
Abstract
Abstract
Introduction:
Laparoscopic percutaneous inguinal ring suturing (PIRS) is a valuable technique to repair indirect inguinal hernias in children. The aim of the study was to show the preliminary results of training in an easy-to-build dry-lab model for laparoscopic PIRS technique.
Materials and Methods:
The dry-lab model consists of two surgical gloves (being the smaller inside the larger). The entry of the glove is tied with a rubber letting a 5-mm trocar within it (optic). Carbon dioxide is inflated through the trocar at 8 mmHg pressure. The four long fingers of the glove simulate four internal inguinal rings. Eighteen participants without significant laparoscopic experience were asked to visualize a video showing a laparoscopic PIRS performed in a 4-year-old girl with a right inguinal hernia followed by a video showing the same technique performed in our dry-lab model. They were then asked to repeat the procedure in each of the four fingers, and the procedures were recorded. Two surgeons using the task-specific checklists (TSCs), global rating scale of operative performance (GRS), and time for the whole procedure evaluated the performance blindly.
Results:
We found significant improvement in median TSC (P < .05) and median GRS each time the procedure was repeated (P < .05). There was significant shortening each time the procedure was repeated (P < .05), except between the third and fourth finger (P = .068).
Conclusion:
Our dry-lab model might be a good option for starting laparoscopic PIRS training.
Introduction
I
The percutaneous inguinal ring suturing (PIRS) 9 is an attractive laparoscopic technique to repair inguinal hernias in children, but passing the suture under the peritoneum in the internal inguinal ring can be demanding.
We created an easy-to-build dry-lab model for laparoscopic PIRS training, and we present here the preliminary results on training in this model.
Materials and Methods
We designed a dry-lab model for training laparoscopic PIRS technique. The model was created using two surgical gloves inside each other, which simulated the peritoneum (the inside glove) and the skin (the outside glove). The entry of the glove was tied with a rubber, letting a 5-mm trocar within it, for the optic. Each finger (excluding the thumb) simulated four internal inguinal rings (Figs. 1 and 2). Carbon dioxide was inflated through the trocar at 8 mmHg pressure.
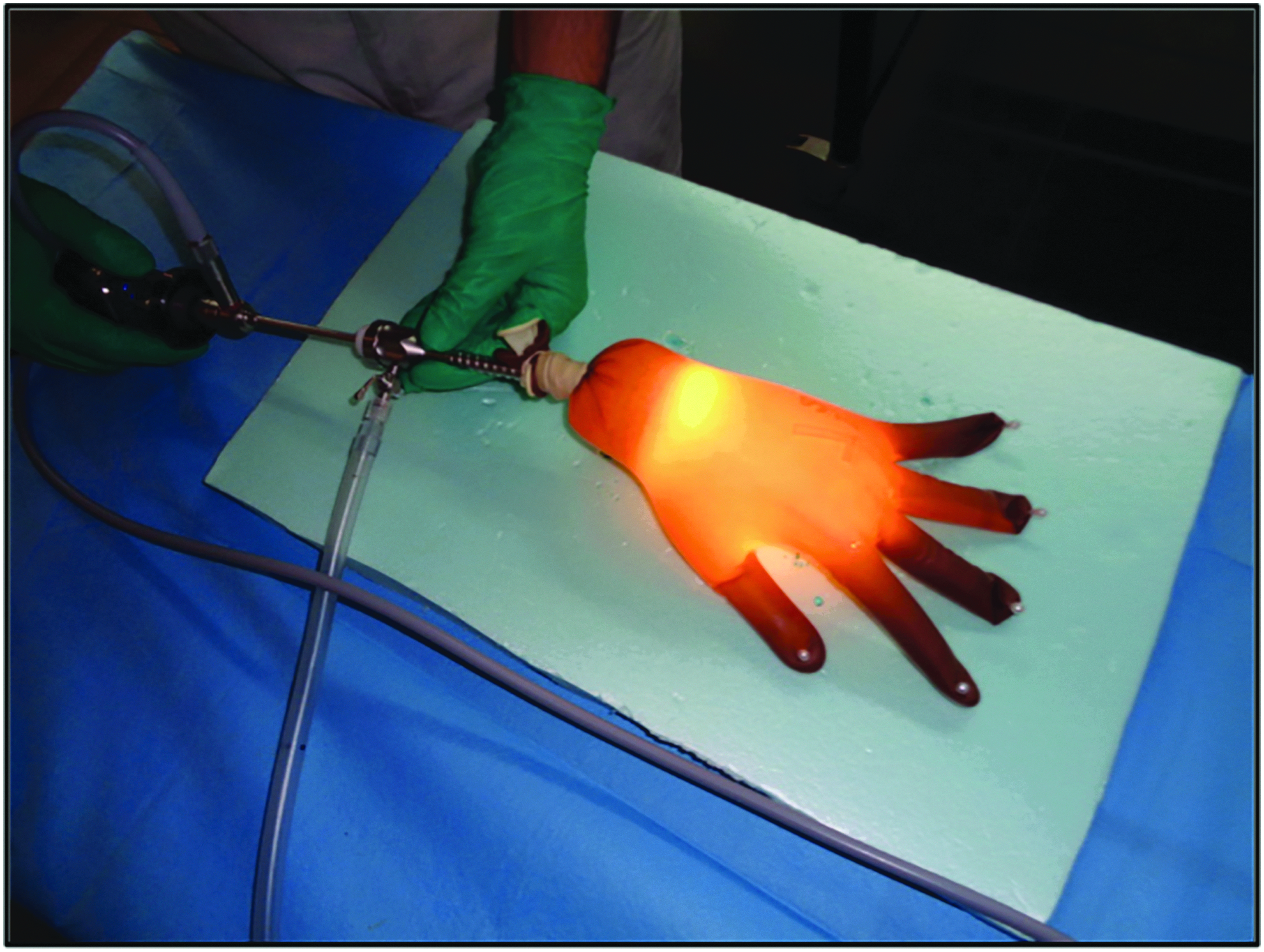
View of the percutaneous inguinal ring suturing technique dry-lab model.

Inside view of the model—each finger representing an internal inguinal ring.
For the suturing technique, hypodermic 18G needles and Ethicon® Ethilon thread (monofilament 2-0) and Ethicon® Ethibond Excel thread (multifilament 2-0) with the needles removed were used. The hypodermic needle, with the monofilament thread inside it, pierces the outer glove (representing the skin) and makes half a circumference around the internal inguinal ring, extraperitoneally (preserving the inner glove). At this stage, the peritoneum is pierced, and a loop of thread is left inside. With the multifilament thread, the hypodermic needle pierces the exact same initial puncture site, and makes the other half of the internal inguinal ring. The second needle goes through the loop made by the first thread, and the second thread is left there. Both ends of the first thread are pulled and completely removed. The ends of the second thread are tied and the internal inguinal ring (glove's finger) is closed (Supplementary Video S1, Laparoscopic PIRS Technique Performed in our Dry-Lab Model; Supplementary Data are available online at www.liebertpub.com/lap).
Each participant was asked to visualize a video showing a laparoscopic PIRS performed in a 4-year-old girl with a right inguinal hernia, followed by a video showing the same technique performed in our dry-lab model.
After that, the participants were asked to repeat the procedure in each of the four fingers and the procedures were recorded. Each finger is referred to as M1 through M4.
The participants were volunteers attending the 6th year medical school, and junior residents without significant laparoscopic experience. This was a nonrandom sample of participants.
Variables to characterize the population were collected: (1) number of participants, (2) academic degree, (3) age, and (4) sex.
Two surgeons evaluated the performance of each participant, blindly.
As a means to evaluate surgical performance, a modified version of the objective structured assessment of technical skills (OSATS) was applied. 10 The task-specific checklist (TSC) was adapted so that all the steps of the PIRS technique were evaluated; each of the 15 steps represents a single technical gesture of the procedure organized sequentially. Each step was evaluated as correctly or incorrectly performed, counting 1 and 0 points, respectively. The overall punctuation of the TSC was obtained by the sum of the evaluation of each step. From the global rating scale of operative performance (GRS), only 4 of the 7 point Likert scale were selected, because only these were adequate to the technique in question: (1) time and motion, (2) instrument handling, (3) flow of operation, and (4) knowledge of specific procedure. The overall punctuation of this Scale was registered as the sum of the evaluation of the 4 scales.
Time spent to complete the procedure was another variable analyzed.
The technical goal was defined as single and complete passage of the second thread through the ring of the finger opening, in the space between both gloves, with both thread extremities at the surface allowing for the surgical knot at the end.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics 22.0 64-bit (IBM Corporation® 2013) and Microsoft® Excel 2013.
Descriptive statistics, used for categorical variables, were based on the calculation of the absolute and variable frequencies.
For variables that did not have a normal distribution, medians were calculated.
To assess differences between each pair of moments for the punctuation obtained in the TSC and the GRS and procedure time, the Wilcoxon test was used.
Ethical considerations
This study was approved by the Ethics Subcommittee for Life and Health Sciences of the University of Minho.
Results
There were 18 participants in this study, aged between 23 and 27 years (median 25 years); 66.7% were female, and 94.4% were junior residents.
In Figures 3–5, we are able to see the progression of the median of each variable along the 4 moments. The TSC and GRS medians increased along the 4 moments, and the median time do complete the task decreased.

Progression of the median of the task-specific checklist along the four moments.

Progression of the median of the global rating scale of operative performance along the four moments.
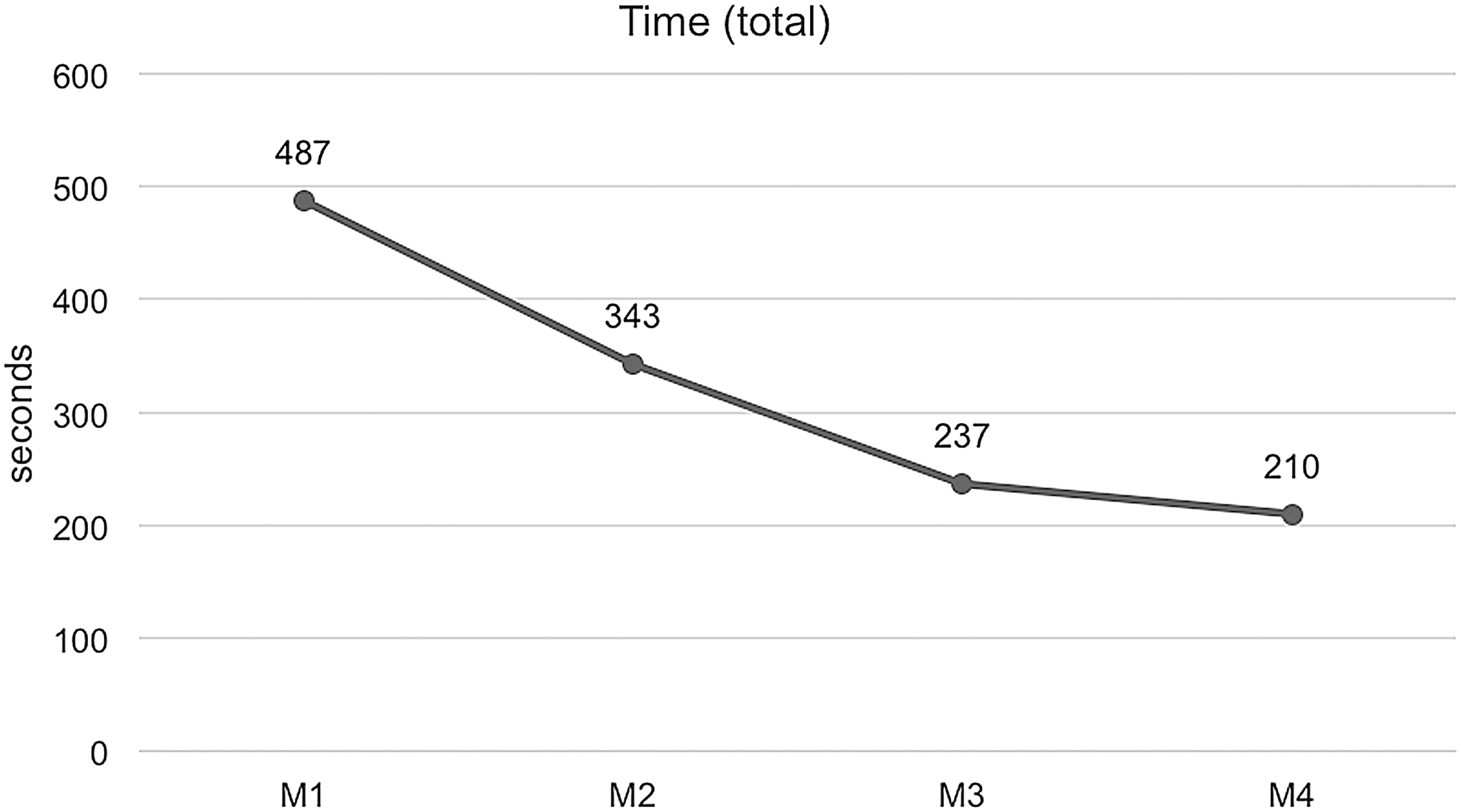
Progression of median of time spent to complete the task along the four moments.
When comparing each pair of moments, we found significant improvement in median TSC (P < .05) and median GRS (P < .05), each time the procedure was repeated. There was significant shortening each time the procedure was repeated (P < .05), except between the third and fourth fingers (P = .068).
Discussion
In the last few years, there have been various laparoscopic techniques described to correct inguinal hernias in children.1,3–9 The PIRS technique, utilized in our dry-lab model, was first described by Patkowski et al. 9 We introduced two modifications to the original description of the technique: we use two hypodermic needles to follow each half of the deep inguinal ring (semicircle), which carry the two different threads (nonabsorbable monofilament and multifilament). The multifilament thread is used for the final knot.
Surgical skills can be trained in the operating room (OR), under direct supervision.10,11 However, there are other methods for learning surgical skills. Nowadays, simulation is a well-established component of surgical training. 12 It is known to allow surgical skills acquisition in a preclinical and safe environment, and has been shown to improve performance in the OR.12,13 There are some studies supporting that the skills obtained in dry-lab models can be partially adapted to the OR.13,14
The method we used to evaluate the participants, the OSATS, 10 is a tool that allows quantification of surgical skills either in simulated training or on the OR. We adapted it to our specific dry-lab model.
As illustrated in Figures 3–4, the median TSC and the median GRS increased along each moment. In a similar way, the median time spent to complete the task decreased along the four moments, as depicted in Figure 5.
When we did an evaluation of the progression between each moment, we verified a significant improvement in the TSC and GRS medians each time the procedure was repeated, which means there was a positive acquisition of technical skills throughout the experiment. There was also significant shortening each time the procedure was repeated, except between the third and the fourth fingers. With repetition and training, the task gets completed faster, reaching a plateau at the 3rd repetition.
As already noted by other studies with other models,13,14 there is a positive effect of training in dry-lab models in obtaining technical skills.
One limitation of our dry-lab model is that it only simulates the PIRS technique in females, because the spermatic cord is not represented. The model is also a simplification of the abdominal wall anatomy, and not all layers are represented.
For future validation of this model, the skills acquired by the participants need to be tested in in vivo model or real case patients.
However, we think that the progression achieved by most of our participants can let us conclude that our dry-lab model might be a good option for starting laparoscopic PIRS training in female children.
Footnotes
Acknowledgments
This article has been developed under the scope of the project NORTE-01-0145-FEDER-000013, supported by the Northern Portugal Regional Operational Programme (NORTE 2020), under the Portugal 2020 Partnership Agreement, through the European Regional Development Fund (FEDER). This work has been funded by FEDER funds, through the Competitiveness Factors Operational Programme (COMPETE), and by National funds, through the Foundation for Science and Technology (FCT), under the scope of the project POCI-01-0145-FEDER-007038.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.