
Abstract
Abstract
Background:
The curability of hepatoblastoma (HB) largely depends on the achievement of radical surgical resection, even for metastatic tumors. However, the extension of the metastatic tumor when viewed through an endoscope with the conventional white-light mode is often unclear. Advancements in imaging technology utilizing indocyanine green (ICG) have facilitated precise resection of metastatic HBs, owing to the longer retention of ICG in such lesions than in other normal tissues.
Case:
We utilized an endoscope loaded with the PINPOINT system (NOVADAQ Technologies, Inc., Ontario, Canada), which allows for real-time overlay visualization with the same focal range between the white-light mode and near-infrared mode. Metastatic HBs that have taken up ICG are visualized as an area of green color superimposed on a high-definition white-light image. A 19-year-old female who underwent liver transplantation for an unresectable HB 2 years earlier was noted to have metastases on the diaphragm and the pleura. Preoperative magnetic resonance imaging showed metastatic HBs on the right pleura extending from the ribs and the diaphragm. The margin of the metastatic tumor was more sharply demarcated by the PINPOINT system than that detected in the normal white-light mode. The tumor was successfully resected en bloc with real-time guidance utilizing the overlay image. The alphafetoprotein levels were normalized and have remained within normal limits in the 12 months since the operation.
Conclusion:
Novel overlay imaging technology with ICG makes it possible to achieve real-time precise resection of metastatic HBs.
Introduction
I
We herein report for the first time navigation surgery for pleural metastasis with novel overlay technology that allows for real-time operation without switching visualization modes.
Case
We utilized the PINPOINT endoscopic fluorescence imaging system (NOVADAQ Technologies, Inc., Ontario, Canada), which allows for real-time overlay visualization with the same focal range between white-light mode and near-infrared mode. Metastatic HBs that have taken up ICG are visualized as an area of green color superimposed on a high-definition white-light image (overlay mode), which makes it possible for surgeons to perform real-time operations.
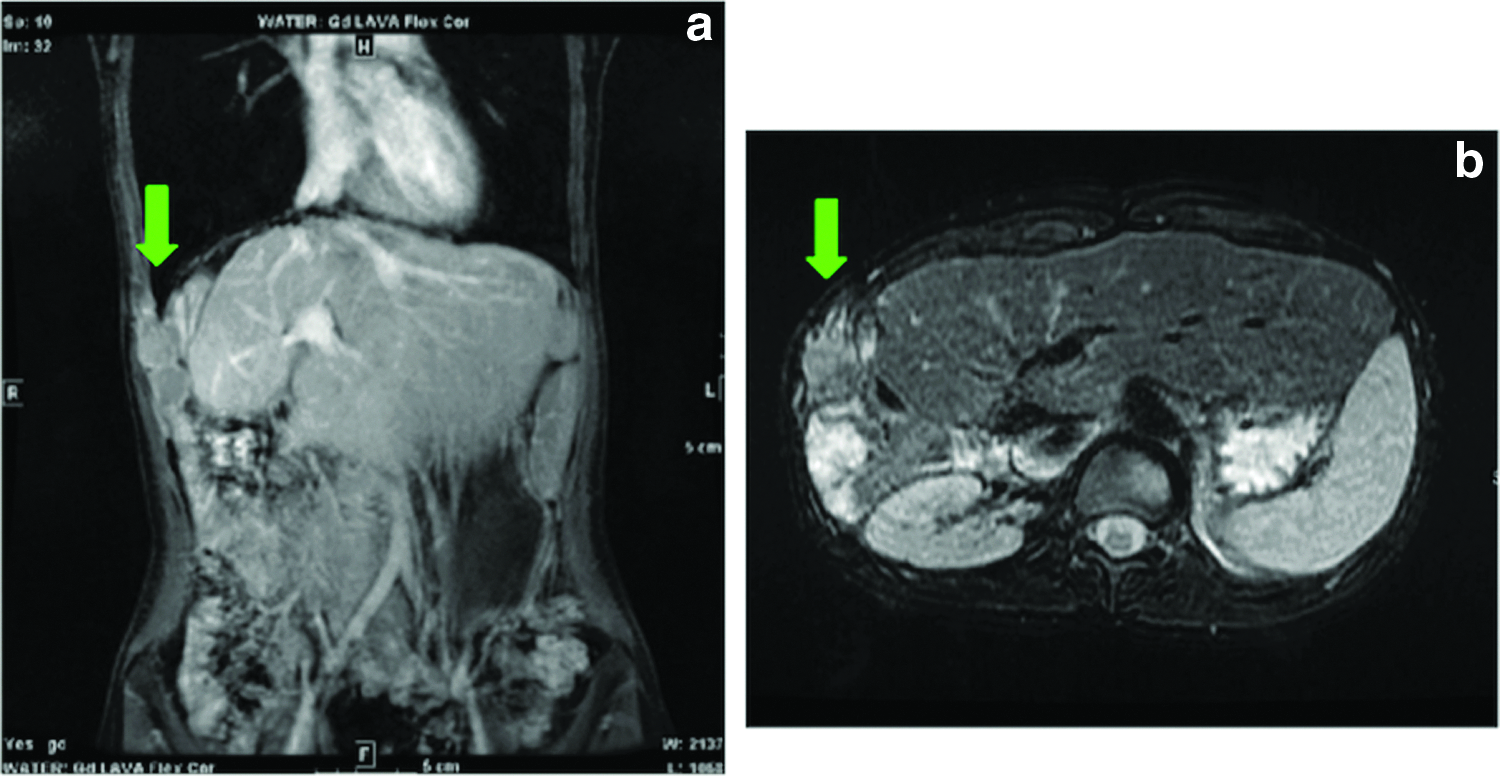
The patient was a 19-year-old woman who had initially presented with pretreatment extension III HB (wholly epithelial type and fetal subtype) at 18 years of age and underwent right trisegmentectomy with thoracotomy in an another institution. Later, the patient was referred to us and underwent liver transplantation (LTx) for recurrence in the remnant of the liver. The perioperative chemotherapy regimen was described in the SIOPEL 4 high-risk protocol. 2 Two years after LTx, the patient was found to have metastases in the right pleural cavity and the diaphragm. Figure 1a and b shows the magnetic resonance imaging findings before metastasectomy, that is, a mass with involvement from the 8th through the 10th ribs in the right pleural cavity along with part of the diaphragm. ICG (0.5 mg/kg; Diagnogreen; Daiichi-Sankyo Pharma, Tokyo, Japan) was given intravenously 72 hour before the operation. This study was approved by the institutional review board.
The patient was placed in the left decubitus position. The first and the second ports were inserted into the sixth and seventh intercostal spaces, respectively (Fig. 2). The PINPOINT imaging system provides a simultaneous single large view with three smaller views on the same screen, as shown in Figure 3a. The metastatic lesion that had taken up ICG was colorized as green in the overlay mode (white-light mode + near-infrared mode). The view from the anterior port is shown in Figure 3b, that is, the clear demarcation of HB in the rib under the overlay mode. The extent of the tumor in the overlay mode was more extensive than that shown in the normal white-light mode. Color-segmented fluorescence (CSF) was also used to image different levels of ICG uptake (Fig. 3c). A color scale on the side of the monitor shows the colors associated with the different levels of ICG uptake. CSF mode also helped us identify the tumor margin. The scale ranges from a low level of ICG uptake (gray = presumably tissues with no HB cells) to the highest level of ICG uptake (red). These colors are all relative and are based on the scale; thus, they are a useful guide for surgeons to draw a surgical margin.

The port layout is shown. The first and second ports were inserted through the sixth and seventh intercostal spaces, respectively.
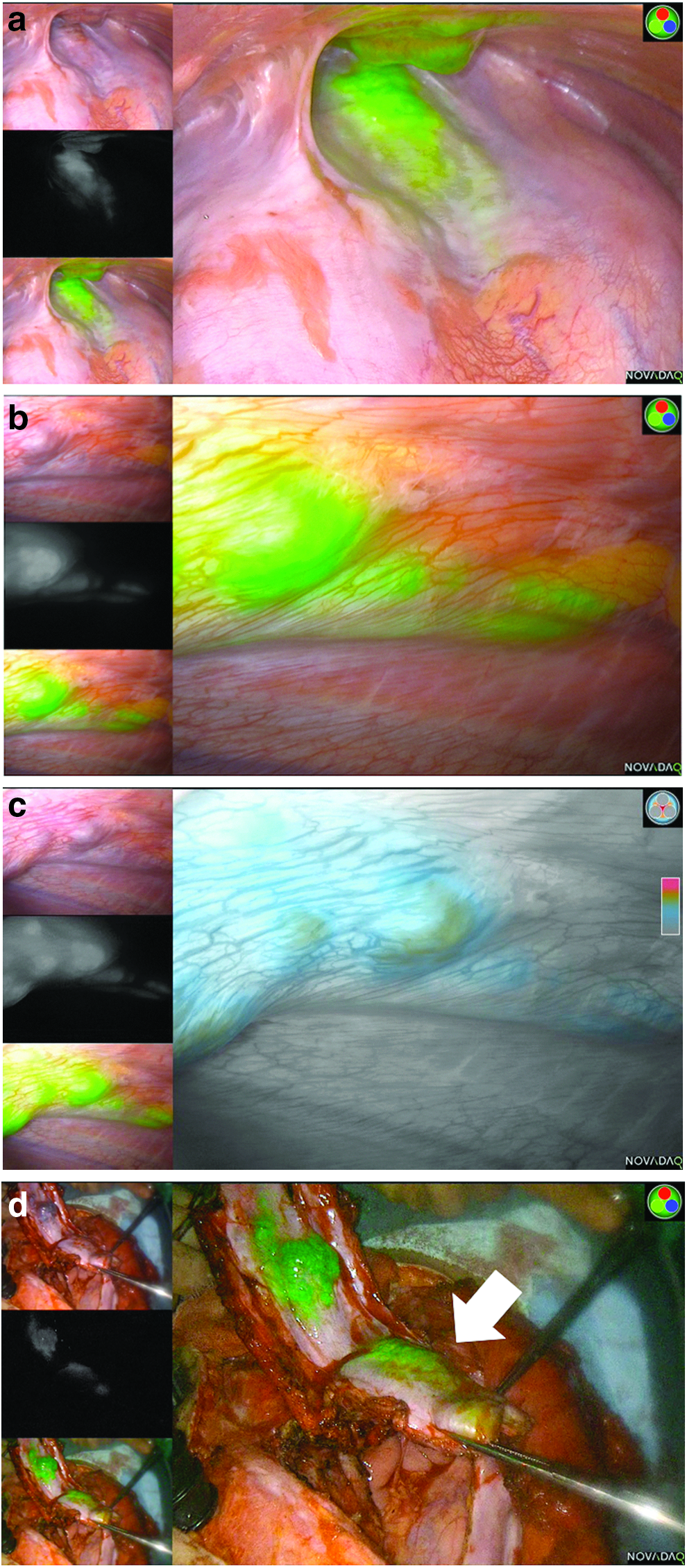
The tumor involving the 8th through the 10th ribs and the diaphragm were resected en bloc under the overlay mode with a safe margin from the green area (Fig. 3d). The intraoperative pathological diagnosis confirmed the negative surgical margins. The defect was reconstructed with a Goretex Soft Tissue Patch® (Supplementary Video S1; Supplementary Data available online at www.liebertpub.com/lap).
No adverse reaction to ICG was observed. The pathological findings in the area visualized as green were compatible with metastatic HB, and the surgical margin was confirmed to be negative. A histological map is shown in Figure 4. The upper picture is a specimen that was resected en bloc. The areas enclosed in the white squares correspond to the area inside the orange squares in the overlay mode as a reference (upper right). The cross section shown in the lower picture is the tumor map corresponding to the green line drawn in the upper picture. The areas marked with violet lines were pathologically proven to contain HB. The margin of the tumor in this section was identical to the green area in the overlay mode. The alphafetoprotein (AFP) levels were normalized after metastasectomy and have remained within normal limits in the 12 months since the operation.
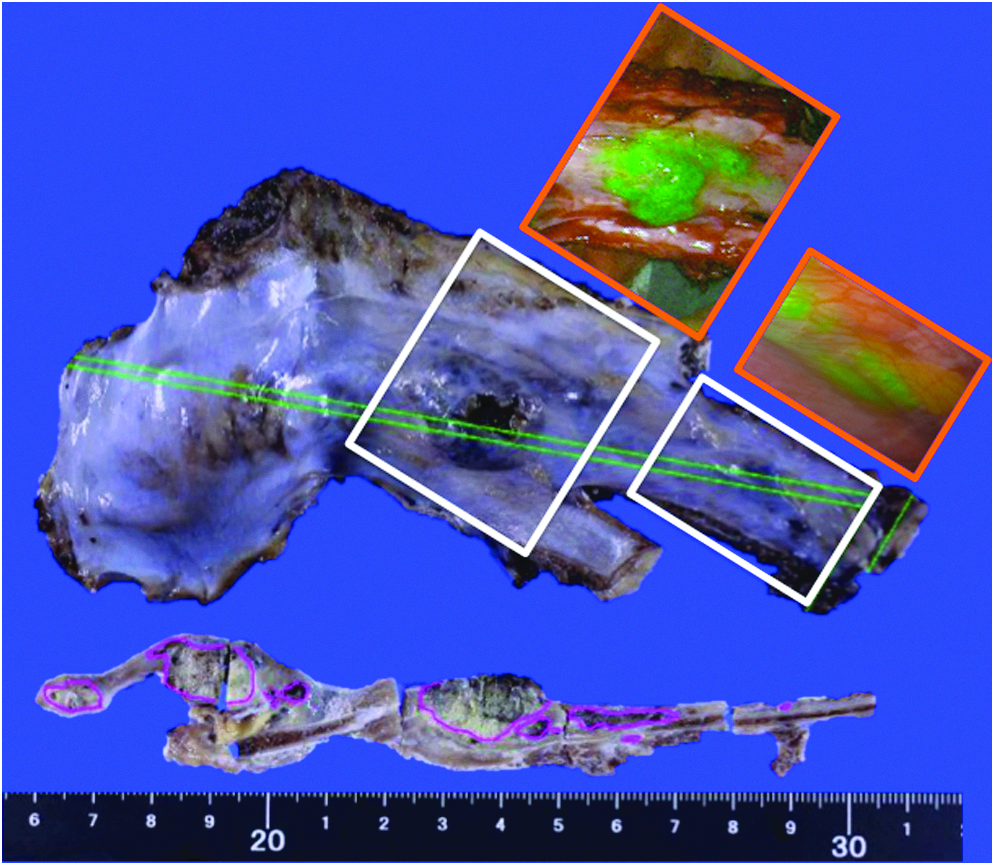
The upper picture is a specimen that was resected en bloc. The areas enclosed in the white squares correspond to the area inside the orange squares in the overlay mode as a reference (upper right). The cross section shown in the lower picture is the tumor map corresponding to the green line drawn in the upper picture. The areas marked with violet lines were pathologically proven to contain HB. The scale (cm) is shown at the bottom of the figure. HB, hepatoblastoma.
Discussion
For patients with HBs, complete surgical resection of all lesions, including chemotherapy-resistant lesions, is essential to achieve a survival outcome. ICG navigation surgery using a fluorescence imaging system is a useful tool for metastasectomy of HB. 3 We have performed several pulmonary metastasectomies with the Photodynamic Eye system® (Hamamatsu Photonics, Hamamatsu, Japan); however, surgeons must switch screens frequently between normal white-light mode and near-infrared mode when performing actual resection. In contrast, the PINPOINT system allows for a simultaneous overlay view of the normal white-light mode and near-infrared mode with the same focal range through a single endoscope, allowing surgeons to perform operations in real-time without frequent switching of the screens. This technique has already been applied to laparoscopic cholecystectomy to visualize biliary anatomy4,5 and colorectal surgery to assess the blood supply in the anastomosis. 6
In this patient, real-time navigation using an endoscope loaded with the PINPOINT system was extremely useful for achieving complete resection, as there was no other way to allow surgeons to see the precise extent of the metastatic tumor. The pleural dissemination of HB is a rare form of metastasis, so we suspect that the HB cells were implanted in the thoracic cavity at the time of the trisegmentectomy, since it involved thoracotomy.
The dosage and timing of ICG administration are a matter of debate. Based on previous reports and our own experience, we advise that 0.5 mg/kg of ICG be given 24 hours before surgery for lung metastases. Since normal hepatocytes take up ICG and excrete them into the biliary tract, we believe that ICG should be given at least 72 hour before an operation if the lesions lie in the abdominal cavity to minimize physiological emission from the normal liver tissue. In this specific case, ICG was given 72 hours before the operation because the metastatic tumor was located in the diaphragm, which was adjacent to the transplanted liver.
Several limitations associated with this technique should be mentioned. First, the false-positive rate with ICG navigation surgery is reported to be 10%–20% 1 (number of lesions that were not pathologically diagnosed as HBs among ICG-positive lesions). However, as ICG is sensitive enough to detect lesions as small as 0.062 mm in diameter, 1 it is technically difficult to prove the absence of HBs in specimens that are shown as positive in near-infrared mode. In addition, whether a lesion is positive or negative is up to the surgeon's subjective opinion. The CSF mode may solve this issue, since it allows for the imaging of different levels of ICG uptake and also helps surgeons to be as objective as possible. In this specific case, histologically proven HB cells were observed in the margin of the area visualized in the overlay mode. Second, the fluorescence produced by ICG can only be detected when the lesions are located 5–10 mm from the surface. Since HBs lying in deeper layers may go undetected in near-infrared mode, an intraoperative pathological analysis is still necessary to confirm a negative surgical margin. Whether or not this technique provides survival benefits remains to be elucidated in a larger cohort. Most importantly, our patient is now tumor free with a normal AFP, thanks to this novel navigation technique.
In conclusion, ICG navigation surgery in the overlay mode helps surgeons to identify the extent of the tumor and enables real-time metastasectomy for HBs.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.