
Abstract
Abstract
Objective:
To compare the feasibility of three-dimensional visualization technology (3DVT) with that of routine computed tomography (CT) examination during planning of laparoscopic surgery for pheochromocytoma (PHEO) and paraganglioma (PGL) and the effects on operative and postoperative outcomes.
Patients and Methods:
The clinical data for 36 patients who underwent laparoscopic surgery for PHEO/PGL in our department from January 2016 to April 2017 were analyzed retrospectively. Fourteen patients underwent laparoscopic surgery for PHEO/PGL after preoperative 3DVT-based assessment and 22 after conventional CT examination. The demographic parameters, surgical procedures used, and perioperative outcomes were compared between the two groups. Data were entered into a Microsoft Excel worksheet and analyzed using SPSS version 24.0.
Results:
No significant differences were found between the groups with regard to age, gender, body mass index, tumor size, surgical approach, estimated blood loss, mean length of hospital stay, number of hypertensive and hypotensive episodes during surgery, peak blood pressure (BP) values during tumor handling, and minimum values after tumor excision. However, the operating time was significantly shorter and the fluctuations in BP were significantly lower in the 3DVT group.
Conclusions:
3DVT is a feasible and useful preoperative assessment method in patients undergoing laparoscopic surgery for PHEO/PGL. This imaging technique accurately shows the relationship between the tumor and peripheral structures and aids the surgeon's understanding of the anatomic structure in the operative area and in surgical planning.
Introduction
N
Laparoscopic adrenalectomy has been the golden standard procedure for all adrenal pathologies since it was first defined in 1992. 5 However, the surgery becomes progressively more difficult with increasing size of the adrenal tumor. 6 Laparoscopic surgery for PHEO/PGL tends to be difficult because these tumors are larger and have more complications related to their secretion of hormones. 7 Furthermore, the incidence of intraoperative bleeding is high because of the rich blood supply around the tumor and its anatomic position. 8 Therefore, it is essential to have a clear understanding of the surgical anatomy of the target tumor and its relationship with peripheral structures. If surgeons know the location of the adrenal central vein preoperatively, they can identify and ligate it rapidly, which would prevent entry of catecholamines into the bloodstream, thereby reducing fluctuations in blood pressure (BP) as well as the risk of postoperative heart failure and pulmonary edema.8,9
Modern preoperative imaging techniques, including intraoperative ultrasonography, computed tomography (CT), magnetic resonance imaging, and 18 F-DOPA positron emission tomography, have played an important role in improving the safety of surgery by providing surgical guidance and allowing evaluation of treatment.10,11 The three-dimensional (3D) visualization technology (3DVT), based on preoperative image processing of CT data, was only described in a medical context a few years ago, but has rapidly emerged as a tool that can improve the visibility and accessibility of the operative field before surgery and allows simulated manipulation as part of the surgical planning. 12
Presently, there is no literature showing 3DVT to be superior to conventional CT during laparoscopic surgery for PHEO/PGL. Herein, we report our experience with 3DVT when used for preoperative assessment of these tumors. To our knowledge, this is the first comparative study of the impact of 3DVT laparoscopic surgery on perioperative outcomes in patients with PHEO/PGL.
Patients and Methods
Patient data
Thirty-six patients with a diagnosis of PHEO/PGL were retrospectively identified to have undergone laparoscopic surgery in our department between January 2016 and April 2017. Fourteen of these patients underwent laparoscopic surgery after 3DVT planning and 22 after traditional preoperative CT. The study inclusion criteria were as follows: a tumor size >4.5 cm on preoperative CT; a unilateral tumor; a postoperative pathologic diagnosis of PHEO/PGL; and postoperative follow-up of at least 6 months. The study was approved by the Institutional Ethics Review Board at the Xiangya Hospital of Central South University. The patient demographic characteristics are shown in Table 1.
Data are shown as the number or as the mean ± standard deviation.
Fisher's exact test (two-sided); bStudent's t-test (two-sided).
3DVT, three-dimensional visualization technology; CT, computed tomography; PGL, paraganglioma; PHEO, pheochromocytoma.
CT scanning and 3D reconstruction
A 64-multidetector row CT scanner with a 0.5-mm step interval was used in all 36 patients to acquire enhanced CT scans, including arterial, parenchymal, and secretory phases. Routine axial and coronal images were obtained during CT reconstruction. All CT image data were transferred to Digital Imaging and Communications in Medicine format and then segmented and reconstructed to create 3D digital images using the Medical Imaging Three Divisional Visualization System (Yorktal, Inc., Shenzhen, Guangdong, China).
Surgeons can observe the relationship between the tumor and peripheral structures using the FreeForm Modeling System (SensAble Technologies, Inc., Woburn, MA) after importing the reconstructed model data. The tumor, kidney, adrenal gland, local arteries, and veins are distinguished using different colors for each structure. This system can help surgeons to rotate, amplify, delete, and hyalinize for better visualization of the anatomy of the surgical area (Fig. 1).
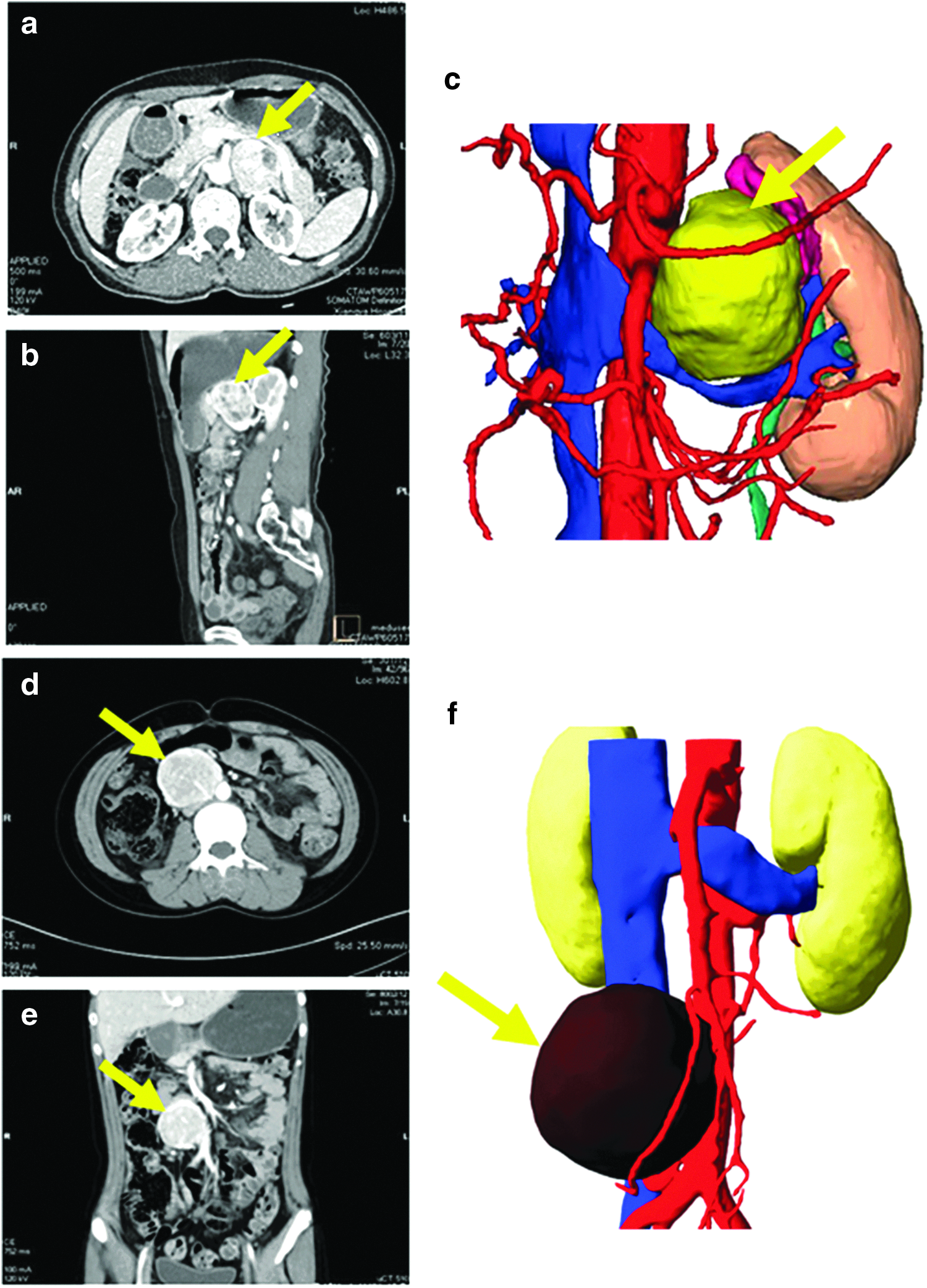
Computed tomographic images and the three-dimensional visualization model.
Preoperative management and surgical procedures
In all cases, an α-adrenoceptor antagonist (phenoxybenzamine or prazosin) was administered preoperatively. A β-blocker was administered to control reflex tachycardia when needed. All patients were placed in the lateral or supine position while under general anesthesia. Continuous direct measurements of systolic BP (SBP), diastolic BP (DBP), and central venous pressure were taken intraoperatively. The heart rate was derived from the electrocardiogram.
After learning about the relationship of the tumor and the peripheral structures from the preoperative imaging, the tumor was carefully dissected from the surrounding tissues and resected through a transabdominal or retroperitoneal approach. Increases in BP or heart rate during surgery, particularly during handling of the tumor, were treated by incremental central intravenous doses of phentolamine or labetalol, respectively, together with an increase in the isoflurane concentration if necessary. The appropriate agent was injected as soon as the SBP exceeded 160 mmHg or the heart rate reached more than 90 beats/min. Peak SBP, DBP, and heart rate values were recorded during the delay time before these hemodynamic variables responded to the relevant drug(s).
Data collection and statistical analysis
Demographic characteristics (age, sex, and body mass index) and clinical data (BP, heart rate, tumor size, operating time, estimated blood loss, and length of hospital stay) were recorded. All data were entered into a Microsoft Excel worksheet and statistical analyses were performed using SPSS version 24.0 software (IBM Corp., Armonk, NY). Qualitative variables were analyzed using Fisher's exact test and quantitative variables were compared using the Student's t-test after being tested for normality with Levene's test. A two-sided P value <.05 was considered to be statistically significant.
Results
As shown in Table 1, 14 patients underwent surgery after preoperative 3DVT planning and 22 after routine preoperative CT. The two groups were comparable with regard to gender (P = .732), age (P = .603), body mass index (P = .159), and number of PHEO/PGL (P = .634).
Table 2 shows the intraoperative and postoperative outcomes for operations performed with and without preoperative 3DVT planning. The operating time was significantly shorter in the 3DVT group than in the CT group (119.9 ± 33.2 minutes versus 144.1 ± 32.8 minutes, P = .039). There was no significant difference in the location of the tumor (left/right; 6/8 versus 7/15, P = .723), tumor size (5.7 ± 0.7 cm versus 5.8 ± 0.6 cm, P = .845), surgical approach (transabdominal/retroperitoneal; 3/11 versus 7/15, P = .706), estimated blood loss (119.9 ± 33.2 mL versus 144.1 ± 32.8 mL, P = .351), or mean length of hospital stay (6.6 ± 1.2 days versus 6.8 ± 1.3 days, P = .580) between the two groups.
Data are shown as the number or as the mean ± standard deviation.
Fisher's exact test (two-sided); bStudent's t-test (two-sided).
3DVT, three-dimensional visualization technology; CT, computed tomography.
Laparoscopic surgery for PHEO/PGL was successfully performed in all cases with no unexpected interruptions or conversions to open surgery. The final pathological result confirmed PHEO/PGL in all cases. The surgeons considered that 3DVT accurately showed the relationship between the tumor and the peripheral structures and helped them to avoid adjacent blood vessels and identify the adrenal central vein more rapidly (Fig. 2), which significantly shortened the operating time and reduced intraoperative fluctuations in BP.
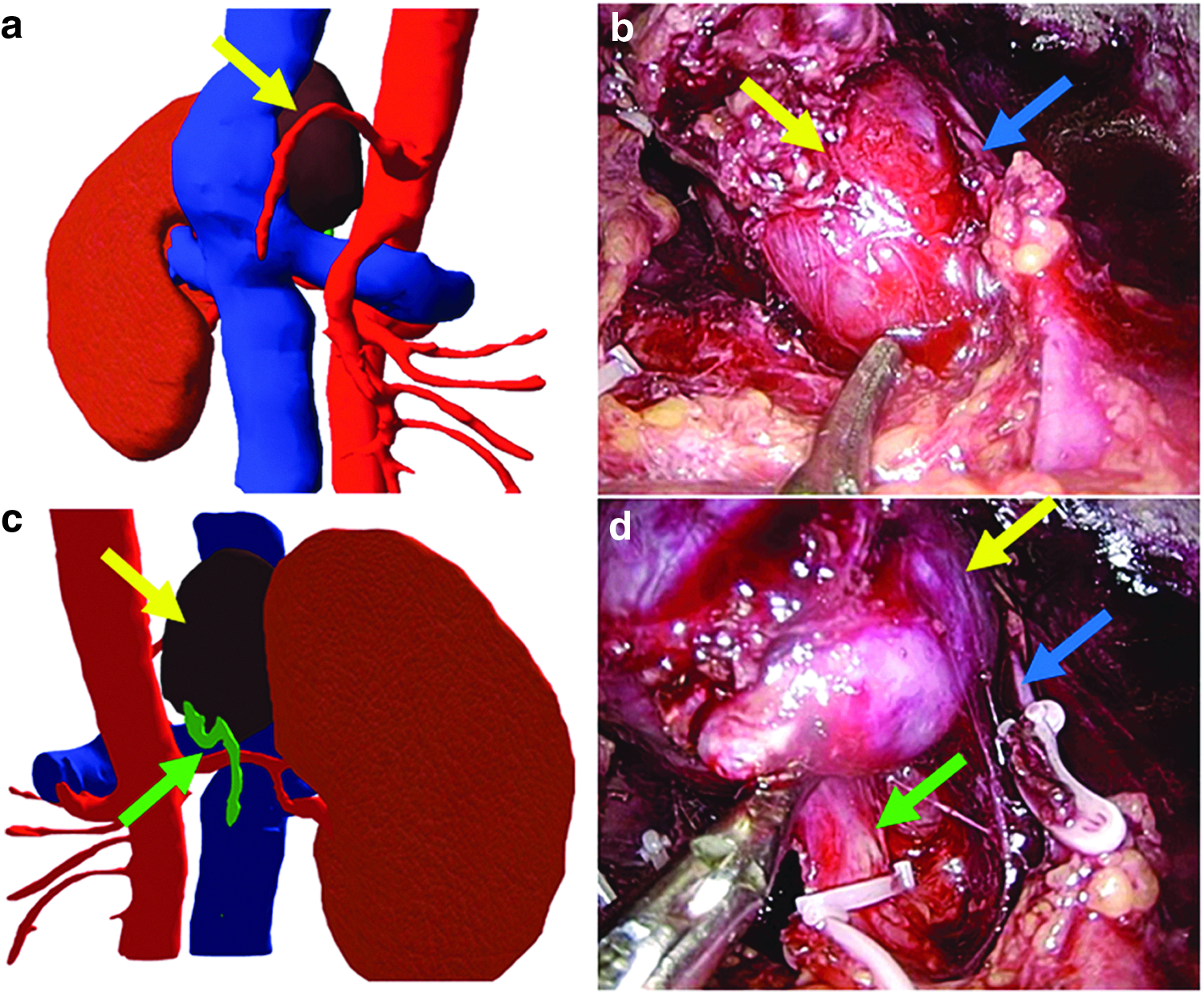
Intraoperative images and the three-dimensional visualization model.
The intraoperative BP and heart rate measurements are shown in Table 3. No significant difference was found between the two groups in terms of the number of hypertensive episodes with SBP >200 mmHg or DBP >100 mmHg (8/14 versus 14/22, P = .738) or hypotensive episodes with SBP <80 mmHg (2/14 versus 5/22, P = .681). Furthermore, there were no significant between-group differences in peak SBP, DBP, or heart rate values during tumor handling or in the minimum values after tumor excision (P > .05). However, the difference (Δ) between the peak values during tumor handling and minimum values after tumor excision suggested that 3DVT had a clear advantage over CT in terms of less fluctuation in BP (ΔSBP, 75.1 ± 22.2 mmHg versus 91.5 ± 21.8 mmHg, P = .037; ΔDBP, 36.5 ± 16.0 mmHg versus 47.4 mmHg ±13.6 mmHg, P = .036).
Data are shown as the number or as the mean ± standard deviation.
Fisher's exact test (two-sided); bStudent's t-test (two-sided).
Δ indicates (peak values during tumor handling) minus (minimum values after tumor excision).
3DVT, three-dimensional visualization technology; BP, blood pressure; CT, computed tomography; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure.
Discussion
It is well known that laparoscopic surgery for PHEO/PGL poses a challenge to both the surgeon and the anesthetist because the average size of these tumors is larger than that of other tumors. Furthermore, there is a high risk of release of catecholamines and hypertensive crisis during pneumoperitoneum and tumor handling. Severe arterial hypotension is common after excision of these tumors because of relative vasodilation and the residual effect of antihypertensive drugs.6,13 In the past, the upper limit of size for endoscopic resection of PHEO/PGL was 6 cm, but with refinement of medical imaging techniques and improved skills in laparoscopic adrenalectomy, several surgeons report excisions larger than 8 cm.14–16
Improved medical imaging techniques are now providing more comprehensive information about anatomic structures in the surgical field, which can reduce intraoperative difficulties and improve the safety of surgery. Clearly, knowledge of the relationship between a tumor and its peripheral structures has an important role in successful completion of a surgical procedure. CT, particularly CT urography, is the most commonly used imaging technique in PHEO/PGL, and 3D reconstruction, which involves volume rendering, maximum intensity projection, curved planar reformation, and other postprocessing techniques, can clearly show the location of the tumor.17–19 However, image reconstruction using traditional CT is often unsatisfactory because of the weak representation of the relationship between the tumor and the peripheral blood vessels. Thus, the pursuit of more powerful medical image postprocessing technology continues.
Recently, Souzaki et al. 9 used a 3D-printed model based on preoperative CT images to simulate the laparoscopic view and range of movement of forceps in 3 pediatric patients with adrenal neuroblastoma. All the tumors were completely resected without any surgical complications. The authors reported that these 3D-printed models were very helpful for understanding the patient's surgical anatomy and for planning the surgical procedure. However, the cost of these printed models may be prohibitive and limit their applicability, especially in developing countries.
Mitterberger et al. 20 used three-dimensional computed tomography to assess 14 adrenal masses in 12 patients before laparoscopic adrenal-sparing surgery. Most of the patients had primary hyperaldosteronism and the mean tumor size was 2 cm. The colored surface-rendered images provided more accurate intraoperative information and were more convenient to use than the volume-rendered CT images. Detection of the adrenal gland, the vessel system, and the tumor was perfectly clear, and complex anatomic relationships were easily grasped. The 3D-CT with state-of-the-art techniques is an accessible method for evaluation of adrenal tumors, serves as an excellent guide for laparoscopic adrenal-sparing surgery, and helps surgeons to avoid potential complications.
In our series, the average tumor size was larger (>5.0 cm), and most of the tumors had a complex anatomic relationship with the peripheral structures. The 3DVT accurately showed the relationship between the tumor and the peripheral blood vessels, and helped the surgeons to understand the anatomic structure in the operative area and avoid operative risks, which significantly shortened the operating time. In some patients, the surgeons knew the location of the adrenal central vein from preoperative 3DVT. In these cases, they could rapidly find and ligate this vein to prevent more catecholamines entering the bloodstream, which lessened the fluctuations in BP. Our results indicate that 3DVT facilitated accurate image-guided tumor resection.
We now have some clinical experience in the application of 3DVT. First, we only use 3DVT in patients with larger or complex tumors. Second, in some patients, we cannot find the adrenal central vein on 3DVT. However, we hope to be able to increase the usefulness of this technology in the future. Furthermore, we have found that 3DVT does not reduce intraoperative bleeding, which may be related to the abundant microvasculature around the tumor.
This study has several limitations. First, it was retrospective in nature, so may contain a degree of selection bias. Second, the clinical data were collected from a small patient group at a single center, and future studies will need to include larger groups of patients. The third and possibly a very important limitation is that the follow-up was short, so more research with longer-term follow-up is needed to assess the oncologic outcomes of 3DVT planning in patients with these tumors.
Conclusion
We have confirmed that 3DVT accurately shows the relationship between PHEO/PGL tumors and the peripheral structures, helping surgeons to avoid operative risks and decreasing the operating time. The 3DVT provides an excellent guide for laparoscopic surgery in patients with PHEO/PGL.
Footnotes
Acknowledgment
This work was supported by the Fundamental Research Funds for the Central Universities of Central South University no. 502211718.
Disclosure Statement
No competing financial interests exist.