly reduced bleeding. Large-scale, randomized controlled studies are required to further validate the effectiveness and safety of preoperative mSAE in CPH patients with complicating HS, a refractory medical condition thought to be contraindicated to LS.
Footnotes
Disclosure Statement
No competing financial interests exist.