
Abstract
Abstract
Purpose:
Robotic surgery should be considered a technical opportunity for many procedures in pediatric age. The purpose of this study is to verify the correlation between robotic procedures and low weight.
Materials and Methods:
It is a retrospective study (2013–2017). We included all patients who underwent robotic assisted surgery for major procedures in two Italian centers for pediatric surgery. All patients were divided into two groups (group A ≤15 kg and group B > 15 kg). Parameters considered were as follows: time to console, average time procedures, time of hospitalization, and minor/major complications. Statistical test used was Wilcoxon–Mann–Whitney test.
Results:
We enrolled 83 patients. Group A: 28 patients, medium weight 11.2 kg (range: 7–15 kg). Group B: 55 patients, average weight 40.8 kg (range: 15.2–120 kg). In relation to the outcomes considered, we found statistical significance in relation to surgical time and time at the console.
Conclusions:
The retrospective analysis of our case found that body weight cannot be considered an absolute contraindication for the execution of surgical procedures in robotics. The improvement of instruments permits to perform complex surgical procedures in low-weight children without additional difficulties. However, it is important to point out that the youngest child of our case had a weight of 7 kg.
Introduction
Minimally invasive surgery had its major development in the last two decades, finding the main expression in laparoscopic surgery. Laparoscopy has improved postoperative discomfort and morbidity, decreased hospital stay, and enhanced recovery and wound cosmesis. Nevertheless, it presented several limitations such as two-dimensional visualization of the surgical field with loss of depth perception, counterintuitive movements with rigid and nonarticulated instruments, loss of eye-hand coordination, and poor ergonomics for the operating surgeon. 1 At the beginning of 21st century, it was possible to overcome these difficulties with the development of robotic surgery, which offered three-dimensional (3D) visualization, complete camera control, tremor filtering, and articulated instrumentation. Thanks to this, robotic surgery has largely been used in general surgery and soon has its role in pediatric surgery. 2 In this article, we evaluate the applicability of robotic surgery in the pediatric field, analyzing, in particular, the possible limitations on patient weight.
Materials and Methods
A retrospective study was conducted in two Italian centers, Department of Pediatric Surgery of Siena and Genova, between February 2013 and August 2017. The first department was in a hospital, which is a tertiary care center that has multiple services using the robot, including our pediatric general surgery division and four adult departments (urology, cardiothoracic, gynecology, and general surgery). The second one was in a children's hospital. Both surgical robots are the Da Vinci surgical robot made by Intuitive Surgical (Sunnyvale, CA). The authors received introductory robotic training in the course offered by the manufacturer. We have the original four-arm Da Vinci with three instrument arms and one camera arm. We had only the 8 mm instruments. For this study, we considered all children undergoing robotic surgery. The whole population was divided into two groups, depending on the intervention weight: group A, patients weighing more than 15 kg, and group B, children up to 15 kg. Figures 1 and 2 show the “docked” robot on patients of the two sizes compared (over and under 15 kg). For both groups, the following parameters were analyzed: time to console, total surgical time, stay time, conversion rate, and complications.
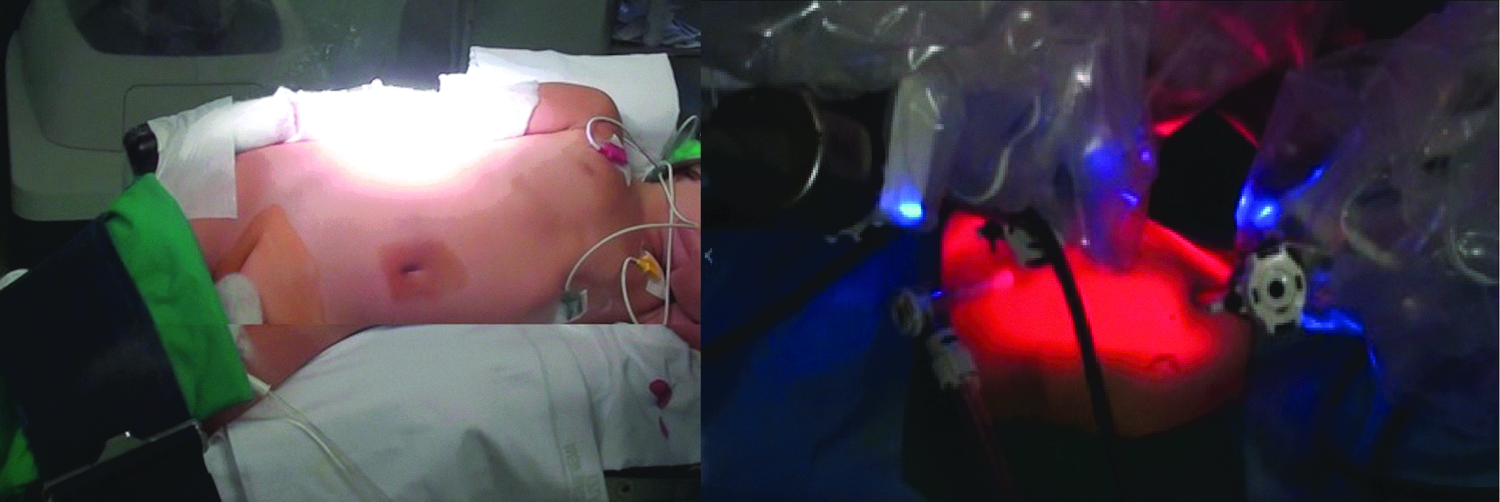
The “docked” robot on patients of the two sizes compared. Male under 15 kg, who underwent nephrectomy.
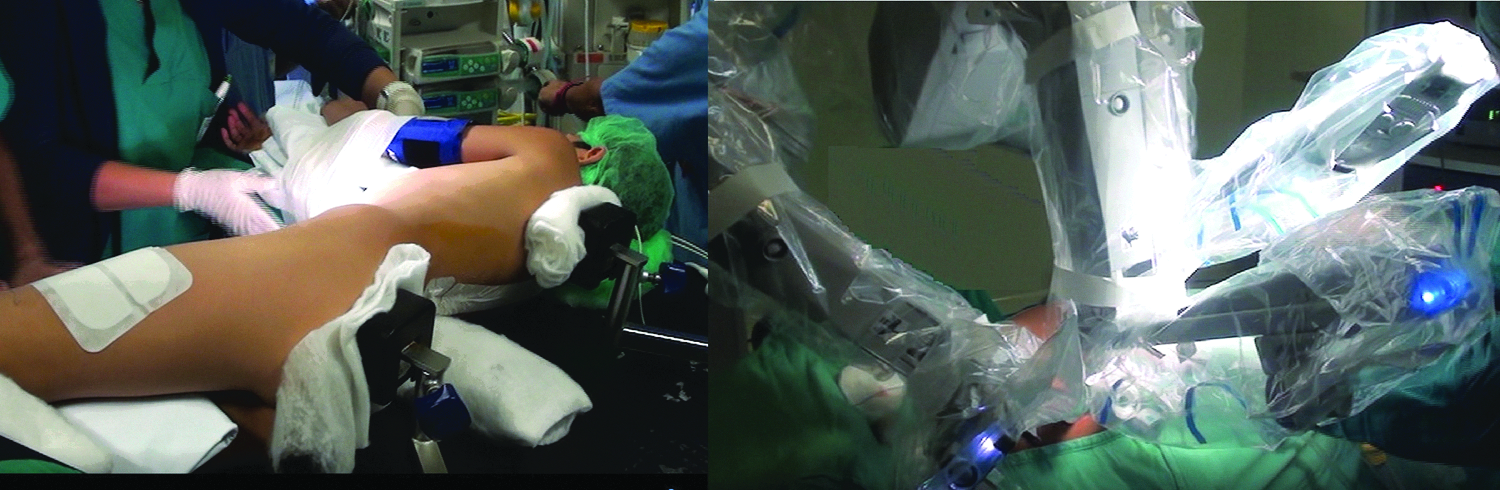
The “docked” robot on patients of the two sizes compared. Male, 26 kg, who underwent pyeloplasty.
Statistical analysis was performed using Mann–Whitney U test (P < .05). In addition, the correlation between postoperative conversion rate and short-term complications was assessed using Fisher's exact test (P > .05).
Results
The total number of patients analyzed was 83, 41 females and 42 males. Of these, 55 were in group A (children with intervention weights >15 kg) and 28 in group B (children weighing ≤15 kg). The demographic characteristics of the population studied, with special attention to weight's data, are summarized in Table 1. Table 2 shows the distribution of pathologies that have placed indication for surgical intervention.
Characteristics of Studied Population
Distribution of Pathologies That Have Placed Indication for Surgical Intervention Divided into Two Groups by Weight Cutoff
Mean times at console were, respectively, group A, 60 minutes, and group B 70 minutes. Statistical analysis did not show a statistically significant difference. Conversely, the study of the total time of surgery has shown a statistically significant difference with P value .0408. Average times were, respectively, group A, 122.5 minutes, and group B 160.0 minutes.
Length of hospitalization did not show statistically significant differences. The median times of hospitalization were, respectively, group A, 5.5 g, and group B, 5 days. Conversion cases were in total 7 belonging to group A and 4 to group B. The comparative study of conversion rate of the groups was conducted using the Fisher test, which did not show significant statistical differences, Table 3 shows the main complications found for both groups, in percentages. The comparative study of the two groups in terms of complications was conducted using the Fisher's exact test, which did not show significant statistical differences.
Complications in the Two Groups
Discussion
Robotic minimally invasive surgery has been rapidly adopted for a wide variety of surgical procedures in adult patients across a broad spectrum of surgical specialties. This has occurred despite the high costs and uncertain benefits of surgical robots. Local competitive pressures may be driving the purchase of a robot. Adoption of this technology by a neighboring hospital increases the likelihood of nearby hospitals acquiring a surgical robot. 3 As opposed, Children's Hospitals and pediatric surgical disciplines took more time to embrace the surgical robot. The challenge may be related to the difficulty in possessing a surgical robot in many children's hospitals. In this context, many pediatric surgeons have to share it with adult surgeons. The first robotic Nissen fundoplication was performed in July 2000 and reported in April 2001. Since that time, robotic procedures have been slowly adopted by select pediatric surgical specialists. Many authors suggest that the technical capabilities of the robot may be ideal for complex pediatric surgical cases that require safe dissection. However, due to the size constraints of the robot for small pediatric patients, the tight financial margins that pediatric hospitals face, and the lack of high-level data displaying patient benefit when compared to conventional laparoscopic surgery, it may take some time for the robotic surgical platform to be widely accepted in pediatric surgical practice. In the following decade, there were a total of 2393 procedures reported in 1840 patients in the published literature. The most common gastrointestinal and thoracic procedures were pyeloplasty, the most common procedure overall, fundoplication, and lobectomy, respectively, with the da Vinci Surgical System (Intuitive Surgical, Inc.) as the most prevalent and most studied robotic platform. 2 This distribution is also present in our series. The pyeloplasty and Nissen fundoplication represent the most represented interventions in our series.
Despite this recent development, the adoption of robotic surgery is less common in the pediatric surgical specialties compared to the adult surgical disciplines.
Supporters of minimally invasive robotic systems have many useful features that include better dexterity, motion scaling, tremor filtration, greater optical magnification, stereoscopic vision, operator-controlled camera motion, and deletion of the effect fulcrum compared to conventional laparoscopy. Wrist laparoscopic instruments used in robotic surgery provide seven degrees of freedom. For the surgeon, these features can allow more precise dissection with greater magnification and visibility. In pediatric surgical procedures, these technical skills can have the potential to overcome the physical capabilities of human performance in the narrow operational fields encountered in children. 3
To date, not many complex procedures are performed in newborn infants with a robotic approach. Its technical requirements may make it ingenious or unworkable for smaller patients. The manufacturer of the Vinci Surgical Robot recommends a distance of 8 cm between each door. This can be difficult to obtain in many neonatal cases. Many of the pediatric surgical problems concern neonatal cases, in which a congenital malformation is present. These limitations therefore risk to exclude a good portion of pediatric surgical patients. In our series, in fact, there are no cases in which the robotic approach has been chosen to treat congenital diseases in the neonatal age.
The size and the length of the instruments can also be a problem. Neonatal surgical procedures are often performed with 3 mm instruments and endoscopes, which are smaller than the smaller tools and endoscopes currently available for robotic surgery. Currently, two endoscopes for the Vinci Surgery are available: 12 mm 3D and 8.5 mm 3D. 2
The instruments are available in two sizes: 8 and 5 mm. The 8 mm instruments are articulated with a roll-over punch mechanism, while the 5 mm instruments are articulated similar to a snake. The difference in the joint brings the 5 mm instruments longer than the corresponding 8 mm, losing the working area within a small body cavity. As showed by Ballouhey et al., in light of better performances with 8 mm tools for specific tasks and parietal sparing constraints in restricted spaces, 5 mm instruments can be deemed to be less effective for reconstructive procedures in small children. 4 Some authors have stated that 5 mm instruments offer advantages in regard to pediatric patients, due to their smaller diameter and the finer needle forceps for grasping. This advantage has been clearly demonstrated for pediatric thoracic surgery, where there is a limited width in regard to the intercostal space. 5
For infants and young children, 3 mm instruments are commonly used for many basic and advanced laparoscopic procedures. In our department, we are used to operating patients with a small size and weight, especially newborns, with 3 mm instruments, when the minimally invasive approach is chosen. In our department, when choosing minimally invasive approach, we used to operate patients with a small size and weight, especially newborns, with 3 mm instruments. The lack of 3 mm instruments available on the market represents a significant limitation of existing robotic surgical platforms and a disincentive for their use in small children. Finally, there are a limited number of tools to choose from. The absence of 3 mm and the few options for 5 mm instruments can limit the use of robots in infants and children. The patient benefits of robotic surgery are thought to be essentially the same as conventional laparoscopy: decreased length of stay, decreased blood loss, decreased pain, quicker return to work, and improved cosmetic result through smaller incisions. In pediatric urology, there is evidence that robot-assisted pyeloplasty may be superior to open and laparoscopic approach with decreased length of stay, decreased narcotic use, and decreased operative times. 6 The total conversion rate from open to open procedure is low. It has been reported as 2.5% in a meta-analysis of robotic pediatric surgery. This is comparable to the conversion rate in conventional minimally invasive pediatric surgery. However, the real conversion rate for robotic pediatric surgery may be higher due to quotation bias. 2
In this article, we evaluated if low-weight patients could be considered feasible for robotic surgery or if could be a weight to be considered a cutoff value for a robotic intervention. This consideration stems from the observation that with the growth of our robotic experience, we have treated children of even smaller size and weight. The parameters we considered did not show a significant difference between the two groups, except for the surgery time. The total time of surgery was shorter in the group of patients who weighted >15 kg, suggesting an easier procedure due to a bigger abdominal space and consequently easier trocar insertion. We also have a higher practice regarding surgery in patients weighing more than 15 kg, with better learning curves that translate into lesser operating times. In the group of patients weighing less than 15 kg, operating times were longer due to a more complex docking and a learning curve that still needs to grow for this type of intervention. Robotic surgery could have the possibility to overcome the problem of improvement in surgical learning curve in an easier and faster way than laparoscopic surgery. 7
The technical difficulty and steep learning curve of laparoscopic surgery have contributed to the growing popularity of robot-assisted surgery (RAS). Da Vinci Surgical System (Intuitive Surgical) provides the advantages of simplification and precision of exposure and suturing because of allowing movements of the robotic arm in real time with increased degree of freedom and magnified 3D view. RAS has the potential to make laparoscopic surgery more accessible to pediatric surgeons and simplify complex intervention, as it was in pediatric urology for upper urinary tract reconstructive procedures. RAS, initially used for pyeloplasty and nephrectomy, can be used to perform ureteral reimplantation and more complex reconstructive surgeries, including bladder augmentation and antegrade continence enema. One disadvantage of conventional pediatric laparoscopy and RAS is the need for multiple incisions that are significant in size with relation to patient size. Single-incision laparoscopic surgery may be advantageous in children, but experience with these novel techniques remains in its infancy. 4
Robotic surgery is the new step in evolution of minimally invasive surgery. Many studies have been published, but these are often case reports or small series. Our series was one of the biggest in Italy, collecting patients from two centers. The initial results of robotic surgery in the field of pediatrics are encouraging. The success rates of robotic procedures seem identical to those of conventional laparoscopy. However, there is no randomized study currently available for children in the literature. Meehan et al., in their large series of 100 cases of pediatric robotic surgery, described 22 patients who weighed less than 10.0 kg, with a cutoff of 2.2 Kg. They explained that small patients, even patients less than 5 kg, can have many different procedures accomplished with excellent results. However, space becomes a significant issue in children less than 3 kg, particularly in the chest. 8 This has also emerged from the study of our series. Valuation of the distribution of thoracic surgery interventions shows that the largest part of them has been performed in patients weighing more than 15 kg. Although not statistically significant, this figure confirms, also in our study, what emerges from the literature.
Further prospective and comparative studies, especially comparisons between robotic and laparoscopic approaches, are necessary to confirm these preliminary results. Economic analyses are also indispensable to ensure the viability of robotic technology. 9 In addition, robotic surgery can be combined with new concepts such as virtual reality or augmented reality, which provide valuable preoperative or intraoperative information for the surgeon. Pediatric surgeons must be actively involved in the evolution of robotics to ensure a suitable and reasoned use of this new technology for their young patients. 10
Conclusion
Retrospective analysis of our series shows that weight cannot be considered an absolute limit for robotic surgery. The improvement of instruments permits to perform complex surgical procedures in low-weight children without additional difficulties. However it is important to report that the smallest child of our group weighed 7 kg, without neonatal cases. Extending robotic surgery to this latest type of patient is the challenge for the future of mini-invasive pediatric surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.