
Abstract
Abstract
Background:
Peripheral arterial disease (PAD) is a complex and highly prevalent pathology. It has been estimated that ∼8.5 million people in the United States are affected by PAD, of which 12%–20% are older than age 60. The TransAtlantic Inter-Society Consensus (TASC) guidelines classified aortoiliac atherosclerotic disease based on morphology and level of lesions. TASC II guidelines recommend bilateral surgical bypass to the femoral arteries for TASC II C and D lesions. The aortobifemoral bypass (ABF) has been considered the gold standard in the treatment of aortoiliac occlusive disease (AIOD). The long-term patency rate of 85%–90% at 5 years and 75%–80% at 10 years has been for a long time unmatched by other methods of revascularization.
Methods:
This is a review of the current literature regarding minimally invasive strategies in the care of TASC II C and D aortoiliac disease.
Results:
Endovascular therapies have led to a paradigm change even in the treatment of highly advanced lesions. Reconstruction of the aortic bifurcation for distal aortic and/or ostial unilateral/bilateral common iliac artery disease can be achieved via the deployment of stents with “kissing” technique and aortic endografts. Laparoscopic aortoiliac surgery for TASC II C and D lesions was first proposed in 1993. Total laparoscopic, laparoscopic-assisted, and laparobotic techniques have been described. Minimal incision aortic surgery (MIAS) describes abdominal incisions varying from 6 to 12 cm and positional adjustment of retractors to access the retroperitoneum for infrarenal aortic aneurysms and/or AIOD.
Conclusions:
Although initial enthusiasm laparoscopic aortic surgery and MIAS have failed to gain acceptance in the vascular surgery community due to intrinsic procedural challenges, they are currently practiced in few highly specialized centers. At this moment, high-quality evidence is lacking regarding the further feasibility of these techniques and their applicability in general practice compared to endovascular therapies. While the ABF remains still the optimal choice in select, fit for surgery patients, endovascular therapies offer a less invasive approach that may provide a mortality and morbidity benefit in higher risk patients with acceptable short- and long-term outcomes.
Introduction
P
The development of atherosclerotic plaques in the abdominal aorta has been observed as early as the first decade of life. Aortoiliac occlusive disease (AIOD), in particular, seems to be more prevalent in younger patients. 2
While the majority of patients may be asymptomatic for a long time, the most common clinical manifestations are intermittent claudication (IC) and critical limb ischemia (CLI). IC typically presents with buttock/thigh pain on ambulation. It has been estimated that 10%–20% of patients initially diagnosed with AIOD and IC develop worsening claudication, and 5%–10% progress to CLI. 1 CLI can be defined as a syndrome characterized by chronic lower extremity rest pain, nonhealing ulcers, and/or gangrene. The incidence of CLI has been estimated as high as 500–1000 per million per year in patients with PAD. 1 Mortality, mostly associated with myocardial infarction and stroke, is threefold higher in patients with IC (25% at 1 year from diagnosis) with a 10%–40% primary amputation rate. Different classifications of PAD are currently in use. 3
The Fontaine's and Rutherford's scoring systems (Table 1) differentiate pathologic stages of chronic limb ischemia based on the presence of lower extremity symptoms and lesions. 3
Norgren et al. 1
The Transatlantic Inter-Society Consensus (TASC) classification, on the contrary, is an anatomic classification system that provides characterization of the various arterial occlusive disease patterns and provides guidelines on treatment, approaches, and optimal revascularization strategies. 1 These guidelines, which were first published in 2000 and later revised in 2007, stratified aortoiliac atherosclerotic disease into categories, from A to D, based on morphology and level of lesions. TASC A lesions represented the least complex anatomic scenario, whereas TASC D lesions represented the most complex revascularization scenario (Fig. 1). 1
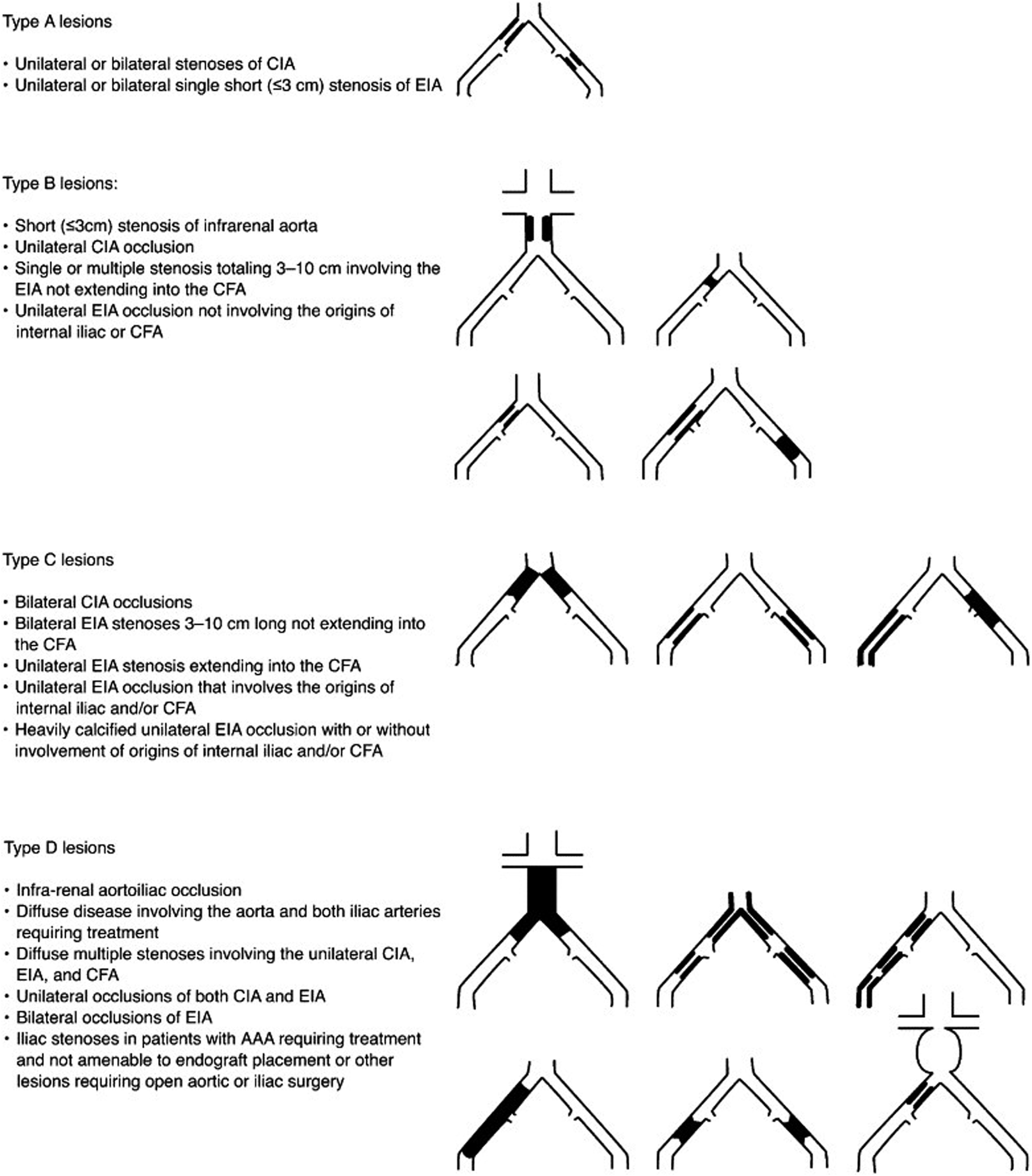
TASC classification of aortoiliac lesions. AAA, abdominal aortic aneurysm; CFA, common femoral artery; CIA, common iliac artery; EIA, external iliac artery; TASC, TransAtlantic Inter-Society Consensus. (Adapted from Norgren et al. 1 )
TASC II D lesions include the following:
Infrarenal aortoiliac occlusion Diffuse disease involving the aorta and both the iliac arteries requiring treatment Diffuse multiple stenosis involving the unilateral common iliac artery (CIA), external iliac artery (EIA), and common femoral artery (CFA) Unilateral occlusions of both CIA and EIA Bilateral occlusions of EIA Iliac stenosis in patients with an abdominal aortic aneurysm requiring treatment and not amenable to endograft placement or other lesions requiring open or iliac surgery
Historically, the aortobifemoral bypass (ABF) has been considered the gold standard in the treatment of AIOD. 2 This is also reflected in the TASC II guidelines that recommend bilateral surgical bypass to the femoral arteries for TASC II C and D lesions. 1 The long-term patency rate of 85%–90% at 5 years and 75%–80% at 10 years has been for long time unmatched by other methods of revascularization. 2 Excellent outcomes have been confirmed by several studies over the last three decades, with less than 5% 30-day mortality rates and acceptable 30-day complication rates in select patient populations.1,4 However, the advent of new technologies has recently allowed the development of minimal invasive strategies in the care of patients with TASC II C and D lesions.
Endovascular therapy
Although available literature has overwhelming data supporting open revascularization as a main strategy to manage extensive AIOD,1,2 recent advances in endovascular therapies have led to a paradigm change in the approach and treatment of highly advanced lesions. Such endovascular options can be used as stand-alone treatment to recanalize previously occluded or diffusely diseased aortoiliac segments or as hybrid procedures in combination with open repair.
When contemplating endovascular recanalization of occluded aortoiliac segments, preoperative planning is of utmost importance. Computed tomography, angiography, and magnetic resonance angiography have become highly sensitive and specific in the description of vascular disease morphology and levels of pathology. 5 The use of catheter angiography is currently reserved for the study of more distal runoff vessels, and is most often combined with endovascular treatment. Access to the arterial system is commonly gained via open or percutaneous access of the common femoral and/or brachial artery. In certain cases of combined aortoiliac and infrainguinal disease, revascularization of the profunda femoris and superficial femoral artery may also be required. This can be achieved via unilateral and/or bilateral femoral artery exploration, endarterectomy, patch angioplasty, and profundoplasty.
Aortoiliac stenosis and occlusions are navigated and crossed with combinations of soft tip wires and more rigid wires supported by a wide variety of sheaths and catheters. Re-entry devices, such as the Pioneer Catheter® with needle deployment and the Outback system®, are available in the market and can be used to aid re-entry into the vessel lumen in case a subintimal plane in the iliac vessels is developed. Although angioplasty alone or angioplasty with stenting can be used, it is suggested that primary stenting may be favored in occlusive lesions. 6 Reconstruction of the aortic bifurcation for distal aortic and/or ostial unilateral/bilateral common iliac artery disease can be achieved via the deployment of stents with “kissing” technique. 6 Stents may be balloon expandable or self-expanding, covered or uncovered. 6 Another approach that has been recently reported with success is the use of aortic endografts to reline the recanalized segments (Figs. 2A, B, and 3). 7
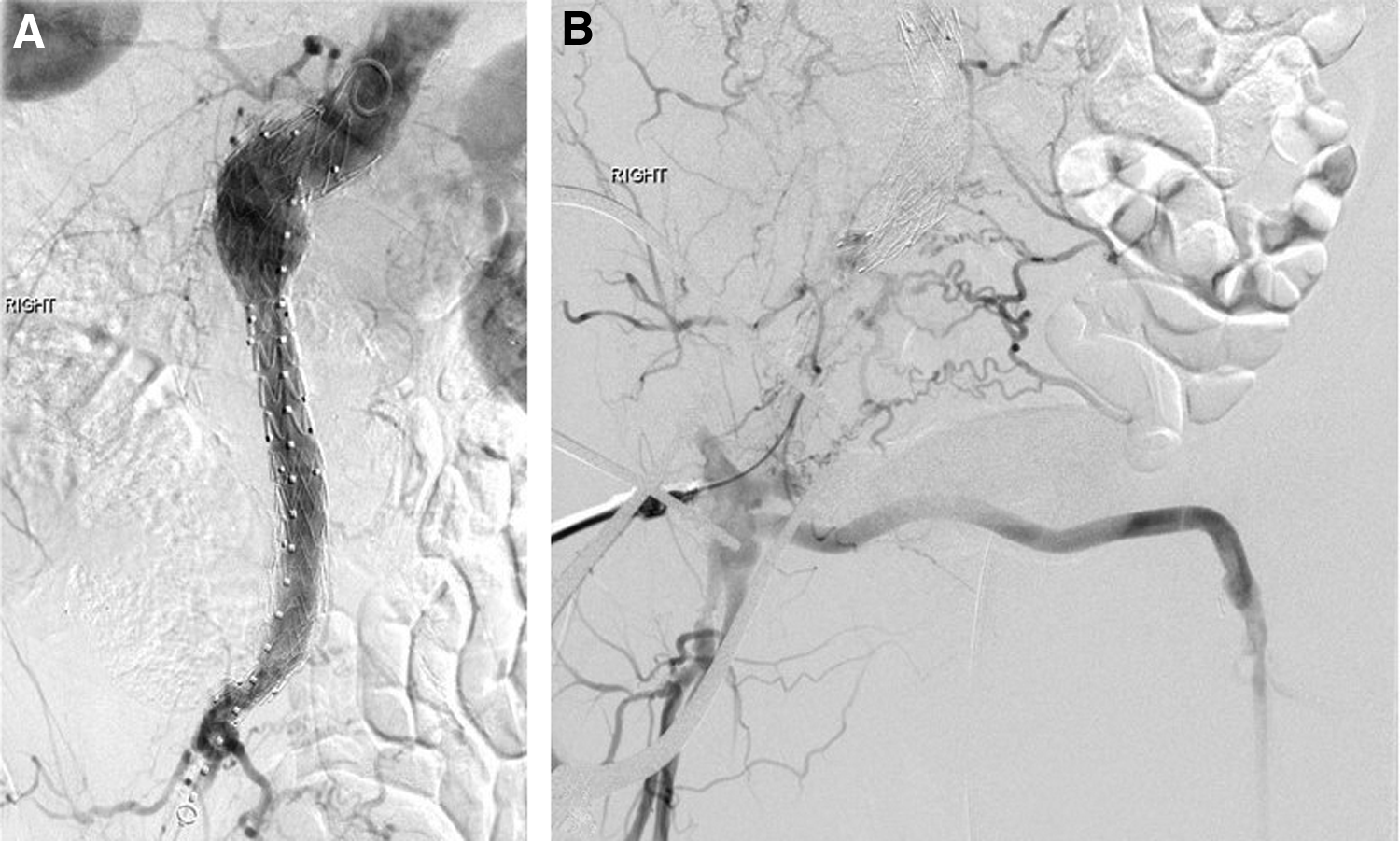
Aortoiliac reconstruction with an aortouni endograft

Aortoiliac reconstruction with Endologix Unibody Endograft®.
In a multicenter retrospective review of the Endologix Unibody Endograft® in AIOD, by Maldonado et al., 91 patients, of whom 67 (74%) with lifestyle limiting IC and 24 with CLI (26%), underwent lower extremity revascularization for AIOD with the Endologix Unibody Endograft with 100% technical success and 1% 30-day mortality rate. 8 The reintervention rate was 10% (16 secondary interventions) and at 22.2 ± 11.2 months of follow-up, primary patency rates were >90%, assisted patency rates >98%, and secondary patency rates 100%. 8 The authors concluded that the use of the AFX Unibody Endograft® was safe and effective in the treatment of AIOD. 8
Overall, the endovascular treatment of TASC II C and D lesions has shown to be highly effective.
A systematic review of endovascular treatment of extensive AIOD identified 19 nonrandomized cohort studies with 1711 patients. The open approach for endovascular access was used in only two studies. 9 In 10 studies, additional surgical outflow procedures, such as common femoral artery endarterectomy, femoro-femoral bypass, and femoropopliteal bypass, were performed. Primary stenting with a wide variety of bare metal stents, covered stents, and aortic endografts was adopted in the majority of reports. Balloon expandable stents were mostly used in calcified lesions. 9 Given the heterogeneity of the studies included in the analysis, the reported 30-day mortality rate varied between 1.2% and 6.7%. Morbidity rates ranged between 3% and 45%. The most common complications were access site hematomas (4%–17%), distal embolization (1%–11%), arterial dissections (2%–5%), pseudoaneurysms (0.5%–3%) and iliac or aortic ruptures (0.5%–3%). Length of hospital stay ranged from 1 to 4.8 days. One-year primary patency rates were estimated between 70% and 97%, while secondary patency rates ranged between 88% and 100%. In eight studies, 5-year patency rates were 60%–80% and secondary patency rates were 80%–98%. In two studies, open surgical reconstruction was compared with endovascular reconstruction. 9 Patients in the open group tended to be older, but the overall comorbidity pattern was similar. Perioperative morbidity rate seemed to be higher in one study (pulmonary complications 13%; cardiac 9%; local wound complications 6%). In the same study, intraprocedural complications occurred in 10% of patients. Both studies reported statistically significant lower long-term primary patency rates in the endovascular group (69% versus 93%, P = .013 and 74% versus 93%, P = .002), whereas the secondary patency rates were essentially similar to the open group (89% versus 100%, P > .05 and 96% versus 96%). 9
Hybrid repair by endovascular revascularization and open common femoral artery endarterectomy has been recently compared to open aortoiliac reconstruction by interrogating the national Vascular Quality Initiative database. 10 The cohorts included 879 patients in the open group and 1472 in the endovascular. Patients in the endovascular cohort were older and more likely to have significant comorbidities, such as diabetes and cardiac failure. Thirty-day mortality was lower in the endovascular group (1.8% versus 3.4%; P = .01). 10 Moreover, shorter length of stay (3 days versus 7 days; P < .001) and higher 1-year mortality (8.6% versus 6.3%; P = .04) were observed in the patients undergoing endovascular reconstruction. Patients with open surgical reconstruction exhibited greater long-term Ankle Brachial Index improvement (0.39 ± 0.37 versus 0.26 ± −0.23; P < .001) and were more likely to achieve ambulatory status (82% versus 65%; P < .001). Major amputation rates were equivalent in the two groups. The authors concluded that open repair should be considered for patients with AIOD and reasonable surgical risk. 10
In a recent retrospective review encompassing 210 open (ABF) and endovascular interventions (aortoiliac kissing stents) from 2006 to 2013 in patients with TASC II C and D lesions, comparison between the open and endovascular group yielded no statistical difference in terms of interval, primary-assisted, and secondary patency rates at long-term follow-up. Reintervention rates were higher (11%) in the kissing stent group. 11 CLI was noticed to be associated with a poorer primary patency (hazard ratio 2.4; 95% confidence interval 0.9–6.4; P = .05). 11
Laparoscopic aortoiliac surgery
Laparoscopic techniques have also been proposed in the treatment of TASC II C and D AIOD.12,13 The first laparoscopic-assisted ABF was described by Dion et al. in 1993. 13 Dissection of the aorta and creation of the retroperitoneal tunnels to the femoral regions were performed with the laparoscopic technique via placement of seven 10-mm trocars (Fig. 4). 3 An end to side aortic anastomosis was then performed via a midline laparotomy incision after evacuation of the pneumoperitomeum. 6 In 1998, the same authors published their early experience with the new technique in 10 consecutive patients with “incapacitating claudication.” 14 The mean total aortic clamping time was estimated as 121 minutes with 66 minutes of aortic anastomosis period and mean blood loss of 820 mL. 14 Mean surgery time decreased from 510 to 245 minutes in the more recent surgeries. 14 In the same year, Barbera et al. described their early experience with 24 totally laparoscopic procedures for AIOD. They performed 7 iliofemoral, 5 aorto-unifemoral, 11 ABF, and 1 aortic endarterectomy. Twenty procedures were performed in total laparoscopy and 4 with hand-assisted techniques. 15 In four instances, conversion to open surgery was necessary. Overall mean operative time was less than 300 minutes with minimal estimated blood loss for the 7 iliofemoral bypasses (92 ± 49 mL) and less than 1000 mL for the other procedures. 15 Mean postoperative length of stay varied from 7.4 days for the iliofemoral bypasses to 10.1 days of the ABF. The authors concluded that laparoscopic aortic surgery of AIOD was feasible, safe, and effective. 15 However, an initial collaboration with experienced laparoscopic surgeons was needed. 15 Since then, total laparoscopic and laparorobotic techniques 16 have been described, but their adoption has been challenged by intrinsic procedural difficulties due to the steep learning curve compared with the more popular and accessible endovascular techniques.17,18 This has become particularly evident in the recent years with the introduction of vascular surgery residency programs that may not offer advanced laparoscopic training. A systematic review of the medical literature between 1990 and 2016 regarding totally laparoscopic ABF identified 66 studies for a total of 588 patients, of whom 22 underwent repair of abdominal aortic aneurysms and 566 were treated for AIOD. 17 In 5 studies, 211 laparoscopic bypasses were compared with open procedures. Total operative time and clamping time were significantly shorter in the open group. Thirty-day mortality and morbidity were equivalent in the two cohorts of patients. Hospital stay after laparoscopic surgery was 12.1 days versus 12.8 days of the open group. 17 The authors concluded that laparoscopic surgery may be a feasible option in the treatment of AIOD. 17 It was also pointed out that the studies included in their analysis were highly heterogeneous and lacked higher grade level of evidence. 17

Laparoscopic dissection of the infrarenal aorta
In a cost–utility analysis comparing laparoscopic versus open aortobifemoral surgery, 50 consecutive patients were randomized to either totally laparoscopic (n = 25) versus open ABF (n = 25) at the University of Oslo in Norway. 19 While operative time was shorter in the open group (196 min [160–230] versus 221 [203–248], P = .024), there were no statistically significant differences in 30-day readmission rate, 30-day mortality, and overall morbidity between the two cohorts. Postoperative hospital stay was 4.0 days (3.0–5.0) in the laparoscopic patients and 7.0 (6.0–9.0) in the open patients (P = .0001). Quality-of-life scores based on the EQ-5D-5L questionnaire showed a statistical advantage in the laparoscopic group. The cost of the procedures at the University of Oslo was lower in the laparoscopic cohort (9,953 € versus 17,260 €), which was mainly related to the longer hospital stay of the open patients. It should be pointed out that the two patient's cohorts were homogenous regarding demographics and the preoperative surgical risk and that the majority of patients (19 in each group) were Fontaine 2b at the time of surgery. 19 It could be argued that these patients would have also done well with the more common endovascular therapy.
Laparoscopic ABF has also shown to have excellent long-term results. A retrospective review from Lecot et al. included 87 totally laparoscopic ABFs performed from 2003 to 2013. Conversion rate was 20.6%. Thirty-day Mortality rate was 1.1% and median length of hospital stay was 6 days. Five-year primary and secondary patency rates were greater than 90%. In their conclusions, the authors remarked the good results, “albeit at the cost of a steep learning curve.” 20
Minilaparatomy
Minimal incision aortic surgery (MIAS) describes abdominal incisions varying from 6 to 12 cm and positional adjustment of retractors to access the retroperitoneum for infrarenal aortic aneurysms and/or AIOD.
In a prospective nonrandomized trial, Maloney et al. reported their preliminary experience in 21 consecutive elective graft repairs for aneurysmal disease and AIOD. Significant difference in favor of MIAS included shorter intensive care unit stay (1 day versus 1.8 days), earlier return of bowel function (4 days versus 4.7 days), and shorter overall length of stay. 21 In 2000, the same group published their experience with MIAS in comparison with conventional aortic surgery and endovascular repair of infrarenal aortic aneurysms. MIAS was found to be more cost-efficient than standard open repair ($12,585 versus $18, 445) as well as endovascular repair ($12,585 versus $32,040) due to shorter length of hospital stay and decreased intraoperative cost, respectively. 22 It should be pointed out that only patients with aneurysmal disease were included in this case series. In a retrospective series from the University of Ljubljana in Slovenia, 23 33 patients underwent aortoiliac reconstruction for AIOD via a 6–8 cm midline laparotomy incision (Fig. 5A–C). Retroperitoneal dissection was carried in a standard manner. Aortic clamping was achieved through two Cosgrove flex clamps inserted via two 1 cm incisions in the left upper quadrant and right lower quadrant. An end to side anastomosis was performed through the minilaparotomy. 23 Mean aortic occlusion time was 17 ± 6 minutes, with a mean intensive care unit stay of 32 ± 8 hours. In 27 patients, regular diet resumed from 2 to 3 days after surgery. Patients undergoing the minilaparotomy required less pain medication postoperatively and had more acceptable cosmetic results. 23

Minilaparotomy
Despite these encouraging preliminary experiences, MIAS has failed to gain acceptance because of intrinsic technical difficulties related to the retroperitoneal and aortic anatomy as stated by Fearn et al. recently. 24 In the same review, it was pointed out that only 2% of patients with aneurysm disease have an anatomy suitable for an open repair via an 8 cm incision and only 30% through a 10 cm incision. 24 Minilaparotomy is currently used in combination with laparoscopic-assisted and robotic techniques. 25
In 2012, Lin et al. published his experience with robotic-assisted aortic surgery with and without minilaparotomy for complicated occlusive and aneurysmal. His series included 21 patients of whom 2 had TASC II C and 10 TASC II D aortoiliac disease, 6 an infrarenal aortic aneurysm, 1 an iliac aneurysm, and 2 a persistent Type 2 endoleak that underwent ligation. Only 3 patients had a totally robotic ABF, while 15 required a minilaparotomy for aortoiliac reconstruction. Operative time and estimated blood loss seemed significantly less in the totally robotic ABF.
Conclusions
The TASC guidelines recommend open surgery for patients with TASC II C and D lesions. 1 Laparoscopic techniques for AIOD have been advocated to provide more durable procedures because of their adherence to the TASC II guidelines of performing a more direct approach to pathology. 15 Moreover, in experienced hands, the results and outcomes of this approach appear to be comparable with open surgery. 20
Laparoscopy, robotic techniques, and MIAS have failed to gain acceptance in the vascular surgery community due to intrinsic procedural challenges and they are currently practiced in few highly specialized centers. At this moment, high-quality evidence is lacking regarding the further feasibility of these techniques and their applicability in general practice compared to endovascular therapies. 18
While the ABF remains still the optimal choice in select, fit for surgery patients, endovascular therapies offer a less invasive approach that may provide a mortality and morbidity benefit in higher risk patients with acceptable short- and long-term outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.