
Abstract
Abstract
Background:
Congenital recto-urethral fistula (RUF) is the most common form of anorectal malformations (ARMs) found in boys. The aim of this study is to review our experience with one-stage laparoscopic procedure in the management of ARMs with recto-prostatic fistula and recto-bulbar fistula.
Methods:
Seventeen boys with congenital RUF who underwent one-stage laparoscopy-assisted anorectoplasty (LAARP) between July 2012 and June 2015 were retrospectively in the study.
Results:
All patients successfully underwent one-staged laparoscopic surgery without conversion. The recto-prostatic urethral fistula was encountered in 6 patients and recto-urethral bulbar fistula in 11 patients. The mean age at the time of surgery was 46.2 hours with mean length of hospital stay being 10.6 days. The operative times for the recto-urethral prostatic fistula and recto-urethral bulbar fistula were similar (128.2 versus 122.4 minutes, P = .091). Intraoperative blood loss was minimal. No injury to the urethra or vas deferens. The urethral catheter was removed on postoperative day 10. No one lost to follow-up. The median follow-up period was 2.6 years (range: 2–4 years). No recurrent fistula or urethral diverticulum was detected according to the voiding cystourethrography and pelvic MRI at 1 year.
Conclusion:
One-stage LAARP is safe and effective for neonates with recto-prostatic fistula and recto-bulbar fistula. It provides an alternative method to rectify the ARMs with recto-prostatic fistula and recto-bulbar fistula without colostomy.
Introduction
C
Materials and Methods
The outcomes of one-stage laparoscopic management of RUF performed in our center over the previous 4 years were reviewed. The procedures were performed by the same surgeon team. All patients were regularly followed up in our clinic 1, 3, 6, and 12 months postoperatively and 6 months thereafter. Physical examination, pelvic MRI, and a voiding cystourethrogram were carried out. Data were collected and analyzed using SPSS 21.0 package.
Patients
Seventeen neonates with congenital RUF underwent one-stage laparoscopic repair during the neonatal period from July 2012 to June 2015. We have to explain that it does not entirely dependent on us to perform one-stage laparoscopic repair, because most of ARM newborns undergo a colostomy before being transferred to our center. Hence only for those newborns transferred to us directly after birth, can we perform one-stage laparoscopic corrections without colostomy. The preoperative invertograms, voiding cystourethrogram and pelvic MRI were used as routine methods to identify the location of fistula. The chest X-ray, spine X-ray, abdominal ultrasonography, and echocardiography were used to assess the patients' condition preoperatively. Ethics approval from the Ethics Committee of the Capital Institute of Pediatrics was obtained. Written informed consents were obtained from the parents before the surgery.
Operative technique
The patient was placed in Trendelenburg position. CO2 pressure was maintained between 8 and 12 mmHg. The bladder was emptied by a urinary catheter. The single-incision laparoscopic surgery (SILS) procedure was performed on these 17 infants. First, a right semicircular umbilical incision was made and extended 0.5 cm above and below the umbilicus, along the midline. The total incision length was 2.5–3 cm. The sigmoid colon was exteriorized through the umbilical incision. A 1-cm longitudinal incision was made along the antimesenteric border of the proximal sigmoid colon. A rectal tube connected to a syringe was inserted into the colonic incision to remove and suction off the meconium within colon (Fig. 1), and then the colonic incision was closed with absorbable sutures. A fine needle connected to a syringe was used to release air within the distended small intestine (Fig. 2). After this, the umbilical incision was then partially closed with absorbable sutures. A 2-cm vertical umbilical incision was left open, and three trocars were inserted into the abdominal cavity through this same incision (Fig. 3).
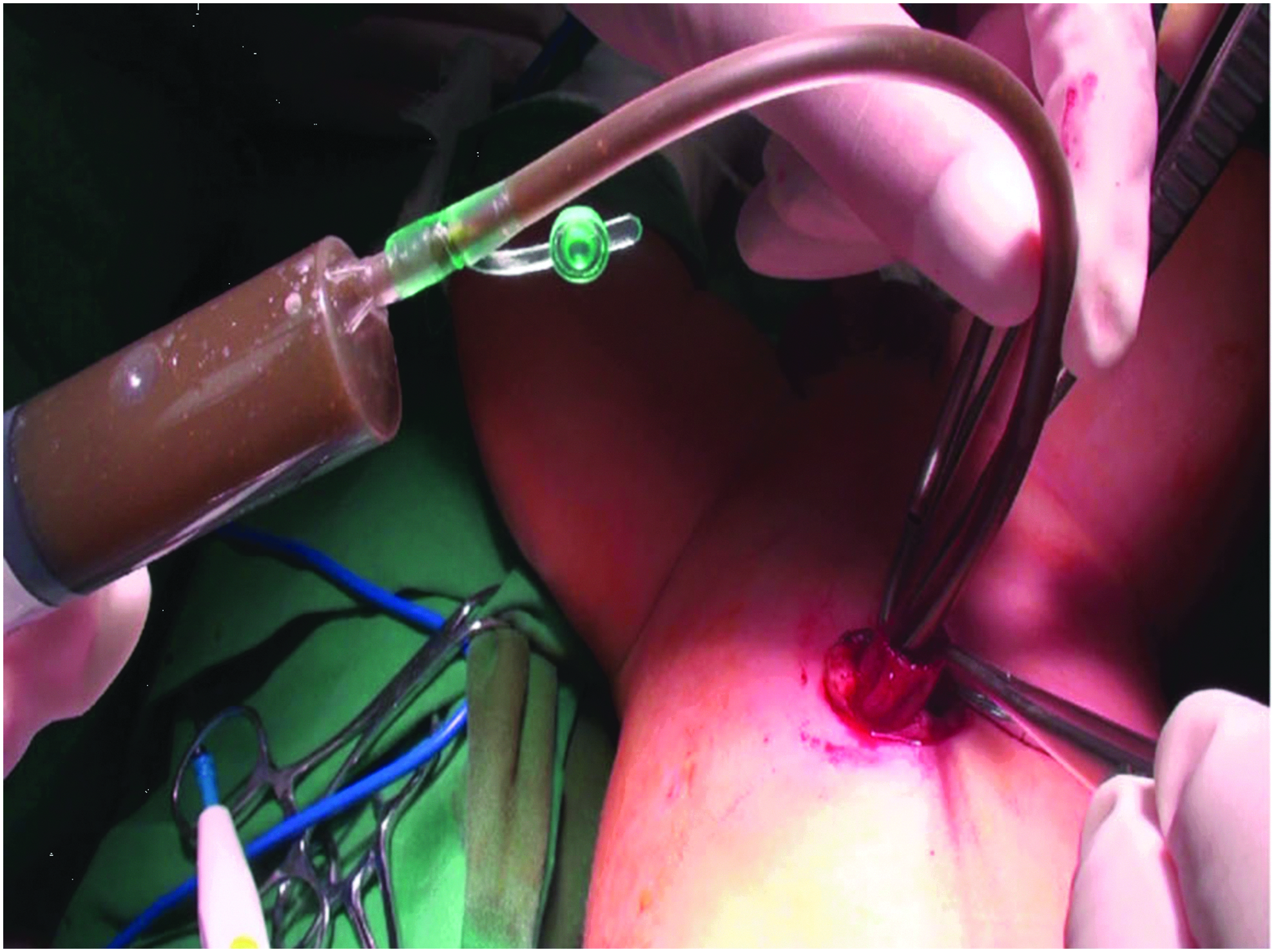
In order to remove the meconium, a 16F rectal tube that was connected to a syringe was inserted through sigmoid colon incision, repeated saline irrigation and suction in the distal the proximal side until the meconium was cleaned out.
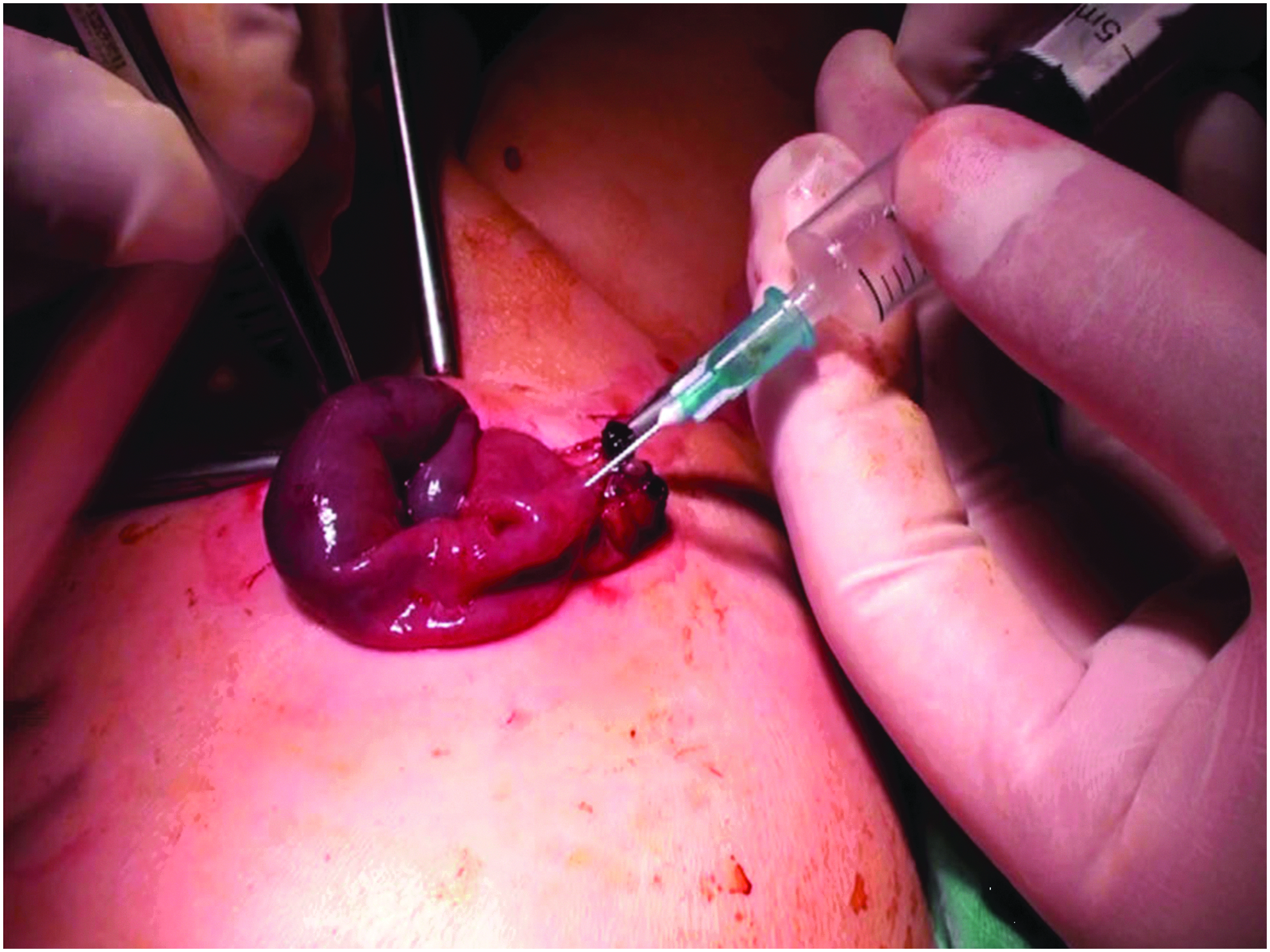
A 5-mL syringe with 1-mL syringe needle was punctured into the distended intestines to release the gas.
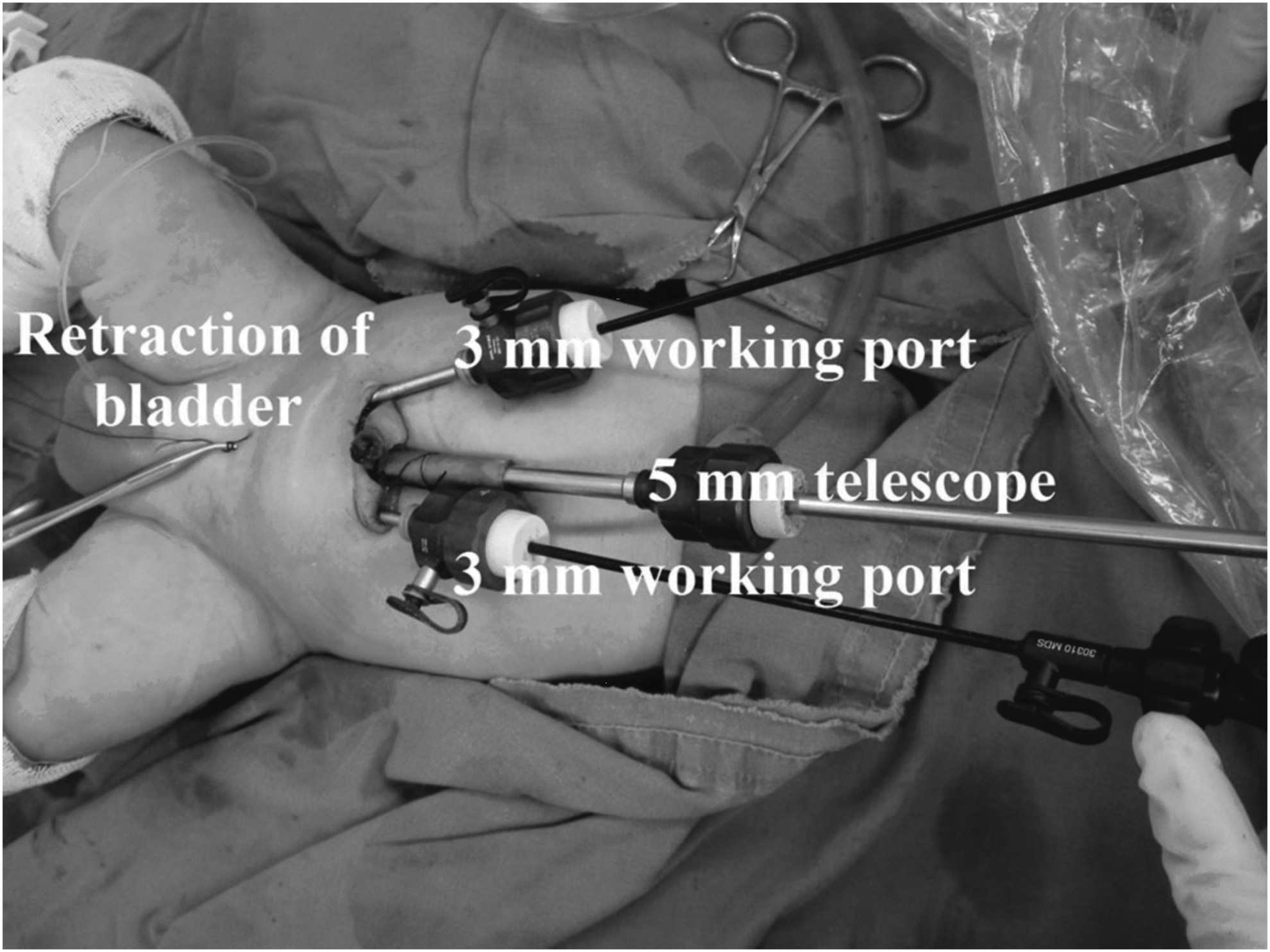
The arrangement of the working instrument, and a trans-abdominal suture was used to retract bladder.
Rectal dissection began at the peritoneal reflection. The distal rectum was mobilized along the plane between posterior urethra and rectal pouch, close to the rectal wall. The rectal blind pouch was pulled up to expose the fistula. The dissection of distal fistula was performed along submucosal layer to a level 0.5-cm proximal to the urethra. The mucosa was dissected to the most distal point and completely transected flush with the posterior urethra. The 0.5-cm remnant muscular cuff of the fistula was ligated with Hem-o-lock clip or 5-0 PDS suture according to the location and length of fistulae. For the patients who had narrow and long fistula length (> 0.5 cm), which were located in relatively shallow pelvis, the stump of muscular cuff was ligated by Hem-o-lock clip (Fig. 4). For those patients with wide and short fistula length (≤0.5 cm) or the fistula located in deeper pelvis (no adequate space allowing 5 mm Hem-o-lock to work), the stump of fistula was closed by 5/0 PDS horizontal running suture (Fig. 5). The distal rectum was ligated before pull-through to minimize fecal contamination in the pelvic cavity. Then, the blunt artery forceps was used to create the potential tunnel through the center of the sphincter complex under the laparoscopic guidance.
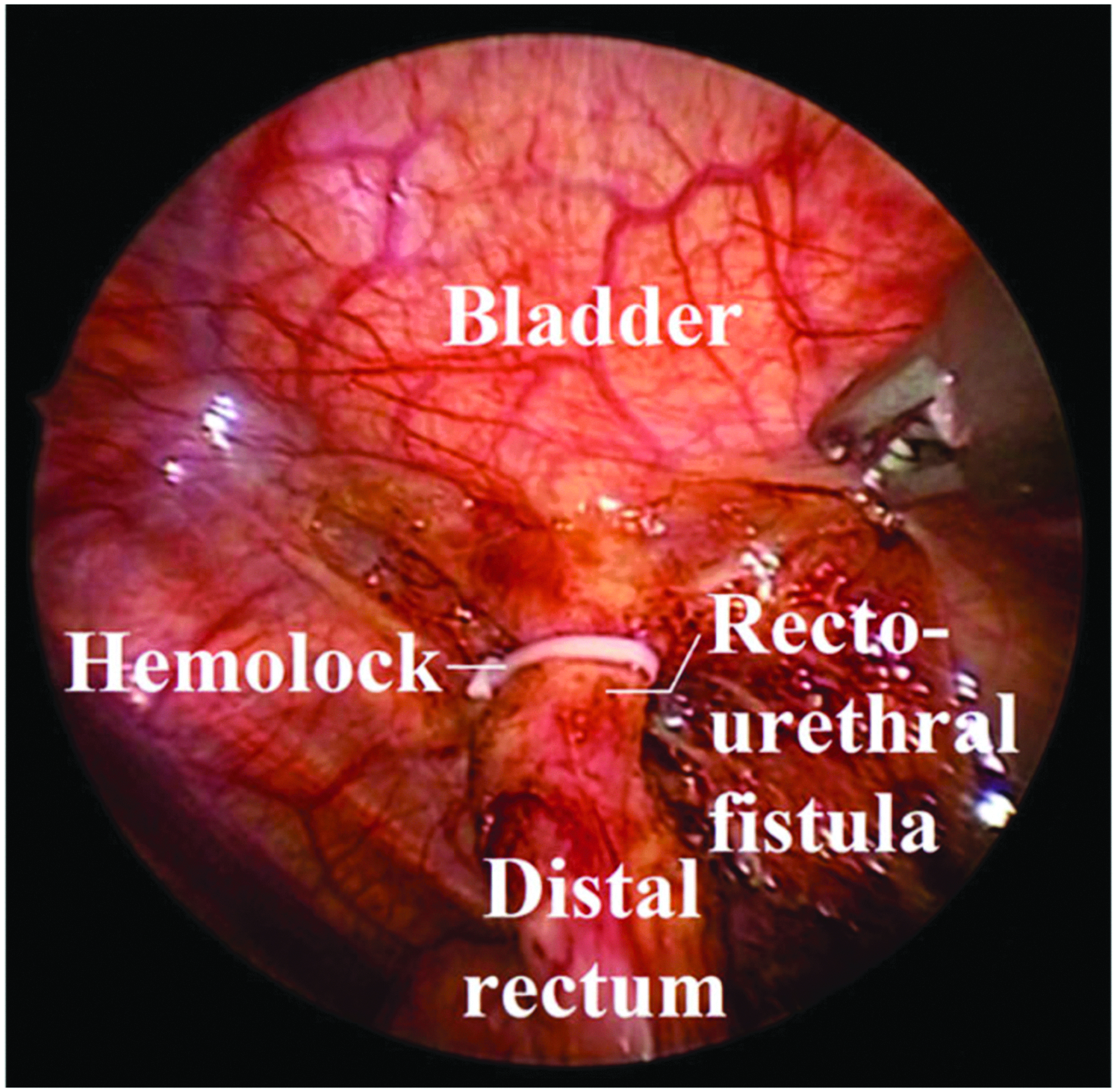
The stump of fistula was closed by Hem-o-lock in a boy with recto-urethral fistula.
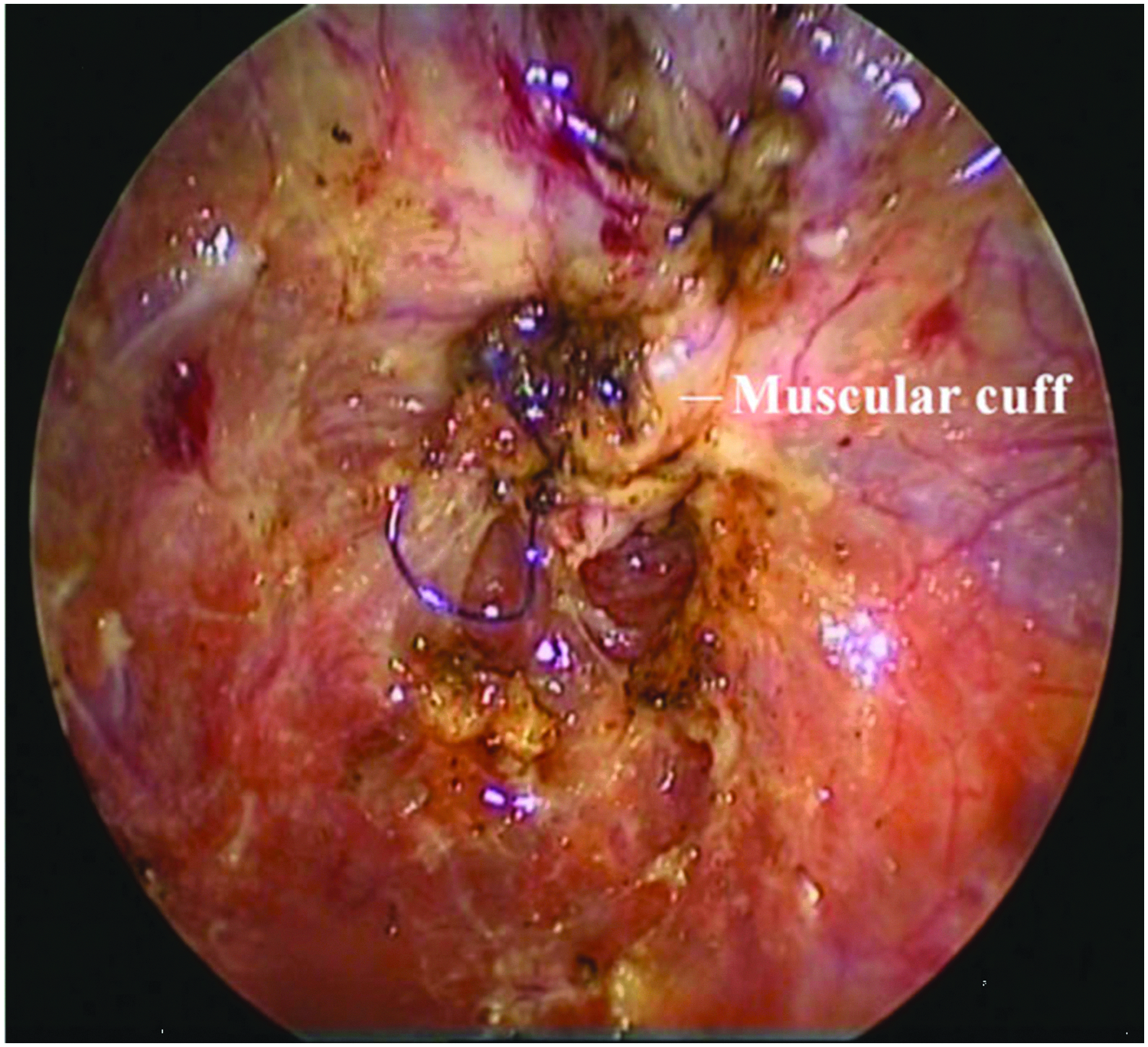
The remnant muscular cuff of fistula is closed by 5-0 PDS horizontal running suture.
The rectal blind pouch was then pulled down through the tunnel muscle complex to the perineum without tension. The grossly dilated distal rectum was excised. Anoplasty was conducted with absorbable interrupted 5/0 PDS sutures between the rectum and perineal skin.
Results
All patients successfully underwent one-stage SILS. The average gestational age was 38.76 ± 1.70 weeks (37–40 weeks). The mean body weight was 3.51 ± 0.22 kg (2.80–4.00 kg). The average total operative time was 125 ± 22 minutes. The mean age at the time of surgery was 46.2 (range: 25–70 hours). Rectal-prostatic urethral was encountered in 11 patients and recto-urethral bulbar fistula in 6 cases. The associated anomalies are depicted in Table 1. The mean operative times for the urethral-prostatic fistula and urethral-bulbar fistula were similar (128.2 versus 122.4 minutes, P = .091). The detailed information is shown in Table 2. No injury of urethra or vas deferens occurred during the operation. The urethral catheter was removed on postoperative day 10. No patients experienced recurrent fistula and urethral diverticulum in either group according to postoperative voiding cystourethrogram and MRI. Ten of 17 neonates underwent excision of grossly dilated distal rectum, and the distal rectal specimens were collected for histopathologic examination. Hypoplastic hypoganglionosis in the submucosa layer (Fig. 6) and muscularis propria (Fig. 7) was confirmed by hematoxylin and eosin (H&E) staining.
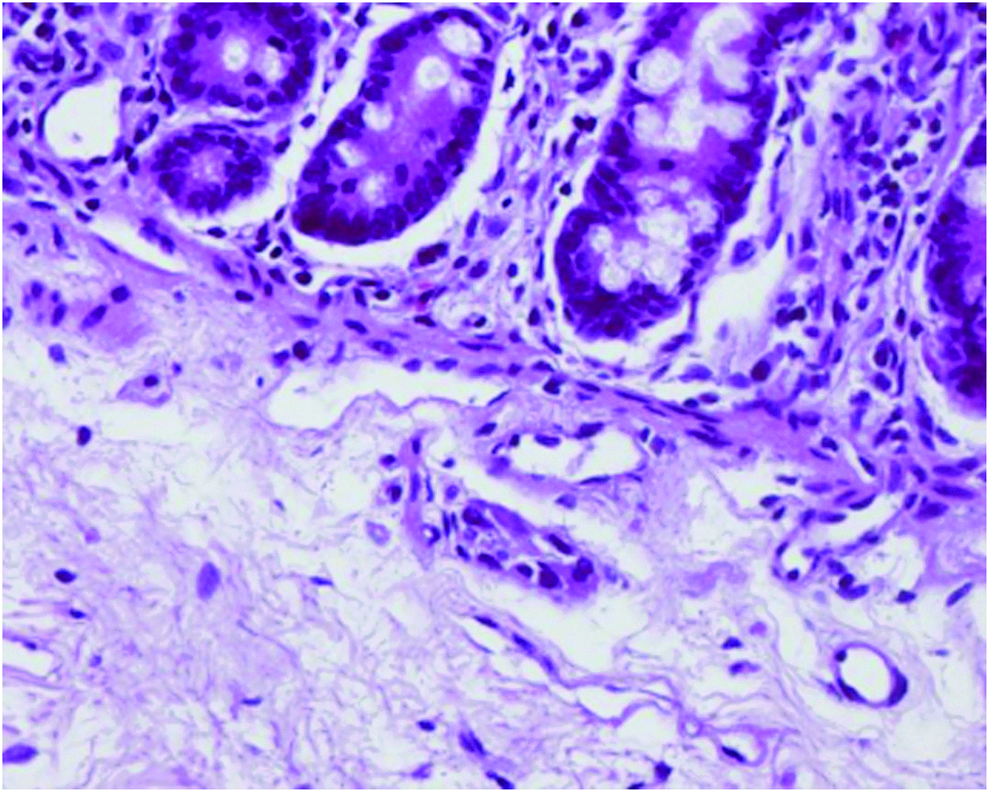
Hypoplastic hypoganglionosis in the submucosa layer.
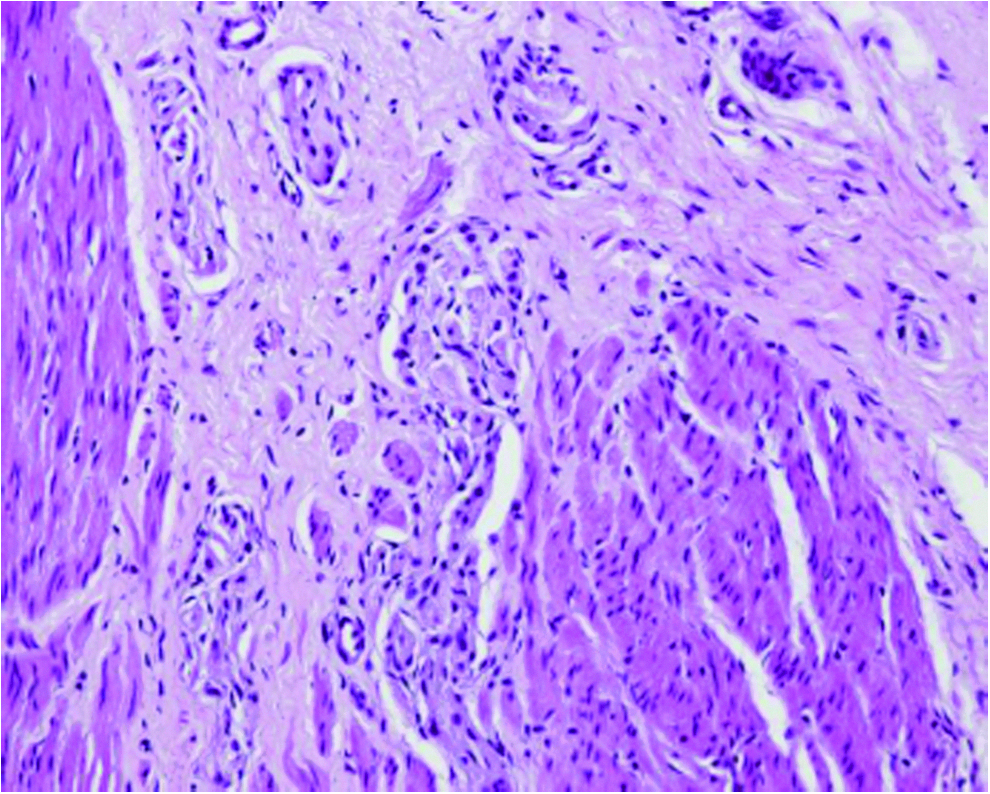
Hypoplastic hypoganglionosis in the muscularis propria.
Follow-up
All patients were followed up. The median follow-up period was 2.6 years (range: 2–4 years). The cosmetic appearance of abdomen and neoanus was shown in (Fig. 8), no obvious scar was observed at follow-up. The rectum was placed centrally within the pelvic muscle complex according to the postoperative MRI. No patients underwent rectal retraction or prolapse, and anal stenosis during the whole period of follow-up. Two patients experienced constipation, which could be treated with a transient course of oral laxatives for 1 month. The 2 patients had sacral anomalies among which one had Grade II soiling and the other had Grade III soiling on follow-up, and the method of intermittent enema allows the patients to be clean of stool.

Cosmetic appearance of abdomen and neoanus; no obvious scar was observed at follow-up.
Discussion
The conventional LAARP procedure is divided into three stages of colostomy, LAARP, and followed colostomy closure. Since the widespread application and constant advances in neonatal and laparoscopic technique, the staged procedure has been challenged. Nowadays, there are many reports on one-stage posterior sagittal anorectoplasty (PSARP) to treat the neonates with ARMs.4–6 Nevertheless, literature related to one-stage LAARP for ARM was rare. Many pediatric surgeons7,8 reported the technique of one-stage LAARP for high imperforate anus. The technique of laparoscopic surgery has the advantages of magnified, minimal surgical trauma, precise identification of the anatomical structures, and exact distal rectum placement within the muscle complex. There are also some obstacles we have to overcome in the application of one-stage LAARP: (1) how to distinguish the types of malformations and recognize the precise location of rectal pouch without a colostomy; (2) how to operate in a very limited working space because of dilated bowel and relatively small abdominal cavity; (3) how to decompress the meconium and air from the bowel; (4) it is difficult to repair the recto-urethral fistula situated in the pelvis.
As for how to distinguish the types of malformations and recognize the precise location of rectal pouch without a colostomy, our experiences demonstrated that preoperative invertograms, urethrograms, and pelvic MRI can be used as routine methods to identify the fistula easily. A successful retrograde urethrocystogram can precisely locate the fistulae, whereas if the fistulae is very narrow and may be obstructed by meconium, a urethrogram may be not effective. The fistula mucosa can be accurately identified according to MRI, as the fistula was always located where the fistula mucosa disappeared if the MRI sometimes maybe not clear. We can also know the development status of the pelvic musculature preliminarily from the MRI, predicting the postoperative anorectal function to a certain extent. To decompress the dilated bowels, we make a small incision at the proximal sigmoid colon to decompress meconium and air from the bowel to create adequate working space without a colostomy. Our previous method of enema was inserting a urethral catheter into the distal rectum through the recto-urethral fistula and puncturing the distal rectal pouch by trans-abdominal under guidance of the laparoscope to decompress bowel. 7 However, neonates with RUFs may pass meconium through the urethra, usually after 20 hours of life, which is an unequivocal sign of RUF. The previous methods lead to a urinary tract obstruction and acute urine retention due to the residual fecalith occasionally. We make the first attempt to decompress the meconium intraoperatively through a small temporary colonic incision, and then the meconium was removed with repeated saline irrigation and suction. The incision was subsequently closed with absorbable sutures. The colonic decompression incision not only plays a role of a distal stoma enema in the procedure of three stage anorectoplasty, but can also be conveniently transformed into a colostomy if needed. Hence, we think that it is safe and effective to decompress meconium intraoperatively through a temporary colonic incision. In addition, a 5-mL syringe that connected to a needle was used intraoperatively to puncture the distended small intestine and release air to create an adequate space.
The technique of SILS was also utilized in the operation. The SILS has been utilized in the treatment of ARMs in our center since 2011. 9 The SILS represents the recent improvement in laparoscopic surgery with the advantages of better cosmetic result than conventional laparoscopic surgery. 10 It is a challenge for laparoscopic surgeons to perform SILS procedure because the placement of a camera and several instruments parallel to each other result in decreased freedom of motion and “conflict” of instruments. Our experience shows that inserting trocars parallel to each other through the umbilicus incision is particularly suitable for newborns. Because the pelvis in neonates is relatively small and shallow, the parallel placement of instruments will facilitate performance of surgery in such a small space. In addition, the newborns' abdominal muscle and fascia is immature, and this will increase the motion of instruments to some degree. The following measures were further utilized to facilitate repair of the recto-urethral fistula. The method of transabdominal suture retraction through posterior bladder wall was conducted to extend the space, and the rectal blind pouch was pulled up to the abdominal cavity to identify the RUF. The telescope was rotated by 180° to facilitate complete exposure and meticulous ligation of the fistula, and to prevent the occurrence of rectal prolapse, the distal rectum should not be dissected excessively. In addition, adequate experience accumulation of laparoscopy and acquisition of learning curve is essential for SILS. There must exist a potential tunnel in the center of the striated muscle complex. Hence, it is extremely important to pull the rectum through the center of the striated muscle complex without any resistance, thus it can effectively reduce the incidence of anorectal prolapse or stricture. The tunnel of sphincter muscle complex should better be moderate enough to allow the rectum to be pulled through without any resistance; otherwise, it can easily result in narrowing not only at the ano-cutaneous junction but also at the deeper level. It is relatively convenient and easy to perform one-stage LAARP in newborns because of the abovementioned advancement in techniques.
It is noteworthy that the leakage from the sigmoid colon incision is a rare but devastating complication after one-stage LAARP. The neonates who underwent one-stage repair surgery defecate from the neoanus immediately after the procedure because there exists no colostomy. If an anastomotic edema and poor rectal function occurred at an early stage after operation, then followed by abdominal distension and decreased bowel motions, risk of leakage from the sigmoid colon incision increases. Hence, the postoperative rectal tube placement is extremely vital for the one-stage procedure. Our practice of placing an 18F rectal tube to stent the edematous anastomotic sites until regular bowel movement was resumed.
Most surgeons believed that the risk of wound infection and dehiscence will increase due to the absence of colostomy in one-stage procedure as a fecal diversion route and direct contact between the surgical site and fecal material after surgery, and it will lead to devastating outcomes such as incontinence and anal stricture. But we think that since the patients are neonates, there is no bacterial contamination in the blind pouch of the rectum. Hence, it will not increase the risk of wound infection under the one-stage procedure theoretically. There were no complications such as anal wound infection, dehiscence, rectal retraction, or anal stricture encountered in our series during the follow-up. And many surgeons divided and ligated the fistula at some distance from the urethra to prevent the injury of urethra and urethra stenosis. It is reported that the incidence of posterior urethral diverticulum might increase with the application of laparoscopy in the treatment of ARMs. 11 Pandey et al. 12 reported the approach of dividing fistula without ligation may prevent posterior urethral diverticula.
The procedure of dissecting the fistula where adjacent to urethra is a technically challenging step and should be meticulous in the laparoscopic approach. In our study, no patients underwent urinary diverticulum or recurrent recto-urethral fistula according to the postoperative voiding cystourethrogram.
In our series, 14 patients started spontaneous bowel movement at postoperative day 1–2, but the rectal tubes were still left in situ for 7 days to avoid leakage from the sigmoid incision. The other 3 patients resumed regular spontaneous bowel movements through 1 to 2 months of intermittent enema, and the rectal tubes were left in situ for more than 10 days. Two of them had varied degree of soiling until time for next enema. The rectal administration of this intermittent enema allows the patients to be clean of stool. The presence or absence of sacrum and its characteristics is the most important factor to determine the functional prognosis for bowel control, 13 the 2 patients who had grade II soiling and the other who had grade III soiling on follow-up had sacral anomalies in our series.
According to several reports,14,15 one-stage repair procedure can result in better continence rates, it may be explained by better brain-anal reflexes development right from the time of birth. It has been suggested that the neuronal framework for normal bladder and bowel function exists at birth. But there is a learning or “training” period when long-lasting, activity-driven, neuronal changes take place during neuronal circuitry development. If definitive repairs are delayed, critical time may be lost during which neuronal networks and synapses would have formed to develop normal rectal function.16,17 So the early restoration of gastrointestinal continuity is beneficial to train the function of perineal musculature and improve long-term anorectal function.
In addition, the 10 patients who underwent excision of grossly dilated distal rectum all had good bowel control outcome, maybe the resection of distal abnormal tissue is beneficial to improve anorectal defecation function. The distal rectum specimens in those 10 patients had hypoplastic hypoganglionosis in the submucosa layer and muscularis propria confirmed by H&E staining, we analyzed that the postoperative intestinal motility will not be influenced by the abnormalities neuromuscular structures for it had been resected. It is reported that the postoperative dysmotility may be explained by the malformed segments in ARM. 18
Several drawbacks also existed in our study. First, this study is retrospective, the results may have confounding bias. Second, the follow-up period is relatively short. Long-term results in patients with ARMs depend not only on the level of the rectum, histology of the blind pouch, intensity of preparation of the pouch, but also on the quality and characteristics of the sacrum, which has a definite influence on the final functional prognosis. So the evaluation of bowel function may be biased influenced by these factors. A large-scale, prospective, comparative study is warranted to evaluate its safety and efficacy.
Conclusions
Our results demonstrated that one-stage LAARP is safe and effective for neonates with recto-prostatic fistula and recto-bulbar fistula. It provides an alternative method to rectify the ARMs with recto-prostatic fistula and recto-bulbar fistula without colostomy.
Footnotes
Authors' Contributions
Hui Xiao carried out the entire procedure including the literature search, data extraction, statistical analysis, drafting of the article, and revision of the submitted article. Long Li and Mei Diao conceived the study, coordinated and participated in the entire process of drafting and revision of the article. Rui Huang, Xiang-hai Ren, and Long Chen contributed to statistical analysis and revision of the article. Hui Xiao and Long Li contributed to revision of the article. All authors have contributed significantly. All authors read and approved the final article.
Disclosure Statement
All authors have no conflicts of interest or financial ties to disclose.