
Abstract
Abstract
Background/Purpose:
The Nuss procedure to correct pectus excavatum is associated with severe postoperative pain. The purpose of this retrospective study was to compare pain management outcomes of thoracic epidural analgesia and continuous infusion of local anesthetic (CILA) with and without preoperative self-hypnosis training (SHT) after Nuss procedure (4 treatment groups).
Methods:
Between February 2010 and December 2013, 24 of 53 adolescents who underwent Nuss procedure received SHT. Of these, 16 received thoracic epidural analgesia and 8 received CILA postoperatively. Of the 29 patients who did not receive SHT, 19 received thoracic epidural analgesia and 10 received CILA. All patients received intravenous patient-controlled opioid analgesia and intravenous nonsteroidal anti-inflammatory drugs (IVNSAIDs) and then were transitioned to oral opioids and NSAIDs. Postoperative mean and maximum pain scores, opioid (morphine equivalents) use and side effects, and hospital length of stay (LOS) were compared between groups.
Results:
Patients who received SHT reported lower mean (P = .0047) and maximum (P = .0028) pain scores and used less morphine equivalents/hour over time (P = .046) compared to patients who did not receive SHT. Patients who received thoracic epidural analgesia reported lower mean (P = .0092) and maximum (P = .0083) postoperative pain scores and used more morphine equivalents/hour (P = .01) compared to those who received CILA. In addition, patients who received SHT and CILA had shorter LOS (P = .0013) than patients who received thoracic epidural analgesia without SHT.
Conclusions:
SHT before pectus excavatum repair by Nuss procedure results in less postoperative pain and requires less morphine equivalents over time for postoperative pain management. Opioid-sparing CILA, when paired with SHT, results in shorter LOS.
Introduction
P
Continuous infusion of local anesthetic (CILA) at the surgical wound site may also provide effective pain management after Nuss procedure. 29 Compared with thoracic epidural anesthesia, CILA was associated with decreased pain and opioid use in adults after thoracotomy, 30 but no difference was found after Nuss procedure. 31 In a retrospective study comparing postoperative CILA to thoracic epidural analgesia for children's postoperative pain, there was also no significant difference in reported pain, time to ambulation, or recovery of postoperative ileus. 32
We previously examined preoperative self-hypnosis training (SHT) as an effective adjunct for managing pain after Nuss procedure. 33 Our initial experience in a small pilot study demonstrated that SHT resulted in less pain and an opioid-sparing effect when paired with thoracic epidural analgesia to manage postoperative Nuss procedure pain. 33 In this retrospective study, we extended our previous work to examine the potential benefits of SHT paired with either thoracic epidural analgesia or CILA as part of a multimodal treatment plan for managing adolescents' postoperative Nuss procedure pain. We tested the hypothesis that patients who received SHT and CILA for postoperative pain management would experience significantly less self-reported pain, use less opioids (morphine equivalents) and experience less opioid-related side effects, and have shorter hospital length of stay (LOS), compared to patients in the other treatment groups.
Materials and Methods
Study design and patients
We conducted a retrospective review of the medical records of all patients 10–21 years of age who underwent Nuss procedure at a free-standing, nonprofit, tertiary care academic children's hospital (Connecticut Children's Medical Center) from February of 2010 through December of 2013 (R.C.B.M., M.N.A., E.D.G; Institutional Review Board approval No. 12-050). Inclusion criteria were as follows: (1) developmental and cognitive ability to self-report pain on a 0–10 numeric rating scale (NRS) and (2) postsurgical care protocol as previously described. 33 Patients were excluded if they were receiving chronic treatment with opioids.
Data extraction
To produce a thorough and complete data set, a data abstraction tool was developed for this study. Deidentified demographic, surgical, and outcome data were extracted from inpatient medical records. Any medication indicated for analgesia was included in the abstraction; and all common drug side effects were also recorded. All patient-reported pain scores documented by nurses in the medical record were abstracted by reviewers. If the medical record indicated that the patient was asleep and a pain score of zero was documented, it was assumed that the patient did not actually give this score and the reviewer was instructed not to abstract that score. Recorded pain scores, analgesic use, and other outcomes related to pain were analyzed in 12-hour intervals from the time the patient was admitted to the postoperative medical-surgical unit throughout the duration of the patient's hospital stay. LOS was defined based on the same postoperative time period. Patients' opioid and intravenous nonsteroidal anti-inflammatory drug (IVNSAID) use was converted to milligrams of morphine equivalents per hour (Table 1).34,35
Amount of drug administered to patient multiplied by the conversion factor equals the equianalgesic morphine equivalency (American Pain Society).34,35
IV, intravenous; PO, oral.
Self-hypnosis training
When scheduled for Nuss procedure, surgeons provided patients with a referral and contact information for preoperative SHT. Patients then self-selected to either receive SHT or not to receive SHT. Scheduling conflicts may have prevented some patients who would have selected SHT from receiving preoperative SHT. Data were analyzed based on actual treatment; therefore, only patients who actually received SHT are included in this treatment group. To distinguish between patients who received and did not receive SHT, outpatient SHT encounters were reviewed in the medical record.
SHT and postoperative self-hypnosis coaching were provided by 1 integrative medicine physician (A.M.V.) in the manner previously described and based on the model described by Lobe.33,36 Preoperative SHT sessions were 60–80 minutes. Sessions began with discussion of patient interests, self-hypnosis goals, and sensory experiences, including prior painful experiences. A formal explanation of hypnosis was then provided. Patients were taught that all hypnosis is self-hypnosis; and patients remain in control during hypnosis. The role of the integrative medicine physician was clarified as teacher and coach, rather than “hypnotist.” Practice of self-hypnosis, including induction, intensification, therapeutic suggestion, posthypnotic suggestion, termination of trance suggestion, and resumption of awareness, was practiced during the second half of the preoperative SHT sessions.
Patients were provided recordings of the preoperative SHT to facilitate additional practice of techniques at home before surgery. There are no records of whether patients practiced these techniques or how often they practiced before their Nuss procedure. Postoperative coaching sessions were provided by the same integrative medicine physician. These sessions took 20–60 minutes and were provided based on patient need and availability of the integrative medicine physician.
Postoperative pain management
Five different pediatric surgeons performed or assisted in the surgical procedures (K.A.R., R.W., C.R., D.H.) for the patients in our study cohort. All surgeons performed this procedure in the manner described by Nuss and Kelly 5 and Nuss et al. 37 Postoperatively, all patients were treated for pain with intravenous patient-controlled opioid analgesia (IVPCA) and IVNSAIDs and then transitioned to oral opioids and NSAIDs as previously described. 33 IVPCA allows patients to self-titrate opioids to reduce disparity in pain management, thus allowing for ethical comparative effectiveness investigations of pain management strategies. 38
Patients received either thoracic epidural analgesia or CILA based on surgeon preference. Thoracic epidural analgesia was provided in the manner previously described and was continuously infused until the 3rd (85–96 hours) postoperative day. 33 CILA was provided through an ON-Q Pump with a Select-A-Flow Variable Rate Controller (ON-Q Pain Relief System; Halyard Health, Inc., Irvine, CA). Once the patient was under general anesthesia and had undergone sterile preparation and draping, bilateral multi-holed, 7.5 cm wound catheters were inserted at the nipple line and tunneled subcutaneously toward the lateral chest wall. At the midaxillary line, the catheters were directed deep to the rib and tunneled along the thoracic cage laterally toward the scapula. They were secured into place at their entry sites with Dermabond and Tegaderm dressing. The catheters were positioned lateral to the surgical incisions and not seen in the wounds during the surgery.
The catheters were primed with local anesthetic (bupivacaine 0.25%) and capped for the procedure. At the conclusion of the Nuss procedure, before leaving the operating theatre, the catheters were attached to a 600-mL fill-volume reservoir, which was overfilled to 750 mL with Ropivacaine 0.2%. Each catheter continuously infused local anesthetic at an average of 4–6 mL/hour to a maximum of 12 mL/hour. The reservoir was refilled every 48–72 hours (before it was empty); and patients were discharged home with the catheters and On-Q pump system in place for up to 9 days after surgery.
Study outcomes
The primary outcome was pain intensity as reported by patients using a 0–10 NRS as documented in their medical records. The secondary outcome was opioid use by IVPCA or oral opioid administration. Other outcomes analyzed were hospital LOS and opioid-related side effects such as nausea, vomiting, constipation, urinary retention, pruritus, sedation, mental status changes/hallucinations, respiratory distress (recorded as respiratory rate <10 breaths/minute or oxygen saturation <90%), and need for supplemental oxygen.
Statistical analyses
The objective of the analysis was to compare self-reported postoperative pain intensity scores, postoperative opioid use, and LOS across 4 treatment groups in patients receiving CILA or thoracic epidural analgesia with or without SHT. Demographic and clinical characteristics were reported as percentages for categorical variables and means and standard deviations for continuous variables. Differences in baseline sample characteristics across the 4 treatment groups were evaluated using one-way analysis of variance (ANOVA) for continuous variables and chi-square tests for categorical variables. Post hoc tests using the Tukey–Kramer method were used to assess pairwise comparisons and further explore differences among means for variables with significant omnibus tests. Mean and maximum pain ratings and calculated morphine equivalents per hour were analyzed across ten 12-hour time periods, up to 120 hours (5 days) after surgery. Change in mean and maximum pain scores and calculated morphine equivalents per hour were modeled and compared across groups and over time using linear mixed effects models assuming an autoregressive covariance structure. Interactions for SHT and either CILA or thoracic epidural analgesia use and time by treatment were also evaluated. In both pain models, a main effect for received morphine equivalents per hour was evaluated. Unless otherwise specified, model P values <.05 were considered statistically significant. To account for multiple comparisons, post hoc analyses using Bonferroni-adjusted P values of .0083 per test were performed for significant effects. Length of hospitalization (hours) was compared across treatment groups using the Kruskal–Wallis test. Pairwise comparisons were then evaluated using the Wilcoxon rank sum test for all possible pairs. All statistical analyses were performed using SAS, version 9.4 (SAS Institute, Cary, NC).
Results
Patient demographics
A total of 53 patients who underwent Nuss procedure between February 2010 and December 2013 were included in the study cohort (Table 2). All patients had a single bar placed during the procedure. Twenty-four patients received SHT and 29 did not. Postoperatively, 8 of the 24 patients in the SHT group received CILA and 16 received thoracic epidural analgesia; 10 patients received CILA only and 19 received thoracic epidural analgesia only. Based on age, sex, race, cognitive ability, and type of pain management received after the Nuss procedure, the cohort comprised a representative sample. The sample was predominantly male (88%) and Caucasian (75%). Sample demographics were similar across groups. The Haller index, a measure of pectus excavatum severity, was significantly different across groups (P = .0149; ANOVA), and pairwise comparisons indicated significant differences between the thoracic epidural analgesia and CILA groups (Diff = 1.26 [0.11–2.42]) (Table 1). The only missing demographic, surgical, or outcome data were the Haller index for 1 patient.
Significantly different groups indicated in bold font.
Statistically significant P < .05.
CILA, continuous infusion of local anesthetic; LOS, length of stay; SD, standard deviation; SHT, self-hypnosis training.
Primary outcome: pain intensity
Significant effects for SHT and postoperative pain management were observed in analyses of mean and maximum pain scores over the study period (Figs. 1 and 2). Patients who received preoperative SHT reported significantly lower mean (−1.72, 95% confidence interval [CI] −2.89 to −0.55, P = .0047) and maximum (−2.27, 95% CI −3.73 to −0.82, P = .0028) pain scores than those who did not receive preoperative SHT. Patients who received thoracic epidural analgesia reported significantly lower mean (−1.51, 95% CI −2.63 to −0.39, P = .0092) and maximum (−1.92, 95% CI −3.33 to −0.52, P = .0083) pain scores compared to those who received CILA for postoperative pain management. There was no significant time effect; and no significant interaction effects for pain were observed.
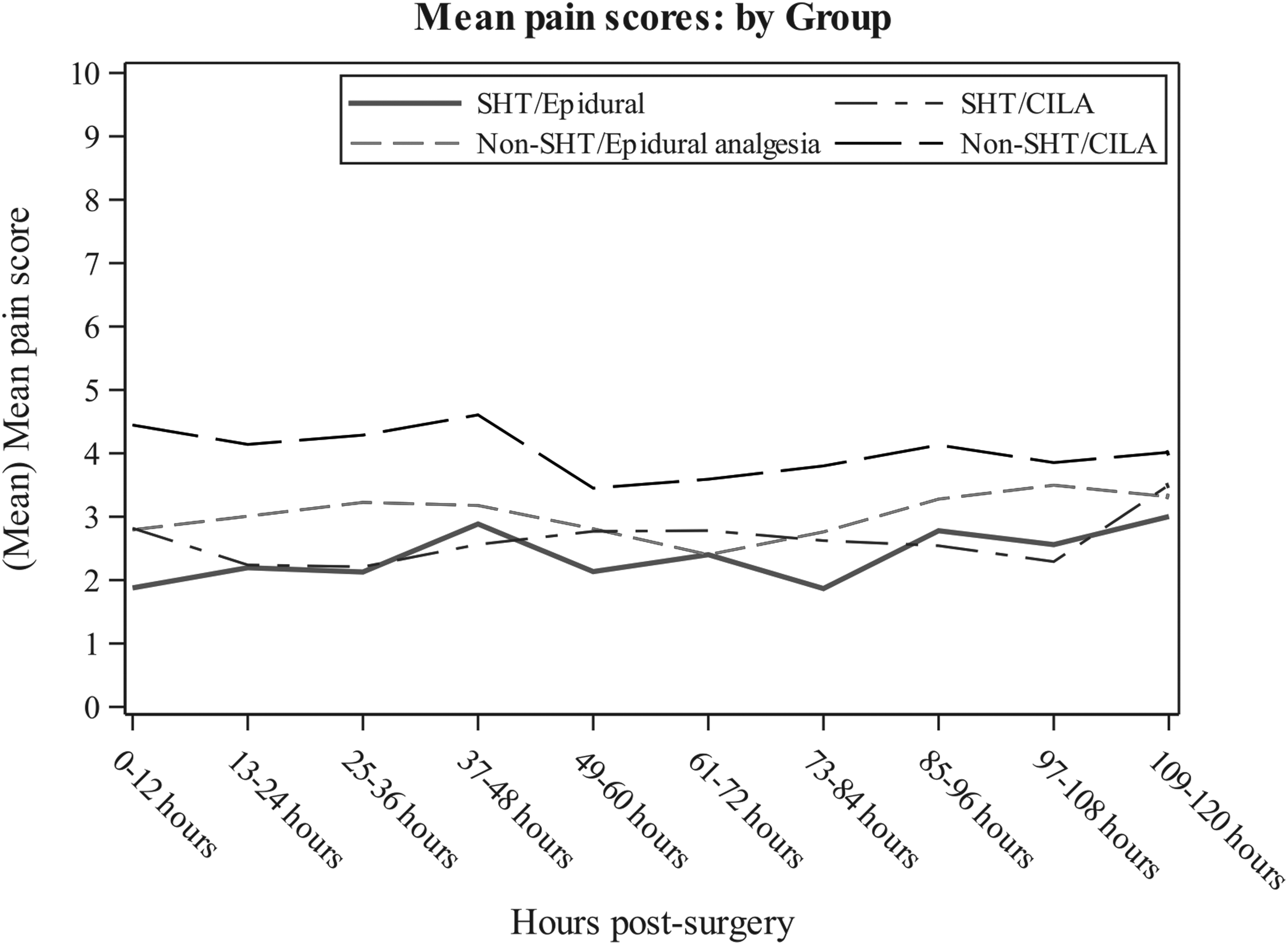
Mean pain scores over time. Plot of mean pain scores reported in 12-hour postoperative intervals for all 4 treatment groups. CILA, continuous infusion of local anesthetic; SHT, self-hypnosis training.

Maximum pain scores over time. Plot of maximum pain scores reported in 12-hour postoperative intervals for all 4 treatment groups. CILA, continuous infusion of local anesthetic; SHT, self-hypnosis training.
Comparisons of self-reported pain intensity scores across the 4 treatment groups indicated that patients who received SHT and thoracic epidural analgesia reported statistically lower mean (P = .0003) and maximum (P = .0002) pain scores than patients who received CILA alone. Two other pain intensity score trends were identified, but these did not reach statistical significance under the more stringent P value of .0083: (1) patients who received SHT and CILA tended to report lower mean (P = .0224) and maximum (P = .0102) pain scores than patients who received CILA alone; and (2) patients who received thoracic epidural analgesia alone tended to report lower mean (P = .0475) and maximum (P = .0361) pain scores than patients who received CILA alone.
Secondary outcome: opioid use
There was a significant association between SHT, postoperative pain management technique, and morphine equivalents per hour received (Fig. 3). Patients who received thoracic epidural analgesia used significantly more morphine equivalents per hour (1.31, 95% CI 0.32–2.30, P = .0104) than patients who received CILA. Patients who received preoperative SHT used significantly less morphine equivalents per hour over time (−0.13, 95% CI −0.25 to 0.00, P = .0465) than patients who did not receive SHT. Two trends in morphine equivalents per hour used across the 4 treatment groups were identified, but these did not reach statistical significance under the more stringent P value of .0083: (1) patients who received SHT and CILA tended to use less morphine equivalents (P = .01) than patients who received thoracic epidural analgesia alone; and (2) patients who received thoracic epidural analgesia alone tended to use more morphine equivalents (P = .0104) than patients who received CILA alone.
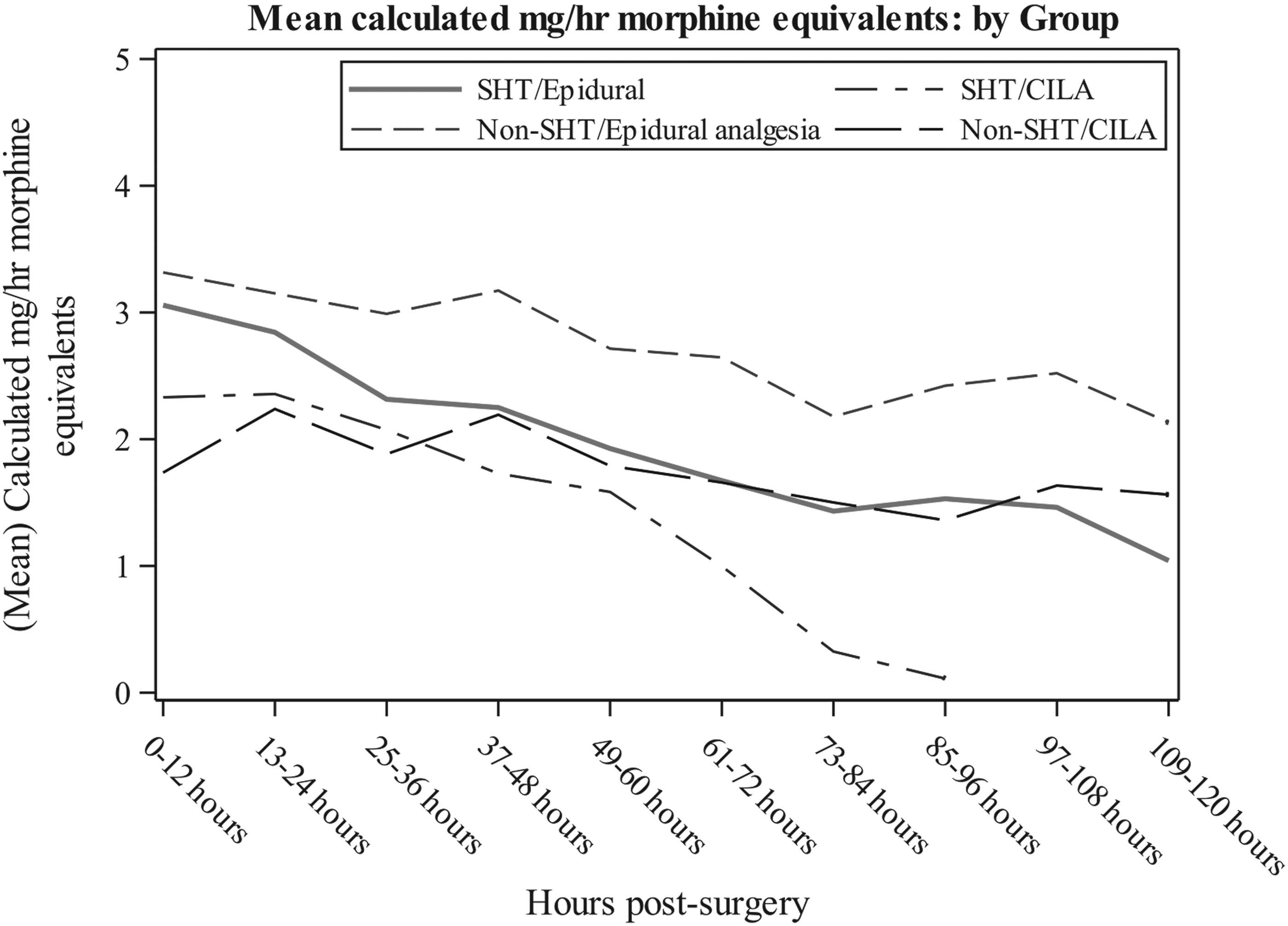
Calculated morphine equivalents (mg/hour) administered over time. Plot of mean opioid (morphine) and morphine equivalents of IVNSAID (Table 2) administered each hour reported in 12-hour postoperative intervals for all 4 treatment groups. CILA, continuous infusion of local anesthetic; IVNSAID, intravenous nonsteroidal anti-inflammatory drug; SHT, self-hypnosis training.
When adjusting pain models for received morphine equivalents per hour, the main effects for treatment associations remained significant (SHT: −2.06, 95% CI −3.22 to −0.90, P = .0008; thoracic epidural analgesia: −1.72, 95% CI −2.92 to −0.52, P = .0059). A significant association was also seen for morphine equivalents used and pain, with pain scores increasing as received morphine equivalents per hour increased (mean pain: 0.16, 95% CI 0.01–0.32, P = .0385; maximum pain: 0.34, 95% CI 0.14–0.54, P = .0010). When adjusting pain models for received morphine equivalents, comparisons of self-reported pain intensity scores across the 4 treatment groups indicated that: (1) patients who received SHT and thoracic epidural analgesia reported significantly lower mean (P < .0001) and maximum (P < .0001) pain scores compared with patients who received CILA alone; and (2) patients who received thoracic epidural analgesia reported significantly lower mean (P = .0029) and maximum (P = .0011) pain scores than patients who received CILA. One other pain intensity score trend was identified when pain models were adjusted for received morphine equivalents per hour, but this did not reach statistical significance under the more stringent P value of .0083. Patients who received SHT and CILA tended to report lower mean (P = .0285) and maximum (P = .0293) pain scores than patients who received CILA but had not received SHT.
Hospital LOS and opioid-related side effects
Postoperative LOS was significantly different among the 4 treatment groups (P = .0010) (Fig. 4). Pairwise comparisons of LOS for all possible pairs demonstrated that patients who received SHT and CILA had shorter LOS than patients who received thoracic epidural analgesia alone (P = .0013).

Postoperative hospital LOS. Whisker plot of hospital LOS (hours) for each treatment group. Diamond symbol is mean LOS. °P = .0013 compared to non-SHT/epidural anesthesia group. LOS for SHT/CILA group. CILA, continuous infusion of local anesthetic; LOS, length of stay; SHT, self-hypnosis training.
Nausea and vomiting were the most prevalent opioid-related side effects documented in patients' medical records. All but 9 patients reported nausea, and 26 patients vomited during the first 120 postoperative hours (5 days). Vomiting was not significantly associated with CILA use, χ2 (1, n = 53) = 0.037, P = .848, phi = 0.066, or SHT, χ2 (1, n = 53) = 0.161, P = .688, phi = −0.093.
All but 1 patient had a urinary catheter for the first 24 hours after surgery. By 37 hours after surgery, more than 30% of patients had their urinary catheter removed (11 CILA, 5 thoracic epidural analgesia, and 10 SHT); and by 49 hours, 60% had their urinary catheter removed (12 CILA, 20 thoracic epidural analgesia, and 19 SHT). At 37 hours, continued urinary catheter use was significantly associated with thoracic epidural analgesia use, χ2 (1, n = 53) = 10.245, P = .001, phi = −0.483, but not at 49 hours, χ2 (1, n = 53) = 0.140, P = .708, phi = −0.092. Urinary catheter removal was not associated with SHT.
Pruritus was uncommonly reported after Nuss procedure. Of the 10 patients who reported pruritus during the first 120 postoperative hours, all but 1 received thoracic epidural analgesia. Three patients had persistent pruritus for more than 36 hours after surgery.
There were no occurrences of respiratory distress, but more than 40% of patients in the cohort were on oxygen at some point during the first 120 postoperative hours of hospitalization. Oxygen use was not significantly associated with CILA use, χ2 (1, n = 53) = 3.755, P = .053, phi = −0.03, or SHT, χ2 (1, n = 53) = 0.038, P = .846, phi = −0.065. Three patients in the thoracic epidural analgesia alone group experienced sedation. One patient in the thoracic epidural analgesia with SHT group had two episodes of mental status changes.
Only 14 patients had a bowel movement in the first 120 hours after surgery, with 5 additional patients discharged home before a bowel movement was recorded in their medical record. Almost all (81%) patients were started on a bowel management medication in the first 36 hours after surgery. These varied and included: stool softeners every 12–24 hours (11 and 4 patients, respectively); oral stimulants every 12–24 hours (9 and 11 patients); both a stimulant and a stool softener (3 patients); or other agents (5 patients). Bowel management regimen or bowel movement before discharge to home were not associated with any treatment group.
Discussion
The aim of this retrospective study was to compare the efficacy of postoperative CILA and thoracic epidural analgesia with and without preoperative SHT for the treatment of pain after Nuss procedure. We found that patients who received preoperative SHT reported significantly lower pain scores and used significantly less morphine equivalents per hour over time than patients who did not receive preoperative SHT. Patients who received thoracic epidural analgesia reported significantly lower pain scores, but used significantly more morphine equivalents per hour than patients who received CILA. Higher patient pain scores were associated with increased use of morphine equivalents per hour; however, the main effects for treatment associations remained significant after adjusting for received morphine equivalents per hour. In addition, patients who received SHT and CILA had significantly shorter LOS than patients who received only thoracic epidural analgesia. These results add to the limited knowledge of the effectiveness of preoperative SHT as an adjunct to postoperative pain management after Nuss procedure.
In our previous pilot study of thoracic epidural analgesia in 22 patients with and without preoperative SHT, we were unable to demonstrate a difference in mean and maximum pain intensity scores. 33 In this larger cohort, mean pain intensity scores for patients receiving SHT were more than 1 point lower compared with patients who did not receive SHT, with a CI of 0.55–2.89; maximum pain intensity scores were more that 2 points lower, with a CI of 0.82–3.73. A one-point difference in pain intensity scores is considered clinically significant. 39
Our results are not consistent with those of Lobe, who reported that SHT decreases hospital LOS after Nuss procedure. 36 While postoperative hospital LOS was significantly different among the 4 treatment groups in our study, only the CILA with SHT group had a statistically significantly shorter LOS compared with patients who received thoracic epidural analgesia alone. In Lobe's study, patients who received SHT also received IVPCA and patients who did not receive SHT were treated with thoracic epidural analgesia. 36 Therefore, thoracic epidural analgesia may be contributing to the longer postoperative LOS seen in both studies.
The most significant benefit of CILA may be the lower risk of major thoracic epidural anesthesia-related complications. 30 We and others have investigated CILA as a less risky alternative to thoracic epidural analgesia for postoperative pain management after the Nuss procedure. In this study, CILA allowed for earlier postoperative termination of urinary catheter use, which may prevent postoperative catheter-related urinary tract infections. Postoperative nausea, vomiting, constipation, and oxygen use were common with CILA, and the association of these postoperative concerns was no different from those associated with thoracic epidural analgesia. In contrast, postoperative pruritus was only reported by 1 patient who received CILA compared to almost 25% of those who received thoracic epidural analgesia. The most concerning major complications of thoracic epidural analgesia are rare, and no incidents of respiratory depression or neurologic injury were identified in any patient in this study.
A retrospective study comparing postoperative CILA to thoracic epidural analgesia for children's postoperative pain showed no significant difference in reported pain, time to ambulation, or time to recovery of postoperative ileus. 32 Supplemental opioid use was higher on the first postoperative day for children in the CILA group, but patients in this group had a significantly shorter duration of urinary catheter placement. 32 In two other retrospective studies comparing thoracic epidural analgesia to multimodal anesthesia 27 and intercostal nerve cryoablation after Nuss procedure, 40 pediatric patients also received CILA. While subset analyses of patients who received CILA demonstrated decreased LOS and opioid use with cryoablation compared to thoracic epidural analgesia, outcomes for patients who received CILA were not compared to patients who did not receive CILA. 40
In our study, patients who received CILA reported significantly greater mean and maximum pain intensity scores than patients who received thoracic epidural analgesia for postoperative pain management after Nuss procedure. These results were surprisingly inconsistent with the significantly lower use of morphine equivalents per hour by these patients and our finding that higher pain scores were associated with increased use of morphine equivalents per hour. A potential explanation for this inconsistency is increased pain with movement with CILA compared to thoracic epidural analgesia. Patients who receive CILA are encouraged to be up and out of bed up to three times per day in the first 5 days after surgery. We noted in our pilot study differences in pain intensity scores during the evening and into the night after times of increased activity. 33 If patients have increased pain with movement, this may have skewed their mean and maximum 12-hour interval pain scores. Morphine equivalent use per hour was found to increase with increased pain; but if pain is isolated to limited episodes of movement, these patients' overall morphine equivalent use per hour per 12-hour interval could potentially be less than patients who must vigilantly treat their pain with supplemental morphine equivalents at both rest and with movement. As pain intensity in relationship to activity and movement is not well documented in patients' medical records, a prospective study of pain and opioid use that includes documentation of patient movement is needed to test this hypothesis.
An alternative explanation for the higher pain scores with less morphine use may be related to the shortened LOS among patients who received CILA. Thoracic epidural analgesia and thoracic epidural catheters were discontinued by the third postoperative day. With the loss of thoracic epidural analgesia, more opioids may have been needed to control patients' pain during their transition to other forms of analgesia. CILA is continued at home after patient discharge, so transition to other forms of analgesia is not required. Opioid availability and use may have been less frequent as CILA patients were readied for earlier hospital discharge. In addition, patients who received SHT and CILA had significantly shorter LOS than patients who received thoracic epidural analgesia alone; SHT has been shown to have an opioid-sparing effect in this and our pilot study. 33
Another important difference to note between the CILA with SHT group and the thoracic epidural analgesia alone group is their pectus excavatum severity. Haller index measurements were significantly different for these 2 groups. It is reasonable to expect that the extent of correction required would correlate with hospital LOS and morphine equivalents required to manage postoperative pain when other pain management treatments are not available. This also emphasizes the importance of our finding that the main effects for SHT and thoracic epidural analgesia remained significant even after pain models were adjusted for received morphine equivalents per hour.
This study has several limitations. First, the sample size was small with only 53 patients in the study distributed into 4 treatment groups. To increase the sample size of patients undergoing this particular surgical procedure, a multisite study would be required. Second, in 2 of the groups, there was a significant difference in the Haller index, a measure of pectus excavatum severity that may correlate with postoperative pain. In addition, patients self-selected to receive or not receive preoperative SHT, and surgeons selected whether patients received CILA or thoracic epidural analgesia. The difference in patients' and surgeons' decisions may predispose the results to bias from an unmeasured difference in the groups. Randomization to treatment is needed to confirm our study findings. Third, there was lack of standardization in prescribed analgesics within the cohort. The mathematical correction to morphine equivalents is based on equianalgesic data from single-dose analgesic studies rather than repeated administration of these analgesics over time for a dynamic postoperative pain condition. In addition, there are no published equianalgesic data for acetaminophen or ibuprofen, so the extent to which these analgesics may have contributed to patients' pain management could not be calculated. Fourth, timing and number of postoperative hypnosis coaching sessions were not standardized and were based on patient need and availability of the integrative medicine physician. The final limitation of the study is the retrospective design. While only one data point was missing, documented outcome data from medical records may not fully reflect patient experience and treatment. A prospective randomized controlled trial is needed to validate the effectiveness of SHT and CILA for pain management after this and other painful pediatric surgical procedures.
We hypothesized that adolescent patients who received preoperative SHT and postoperative CILA for pain management after Nuss procedure would experience significantly less self-reported pain, use less opioids, experience less opioid-related side effects, and have a shorter hospital LOS compared to patients who received SHT with thoracic epidural analgesia or who received no SHT. The results of this study suggest that SHT before surgery provides adolescents with an effective opioid-sparing adjunctive therapy for the management of postoperative pain after the Nuss procedure. CILA also had an opioid-sparing effect, but was associated with more self-reported pain than thoracic epidural analgesia. Patients who received SHT and CILA experienced shorter hospitalizations than patients who received thoracic epidural analgesia without SHT. When adjusting for received morphine equivalents, the main effects for SHT associations remained significant, thus supporting our hypothesis. More research is needed to determine the effectiveness of SHT for symptom management after painful pediatric surgical procedures and the comparative effectiveness of CILA as an alternative to thoracic epidural analgesia for major pediatric surgical procedures.
Footnotes
Acknowledgments
The authors thank Stacey Tobin for her editorial expertise and review of this article. The authors also thank Sandra Riccardelli, RN, James Santanelli, MPH, Ashley Pantaleo, BA, and Brendan Campbell, MD for their assistance conducting the study.
Disclosure Statement
No competing financial interests exist.