
Abstract
Abstract
Purpose:
Intraperitoneal local anesthetic nebulization is a new and novel technique for providing pain relief following laparoscopic cholecystectomy. We compared the analgesic efficacy of intraperitoneal ropivacaine-fentanyl nebulization with ropivacaine nebulization alone for providing pain relief following laparoscopic cholecystectomy
Materials and Methods:
This prospective, randomized, double-blind, placebo-controlled trial included 75 American Society of Anesthesiologists I/II patients, 18–60 years old, scheduled to undergo laparoscopic cholecystectomy under general anesthesia. Patients were randomly allocated to one of the three groups of 25 patients each to receive intraperitoneal nebulization using normal saline (group I), 30 mg of 0.75% ropivacaine (group II), or 30 mg of 0.75% ropivacaine with 100 μg fentanyl (group III). Visual analogue scale (VAS) scores for pain during rest and movement, shoulder pain, nausea or vomiting, and sedation were recorded for 48 hours postoperatively. Time to providing first rescue analgesia and 48-hour tramadol consumption were also noted.
Results:
Significantly greater number of patients in the placebo group had overall VAS >30 both at rest and during movement. Greater number of these patients also complained of postoperative shoulder pain and had significantly more tramadol consumption in the postoperative period. Furthermore, patients in the ropivacaine-fentanyl group demanded first dose of rescue analgesic significantly later than the other two groups.
Conclusions:
Nebulization results in better and uniform dispersion of analgesic drug intraperitoneally. Following laparoscopic cholecystectomy surgeries, ropivacaine nebulization of intraperitoneal cavity, with or without fentanyl, provides highly effective postoperative analgesia, with decreased incidence of shoulder pain. Furthermore, addition of fentanyl to ropivacaine prolongs the duration of analgesia.
Introduction
L
In the past, numerous techniques have been tried for relief of post-laparoscopic cholecystectomy pain, with variable success rates. These include intravenous (IV) opioid and nonopioid analgesics, transverse abdominis plane blocks, port-site local anesthetic (LA) infiltration, intraperitoneal LA instillation, intraperitoneal saline administration, and low-pressure pneumoperitoneum. 2
Among the various LA techniques for pain relief that are currently in practice, intraperitoneal LA instillation is the most commonly used. 3 This route is said to block the visceral afferent signaling, thus potentially modifying visceral nociception and providing analgesia. 4 Although commonly used, previous studies have reported variable efficacy of this technique. 5 To further enhance the analgesic effect, combinations of intraperitoneal LA with many opioids, like morphine, tramadol, and fentanyl, have been studied in the past.2,3,6,7 Opioids, especially fentanyl, instilled into the peritoneal cavity along with LAs have been said to provide better and increased duration of pain relief following laparoscopic cholecystectomy.
Intraperitoneal LA nebulization is a new and novel analgesic technique. Compared to LA instillation, nebulization is said to provide better and more uniform dispersion of LA particles throughout the peritoneal surface. 1 Reviewing previous literature, we found only a few studies1,8,9 that had evaluated the analgesic efficacy of intraperitoneal LA nebulization, with none, till date, having been conducted in our population group. Furthermore, although, analgesic efficacy of intraperitoneal nebulization with LAs has been studied in the past, the effect of addition of an opioid to LA for the purpose of intraperitoneal nebulization has never been assessed. We thus decided to conduct this study with the aim of evaluating the analgesic efficacy of intraperitoneal nebulization with ropivacaine-fentanyl combination compared to ropivacaine alone for providing pain relief following laparoscopic cholecystectomy. We hypothesized that, similar to previous studies that have shown superior analgesic effect of intraperitoneal instillation of LA-opioid combination compared to LA alone, the addition of fentanyl to ropivacaine for the purpose of intraperitoneal nebulization would provide superior and longer duration of pain relief compared to intraperitoneal ropivacaine nebulization alone.
Primary outcome of our study was the incidence of significant pain (dynamic visual analogue scale [VAS] score ≥30 mm) requiring rescue analgesic, during the first 48 hours after an elective laparoscopic cholecystectomy. Secondary outcome measures included postoperative pain intensity at rest and on movement as measured by VAS scores, presence of postoperative shoulder pain, total opioid consumption in the postoperative period, time to first request for rescue analgesic, and side effects, if any, with the use of study drugs.
Materials and Methods
This prospective, randomized, double-blind study was approved by the institutional ethics committee (IEC-NK/1326/Res/629) and registered with the Clinical Trial Registry of India (registration number: CTRI/2014/08/004810; http://ctri.nic.in). After obtaining written informed consent, 75 American Society of Anesthesiologists I/II patients of both sexes, in the age group of 18–60 years, scheduled to undergo laparoscopic cholecystectomy under general anesthesia were enrolled in the study. We excluded patients with coexisting disease affecting clinical assessment, acute preoperative pain other than biliary colic, history of substance abuse, psychiatric illness, opiate tolerance, hepatic/renal dysfunction, coagulopathies, patients on chronic pain treatment, pregnant/lactating females, and patients with allergy to any of the drugs used in the study.
On the day of surgery, an anesthetist not involved in patient care confirmed patient eligibility and gave a sealed white envelope containing patient allocation and instructions for solution preparation to a nurse not involved in the study. Patients were explained about the VAS score 9 for pain where 0 mm stands for “no pain” and 100 mm stands for “worst imaginable pain”. Postoperatively, nausea was assessed by the categorical scoring system for nausea 10 (0: none, 1: mild, 2: moderate, and 3: severe). Any patient who failed to understand these scoring systems were excluded from the study design.
Randomization of patients was done by using coded sealed envelopes, which were computer generated, and subsequently, patients were allocated to one of the three groups of 25 patients each to receive intraperitoneal nebulization using 6 mL normal saline (group I), 4 mL of 0.75% ropivacaine (30 mg) with 2 mL of normal saline (group II), or 4 mL of 0.75% ropivacaine (30 mg) with 100 μg fentanyl (2 mL) (group III). An anesthetist not involved in the study prepared solutions for nebulization in 10 mL syringes filled with 6 mL of normal saline, 4 mL of 0.75% ropivacaine with 2 mL normal saline, or 4 mL of 0.75% ropivacaine with 100 μg (2 mL) of fentanyl. To maintain blinding, the anesthetists involved in the study were unaware of the study solutions being prepared.
All patients were kept fasting after midnight and premedicated with tablet alprazolam 0.25 mg and tablet ranitidine 150 mg orally a night before and 2 hours before surgery. In the operating room, patients were monitored for heart rate, blood pressure, continuous electrocardiogram, arterial oxygen saturation (SpO2), end-tidal CO2, and temperature using multichannel monitors (Datex-Ohmeda S/5 Avance). Baseline readings were recorded and an IV access was established in all patients. General anesthesia in all the groups followed a standard anesthetic technique. After preoxygenation with 100% oxygen for 3 minutes, anesthesia was induced with IV morphine 0.1 mg/kg and propofol 2–3 mg/kg. Vecuronium bromide 0.1 mg/kg was used to facilitate tracheal intubation and anesthesia was maintained with 66% nitrous oxide in oxygen supplemented with isoflurane (1%–2%). Ventilation was controlled to maintain end-tidal CO2 between 4.5 and 5.5 kPa. At the end of surgery, residual neuromuscular blockade was reversed with IV neostigmine 50 μg/kg and glycopyrrolate 10 μg/kg. All patients received dexamethasone 4 mg IV after the induction of anesthesia and ondansetron 4 mg IV at the end of surgery as a prophylactic measure for postoperative nausea and vomiting. Patients in all the groups received IV paracetamol 15 mg/kg at the end of surgery and then at 6-hourly intervals for the initial 48 hours. In addition, following surgery completion, each port site was infiltrated with 3 mL of 0.25% ropivacaine. Laparoscopic cholecystectomy was performed according to the standard surgical and anesthesia protocols. A classical four-port surgical technique that consisted of placement of a 12 mm port through the umbilical incision, a 10 mm port in the epigastric area, and two 5 mm ports on the right side of the abdomen were used for all the patients. Pneumoperitoneum was achieved using nonhumidified and nonheated CO2 with the intra-abdominal pressure maintained around 12 mm Hg.
At the end of the surgical procedure and before deflation of pneumoperitoneum, patients received intraperitoneal nebulization with normal saline, 4 mL of 0.75% ropivacaine, or 4 mL of 0.75% ropivacaine with 100 μg fentanyl using a nebulizer device, through the umbilical port. Nebulization was terminated once the nebulizer chamber was empty (∼8–10 minutes).
Nebulization device
For the purpose of giving intraperitoneal nebulization, we used an indigenously prepared, highly cost-effective nebulizing kit made with the help of an ordinary nebulizer and silicon tubing (Fig. 1), which was attached to one of the port sites. The other end of the nebulizer kit was attached to the irrigation-suction machine, which is routinely used during laparoscopic cholecystectomy procedures. This machine was used as a driving force for nebulization.

Nebulizing kit.
Postoperatively, all patients were monitored for mean arterial pressure, pulse rate, respiratory rate, temperature, VAS for pain during rest as well as during movement (dynamic VAS), shoulder pain, nausea or vomiting, and sedation (using sedation scale 10 : 0, awake & alert; 1, quietly awake; 2, asleep, but easily aroused; and 3, deep sleep) on admission to postanesthesia care unit and then at 2-, 4-, 8-, 12-, 24-, and 48-hour interval by an investigator blinded to group allocation. Patients with dynamic VAS of more than 30 mm or those demanding analgesic were provided with IV tramadol 2 mg/kg as an initial dose. Subsequent doses of tramadol, if required, were 1 mg/kg. Proportion of patients with significant pain (dynamic VAS ≥30 mm), time to providing first rescue analgesia, and 48-hour tramadol consumption were also recorded.
Statistical analysis
The primary endpoint of our study was the incidence of significant pain (dynamic VAS ≥30 mm) requiring rescue analgesic, during the first 48 hours after surgery. In a previous study involving intraperitoneal LA nebulization, 9 the incidence of patients complaining of significant dynamic pain (VAS ≥30 mm) requiring rescue analgesic, within the first 48 hours after laparoscopic cholecystectomy, is reported to be 80%. In subjects receiving nebulization, we considered an absolute reduction of 50% (i.e., from 80% to 40%) in the incidence of significant pain during the first 48 postoperative hours as clinically significant. To detect a difference of 50% in the number of patients with significant pain (VAS ≥30 mm) requiring rescue analgesic in the initial 48 postoperative hours, with an α of 0.05 and β of 0.2, we required 23 patients in each group. Considering the possibility of dropouts, we decided to enroll 25 patients in each group (total of 75 patients). The statistical analysis was carried out using Statistical Package for Social Sciences (version 15.0 for Windows; SPSS, Inc., Chicago, IL). Mean, median, and standard deviation were calculated for all quantitative variables. Normality of data was checked by measures of Kolmogorov–Smirnov tests of normality. For normally distributed data, means were compared using one-way analysis of variance. For skewed data or for scores, Mann-Whitney test was applied and interquartile range calculated. Qualitative or categorical variables were described as frequencies and proportions, with proportions being compared using chi-square or Fisher's exact test, whichever was applicable. All statistical tests were two sided and were performed at a significance level of α = 0.05
Results
A total of 85 patients were assessed for eligibility, of which 80 patients were enrolled in the study. Of the 80 patients who were enrolled in the study, 75 were included in data analysis. One patient in the placebo group and 2 each in the ropivacaine and ropivacaine-fentanyl groups were excluded due to conversion of the surgical procedure to open cholecystectomy (Fig. 2). All patients who were included in the analysis underwent multiport laparoscopic cholecystectomy. Patients in all groups were comparable with regard to age, weight, height, and surgical duration (Table 1). In the initial hours following surgery, greater number of patients in the placebo group, as opposed to the other two groups, had VAS >30 (both at rest and on movement) (Figs. 3 and 4). Furthermore, compared to the other two groups, a significantly greater number of patients in the placebo group had overall VAS >30 both at rest and during movement (Fig. 5). Ropivacaine and ropivacaine-fentanyl groups were comparable with regard to the number of patients having VAS >30. Total tramadol consumption during the study period was significantly greater in the placebo group compared to the study groups (Fig. 6). Although the study groups were comparable with regard to 48-hour total tramadol consumption, however, patients in the ropivacaine-fentanyl group demanded first dose of rescue analgesic significantly later than the other two groups (Fig. 6). Significantly more number of patients in the placebo group complained of postoperative shoulder pain (Table 2). Among all the groups, there was no significant difference in the number of patients complaining of nausea/vomiting or being excessively sedated (Fig. 7).

Flowchart of participants.
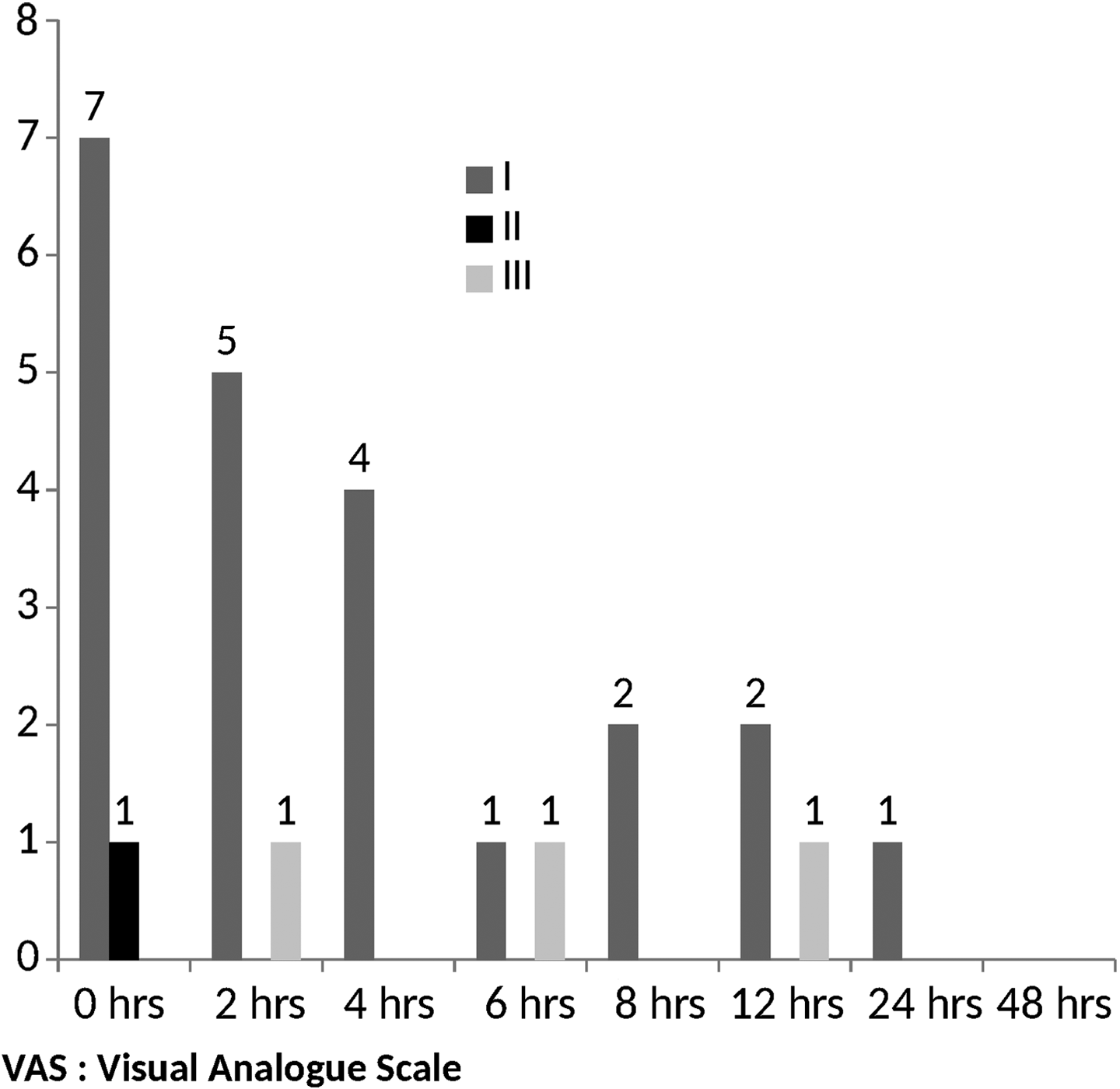
Patients with VAS score (at rest) >30 at different time points. VAS, visual analogue scale.
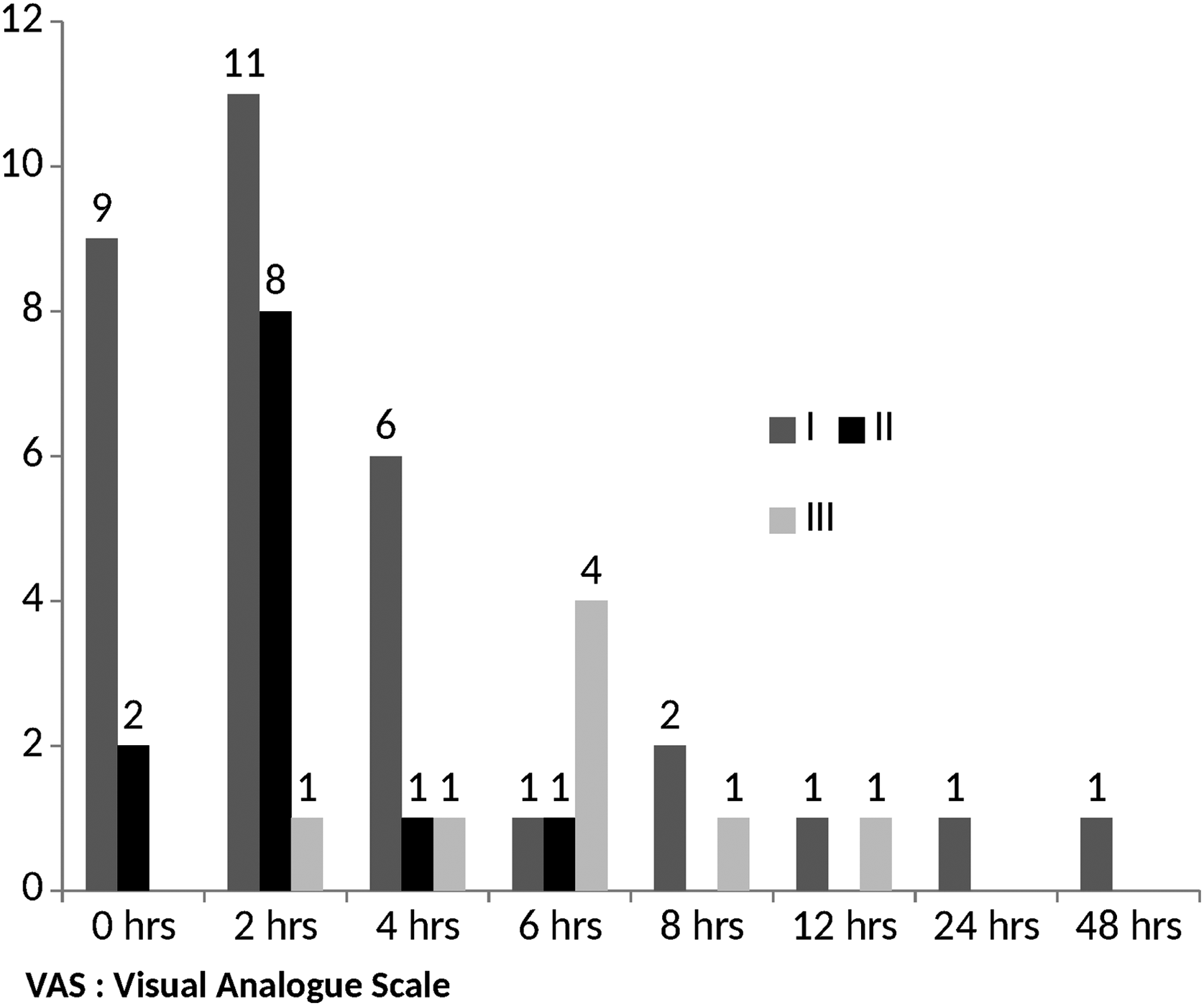
Patients with VAS score (at movement) >30 at different time points.
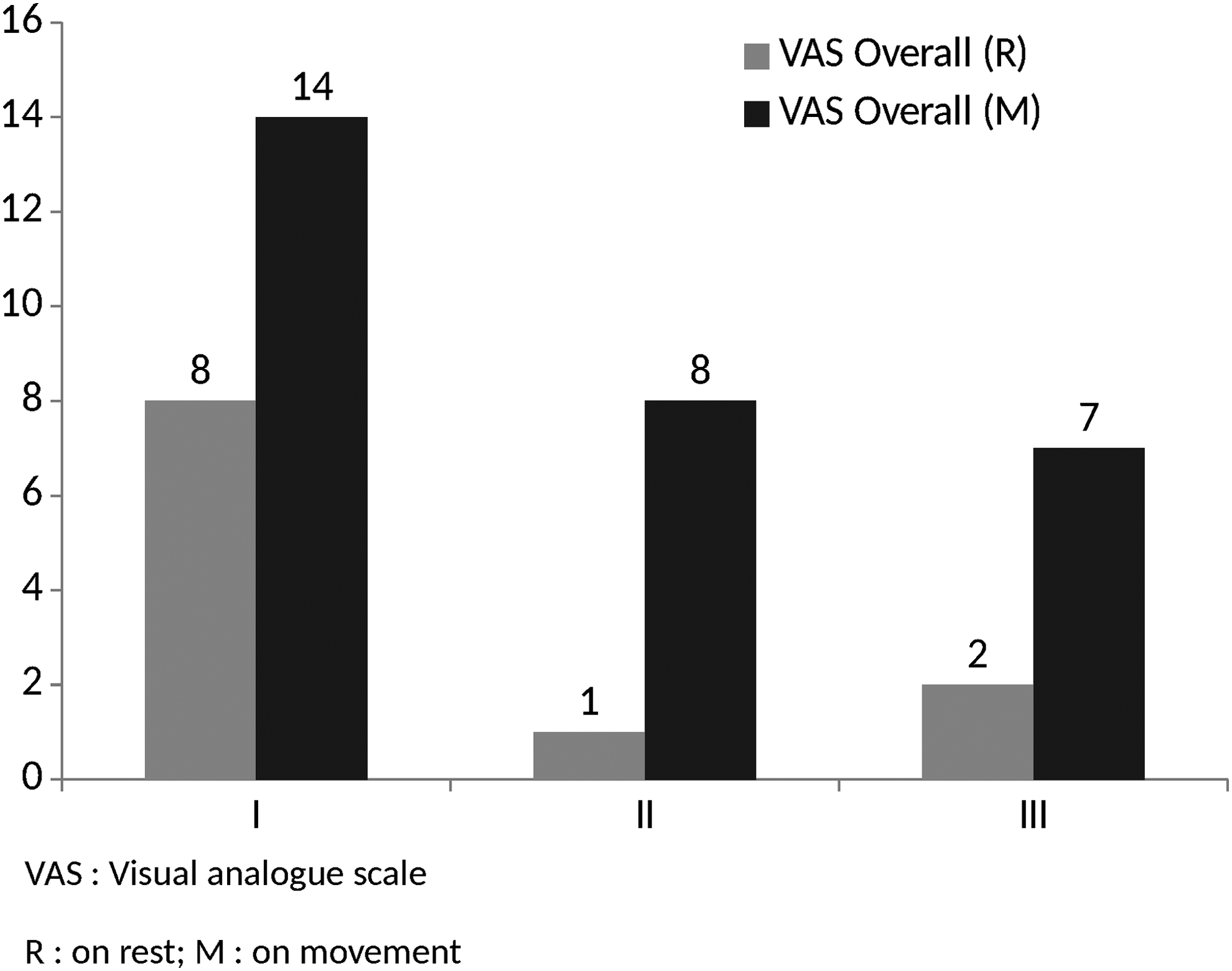
Patients with overall VAS >30 (at rest and on movement).
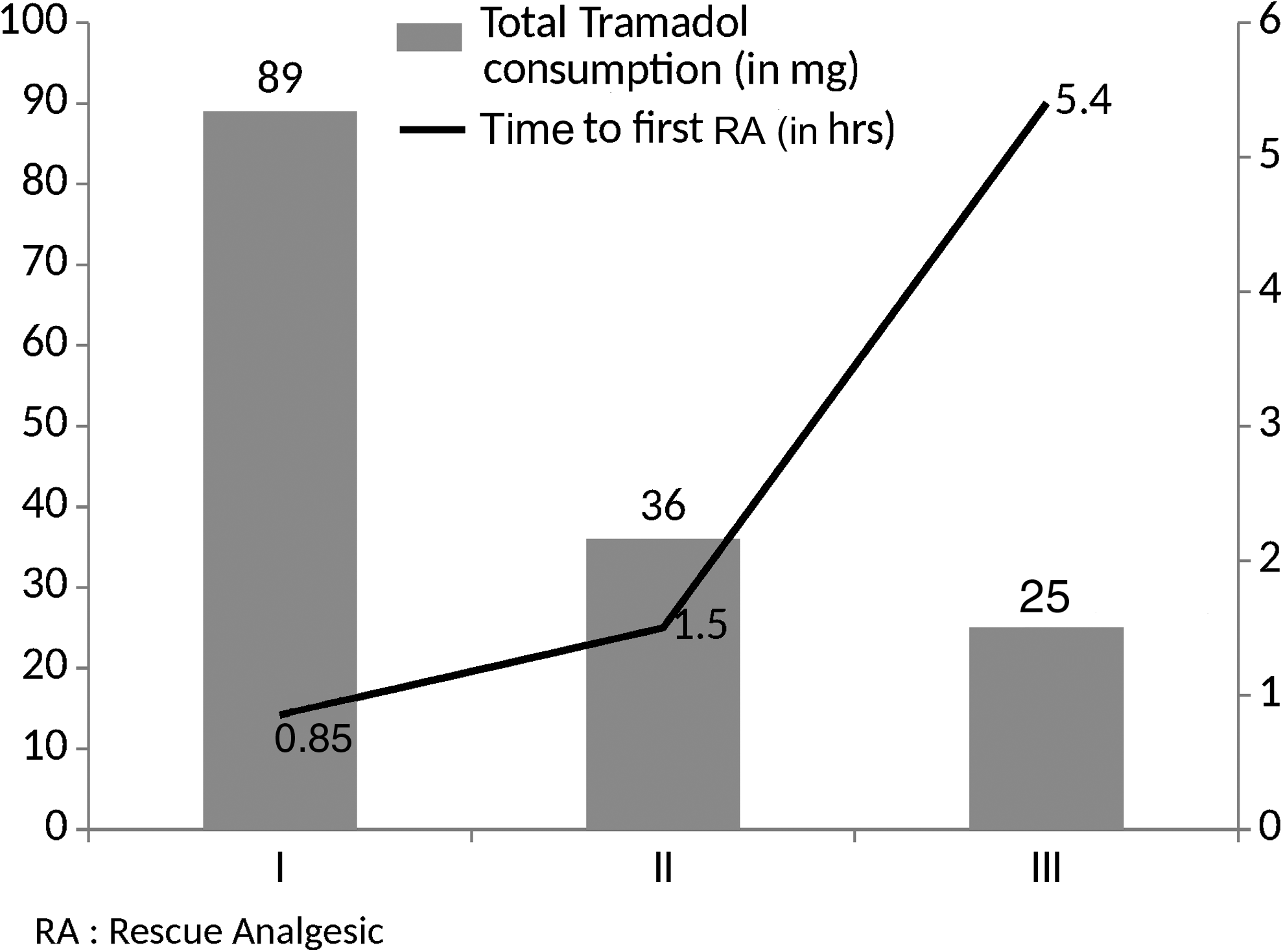
Total postoperative tramadol consumption and time to first rescue analgesic. RA, rescue analgesic.
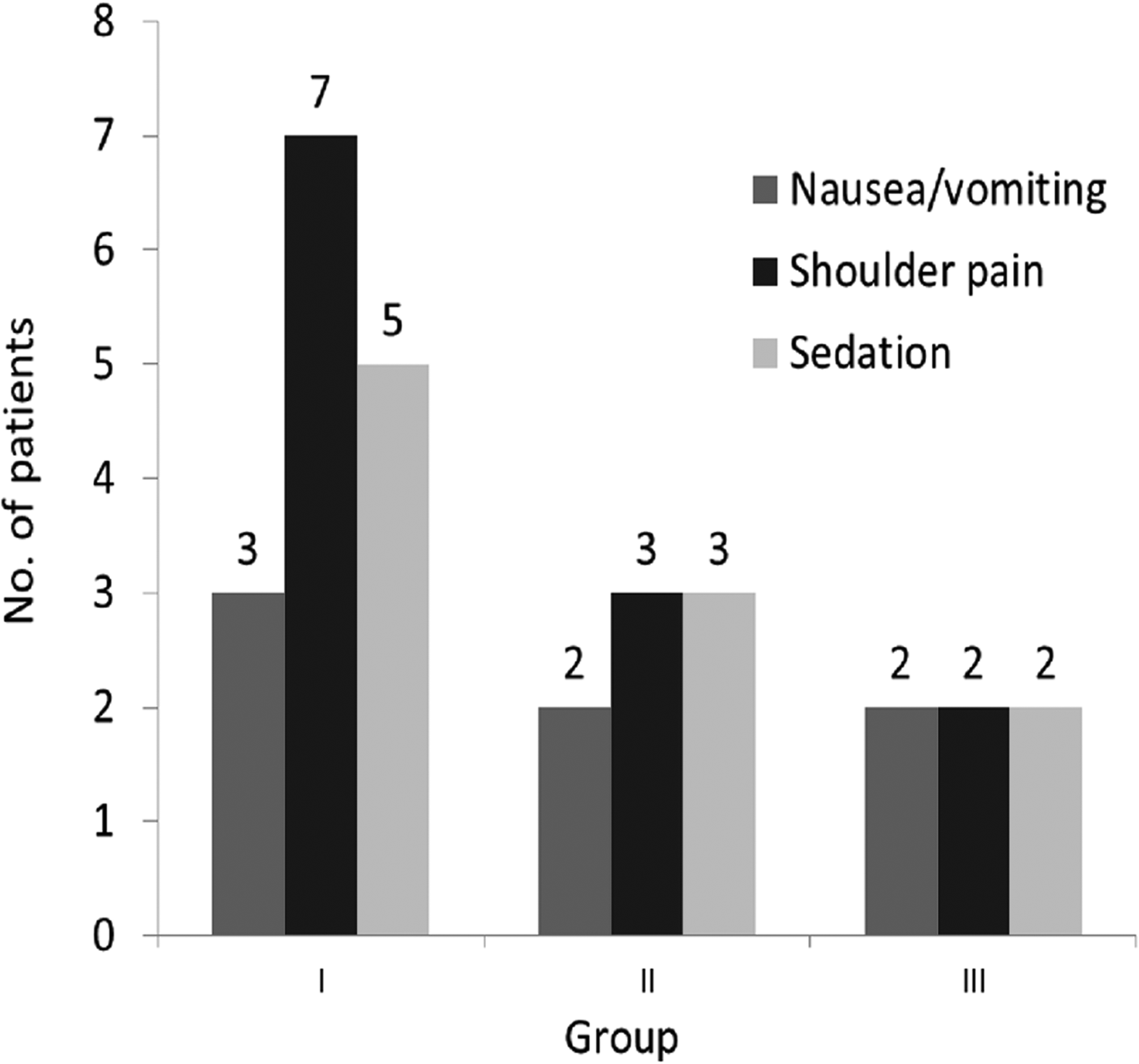
Side effects in the postoperative period.
Values are expressed as mean ± standard deviation.
BMI, body mass index.
Discussion
We compared intraperitoneal nebulization using ropivacaine with that using a combination of ropivacaine and fentanyl. We found that, compared to placebo, intraperitoneal nebulization using either of the drugs (ropivacaine or ropivacaine-fentanyl combination) significantly decreased the VAS scores and total postoperative tramadol consumption. Furthermore, greater number of patients receiving nebulization had dynamic VAS ≤30 in the initial 48 hours after surgery and these patients requested first dose of rescue analgesic significantly later than those in the placebo group. Although there was no significant difference in postoperative VAS scores and tramadol consumption between patients receiving intraperitoneal ropivacaine nebulization as opposed to those receiving intraperitoneal ropivacaine-fentanyl nebulization, however, the addition of fentanyl significantly prolonged the duration of LA action, thus delaying the requirement of first rescue analgesic. We also found lower incidence of shoulder pain in patients receiving LA nebulization with/without fentanyl.
Laparoscopic cholecystectomy, although minimally invasive, can result in significant diffuse abdominal as well as shoulder pain in the postoperative period, which can be very distressing for the patient. 1 Intraperitoneal LA instillation with or without opioids is one of the commonly used techniques to combat this pain, but with variable results.2,3,5,7 This could be due to differences in site of instillation and timing of administration, as well as different doses of LA administered. Furthermore, the conflicting results seen with intraperitoneal LA instillation could be due to inadequate and nonuniform distribution of LA throughout the peritoneal surface.
As is well known, pain following laparoscopic cholecystectomy is multifactorial. Particularly bothersome is the diffuse abdominal as well as the shoulder pain. 1 Although the exact origin of post-cholecystectomy pain still remains largely unclear, however, it is thought that the diffuse abdominal and shoulder pain could be due to peritoneal stretching and diaphragmatic irritation following CO2 pneumoperitoneum. 1 Intraperitoneal LA nebulization results in uniform dispersion and homogenous spread of LA throughout the peritoneal cavity as well as the area under the diaphragm. This could be the reason for less incidence of shoulder pain seen in our study groups. Previous study by Bucciero et al. 1 also reported a lower incidence of shoulder pain following ropivacaine nebulization compared to its instillation, thus indicating that nebulized drug spreads in a better way throughout the peritoneum. Bucciero et al. 1 used commercially available high-frequency vibrating membrane nebulizer. Due to cost restraints, we, however, used an indigenously prepared, highly cost-effective nebulization system that included an ordinary nebulizer and silicon tubing, attached to the irrigation port of the irrigation-suction machine. This machine was used as a driving force for nebulization. The ordinary nebulizer is known to generate a particle size of < 0.5 μ, thus resulting in a uniform spread of the drug throughout the peritoneal cavity. Furthermore, being highly cost-effective, its use can prove to be extremely beneficial in low resource settings.
Opioids have been used previously for intraperitoneal instillation along with LAs.3,6,7,11 Intraperitoneal instillation of bupivacaine with fentanyl is known to produce superior postoperative analgesia following laparoscopic cholecystectomy.7,11 However, use of fentanyl for intaperitoneal nebulization has never been previously reported. We found that that addition of fentanyl to intraperitoneal ropivacaine nebulization resulted in a significant prolongation of analgesia time with delay in the requirement of first rescue analgesic. We used ropivacaine and fentanyl in doses of 30 mg and 100 μg, respectively, based on previous reports by Bucciero et al. 1 (used 30 mg ropivacaine for intraperitoneal nebulization) and Gupta et al. 11 (used 100 μg fentanyl for intraperitoneal instillation). No side effects with the use of ropivacaine nebulization, with or without fentanyl, were reported in our study.
Our study had a few limitations. First, as nebulization technique creates a foggy environment, thus obscuring surgeon's view, it was not possible to nebulize intraperitoneal cavity throughout the surgical procedure. Second, we did not measure the plasma levels of study drugs, and so are unsure about the pharmacokinetics of nebulized drug.
To conclude, nebulization results in better and uniform dispersion of analgesic drug intraperitoneally. Following laparoscopic cholecystectomy surgeries, ropivacaine nebulization of intraperitoneal cavity, with or without fentanyl, provides highly effective postoperative analgesia, with decreased incidence of shoulder pain. Furthermore, the addition of fentanyl to ropivacaine prolongs the duration of analgesia. For the purpose of nebulization, we used a highly cost-effective, indigenously prepared nebulization kit, which can prove to be greatly beneficial in low resource settings.
Footnotes
Acknowledgments
The authors would like to acknowledge the immense contribution made by Mr. George Masih, senior nursing officer, general surgery operation theatre, PGIMER, Chandigarh (India), in conceptualizing and designing the nebulizer set.
Disclosure Statement
No competing financial interests exist.