
Abstract
Abstract
Background:
Hilar cholangiocarcinoma (HCCA) is a rare tumor, usually associated with obstructive jaundice and unfavorable prognosis. Obstructive jaundice can affect the liver, kidney, heart, and the immune system of the patients. Currently, controversy exists in whether preoperative biliary drainage (PBD) is of any benefit to the patients, and the best way for PBD in patients with resectable HCCA of malignant biliary obstruction remains to be determined.
Objectives:
To compare the clinical outcomes and effectiveness of endoscopic biliary drainage (EBD) treatment with those of percutaneous transhepatic biliary drainage (PTBD) treatment in patients with malignant biliary obstruction caused by resectable HCCA.
Materials and Methods:
The databases including MEDLINE, EMBASE, PubMed, CBM (China Biological Medicine Database), and CNKI were employed to identify the clinic trials on EBD versus PTBD for malignant biliary obstruction associated with resectable HCCA from January 2008 to October 2017. A systematic review and meta-analysis were carried out.
Results:
Six trials were identified and included in this study. Overall, the differences in technical success rate, R0 resection, incidence of total complication after resection, postoperative hospitalization time, resection time, and recurrence were not statistically significant between the EBD group and PTBD group (all P > .05). However, the incidence of total complications after EBD treatment is higher than that after PTBD treatment (P < .05).
Conclusion:
For patients with obstructive jaundice associated with HCCA, current evidence indicate no superiority of PTBD over EBD regarding clinical feasibility and success rate, but data suggest a better clinical safety of PTBD compared with EBD in short-term postoperation. In long-term evaluation, the differences in clinical outcomes are not statistically significant between PTBD and EBD.
Introduction
H
With the continuous development of endoscopic biliary drainage (EBD) and percutaneous transhepatic biliary drainage (PTBD), great changes have taken place in traditional operative concepts and technologies, and the concept of minimally invasive treatment is being developed and established, especially for obstructive jaundice with unresectable or resectable tumor. Therefore, endoscopic or PTBD has become the first choice for obstructive jaundice associated with unresectable tumors. However, the supply of equipment and skilled operators varies from one institution to another. Moreover, the timing of intervention greatly relies on the judgment of attending doctors based on patient clinical symptoms. Therefore, controversy remains over the optimal approach to PBD in patients with malignant biliary obstruction associated with resectable HCCA.
In a more recent study including 320 patients randomized to either endoscopic/external drainage or direct surgery without stenting, no significant difference in outcomes was observed between the two groups, although subgroup analysis of patients in group EBD showed higher incidence of total complications. 4 Further, another two studies5,6 found no association between mortality and preoperative stenting, and one of the studies 5 reported a significant decrease in postoperative complications after preoperative stent implantation. In this study, we aim to explore the optimal approach for PBD in obstructive jaundice patients with resectable HCCA through a systematic review and meta-analysis on existing evidence.
Materials and Methods
Search strategy and identification of studies
Relevant articles were identified within the electronic databases including MEDLINE, EMBASE, PubMed, CBM, and CNKI. The search strategy contains publication time (January 1990–October 2017), language (English or Chinese), and key words (“endoscopic”, “percutaneous”, “biliary drainage”, “hilar cholangiocarcinoma”, “preoperative,” and “complication” used in various combinations). To include all the qualified studies as much as possible, the reference lists of all relevant publications and review articles were manually checked. For two or more studies from the same institution, only the most detailed reports are included.
Data extraction and quality assessment
Data was extracted by three separate authors (Liu Jun-guo, Wu Jing, and Wang Jun) using standardized forms. The data including the number of patients, R0 resection, and total complications after resection, postoperative hospital time, resection time, and recurrence after resection was recorded. According to nonrandomized controlled clinical trail quality evaluation standard, the quality of all selected studies was graded (Table 1).
According to the Newcastle-Ottawa Scale NOS for assessing the quality of nonrandomized studies, > = 5* is divided into meta-analyses.
NOS, Newcastle-Ottawa scale.
Selection criteria of trials
Inclusion criteria for this study were as follows: (1) Randomized or nonrandomized controlled study based on EBD versus PTBD; (2) All selected patients in the trails were with resectable HCCA; (3) The data about patient number, technical success, total complications after PTBD or EBD treatment (cholangitis, bleeding, tube dislocation, pancreatis, injury of portal vein, or cancer dissemination), R0 resection, total complications after resection (bile leakage, abscess, hepatic insufficiency, sepsis, or In-hospital death), postoperative hospital time, resection time, and recurrence after resection were reported and can be retrieved; (4) Controlled trial with follow-up.
Statistical analysis
Odds ratio (OR) with 95% confidence interval (CI) were used by the dichotomous data of the studies eligible for meta-analysis. The data were combined for meta-analysis in a fixed effects model, or in a random effects model.
With respect to continuous data, the differences across the studies were pooled and presented as a weighted mean difference (WMD) with 95% CI. The inverse variance method and the DerSimonian and Laird method were used in a fixed effects model and a random effects model, respectively.
All statistical analyses were performed by using Revman Software Version 4.2. The study of variation is used in Chi-square test (the result of hypothesis testing is that all studies come from the same population, i.e., the same size of the population). Statistical heterogeneity was defined as P < .05 or I2 > 50%. When there is no heterogeneity, the fixed effects model is used, or the random effect model is applied in the presence of significant heterogeneity. To detect potential publication bias, a funnel plot analysis and Egger test were performed. The statistical significant level was P < .05.
Results
Description of included trials
According to the exclusion and inclusion criteria, six studies7–12 including one 8 published in a Chinese journal were selected into this meta-analysis, containing 379 patients in the EBD group and 286 patients in the PTBD group. The characteristics of the six clinical trials are shown in Table 1. The total incidence rates of cholangitis in the EBD group and the PTBD group from five studies7–11 are 27.8% (93/334) and 20.9% (51/244), respectively. The total incidence of cholangitis in the PTBD group is lower than that in the EBD group. The total incidence rates of bleeding in the EBD group and in the PTBD from four studies7,8,10 are 3.2% (5/157) and 3.7% (4/108), respectively and it showed that the PTBD group is higher than that in the EBD group. A combined analysis of four studies7–10 show that the total incidences of pancreatis in the EBD group is 11.9% (21/157), in contrast to none in the PTBD group. The total incidence rates of dislocation after EBD and that after PTBD from three studies7–9 are 18.1% (32/177) and 7.7% (12/156), respectively. The total incidence of dislocation after PTBD is lower than that after EBD. With the data from five studies,7–10,12 the incidence rates of total complications after PTBD and that after EBD are 25.6% (51/199) and 53.9% (125/232) respectively. The incidence of total complications after PTBD is lower than that after EBD.
The total incidence rates of R0 Resection after EBD and that after PTBD from two studies10,12 are 77% (57/74) and 77.8% (77/99), respectively. Total incidence of R0 Resection after PTBD is higher than that after EBD.
The total incidence rates of bile leakage after EBD and that after PTBD from two studies10,12 are 5.4% (5/92) and 7.0% (7/99), respectively. Total incidence of cholangitis after PTBD is higher than that after EBD. The total incidence rates of hepatic insufficiency in the EBD group and the PTBD group from three studies9,10,12 are 8.0% (9/112) and 10.2% (15/147), respectively, being higher after PTBD. The data of three studies9,10,12 indicate that the total incidence rates of abscess after EBD treatment and after PTBD treatment are 12.5% (14/112) and 8.8% (13/147), respectively. Total incidence of abscess in the PTBD group is lower. The total in-hospital death rates in the EBD group and the PTBD group from two studies9,12 are 7.4% (5/68) and 9.4% (8/85), respectively, with a higher death rate in the PTBD group. The total incidence rate of complication after resection from three studies9,10,12 is 27.7% (31/112) versus 27.2% (40/147) for EBD versus PTBD.
The total incidence of recurrence after resection for EBD versus PTBD from three studies10–12 is 30.3% (67/221) versus 39.8% (74/186), being higher in the PTBD.
Meta-analysis
The synthesized evidence indicate that the differences between the EBD group and the PTBD group were not statistically significant in technical success (OR = 0.57, 95% CI: 0.30–1.09, P = .09, Fig. 1), dislocation (OR = 1.86, 95% CI: 0.84–8.14, P > .05, Fig. 2), bleeding (OR = 1.2, 95% CI: 0.36–4.02, P = .77, Fig. 2), cholangitis (OR = 2.13, 95% CI: 0.31–14.52, P = .44, Fig. 3), R0 resection (OR = 1.07, 95% CI: 0.06–19.52, P = .96, Fig. 4), total complication after resection (OR = 0.87, 95% CI: 0.49–1.55, P = .64, Fig. 5), bile leakage (OR = 0.67, 95% CI: 0.21–2.21, P = .51, Fig. 5), hepatic insufficiency (OR = 0.77, 95% CI: 0.32–1.83, P = .55, Fig. 5), abscess (OR = 1.69, 95% CI: 0.73–3.89, P = .22, Fig. 5), in-hospital death (OR = 0.63, 95% CI: 0.19–2.1, P = .45, Fig. 5), postoperative hospital time (WMD = 0.29, 95% CI: −4.07 to 4.64, P = .90, Fig. 6), resection time (WMD = 19.42, 95% CI: −9.58 to 48.41, P = .19, Fig. 7), and recurrence after resection (OR = 1.02, 95% CI: 0.63–1.65, P = .94, Fig. 8). To be noticed, there were differences between the EBD group and the PTBD group in the total complications (OR = 3.13, 95% CI: 1.96–5.01, P < .05, Fig. 2) and pancreatis (OR = 11.52, 95% CI: 2.59–51.30, P < .05, Fig. 2).
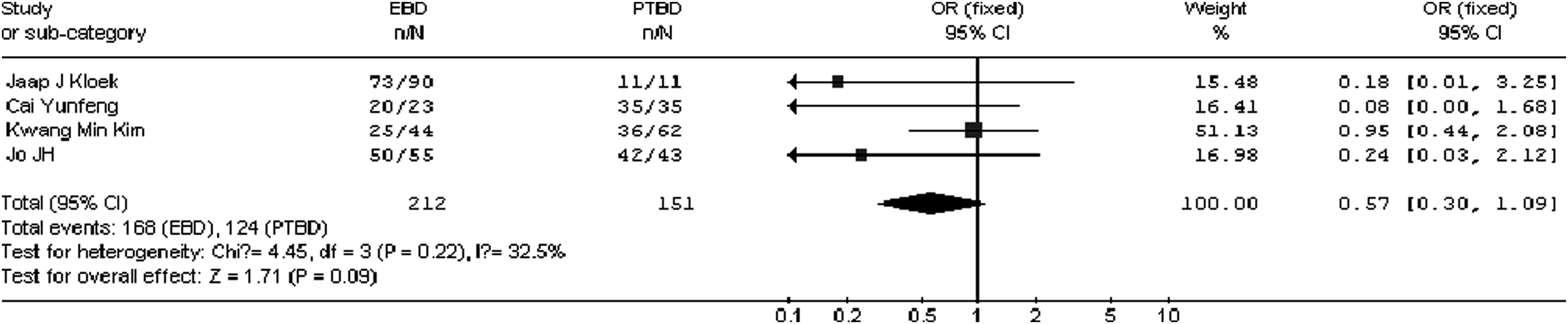
The fixed effects model of OR for technical success after treatment for the EBD group versus PTBD group. CI, confidence interval; EBD, endoscopic biliary drainage; OR, odds ratio; PTBD, percutaneous transhepatic biliary drainage.

The fixed effects model of OR for complication after treatment for the EBD group versus PTBD group. CI, confidence interval; EBD, endoscopic biliary drainage; OR, odds ratio; PTBD, percutaneous transhepatic biliary drainage.
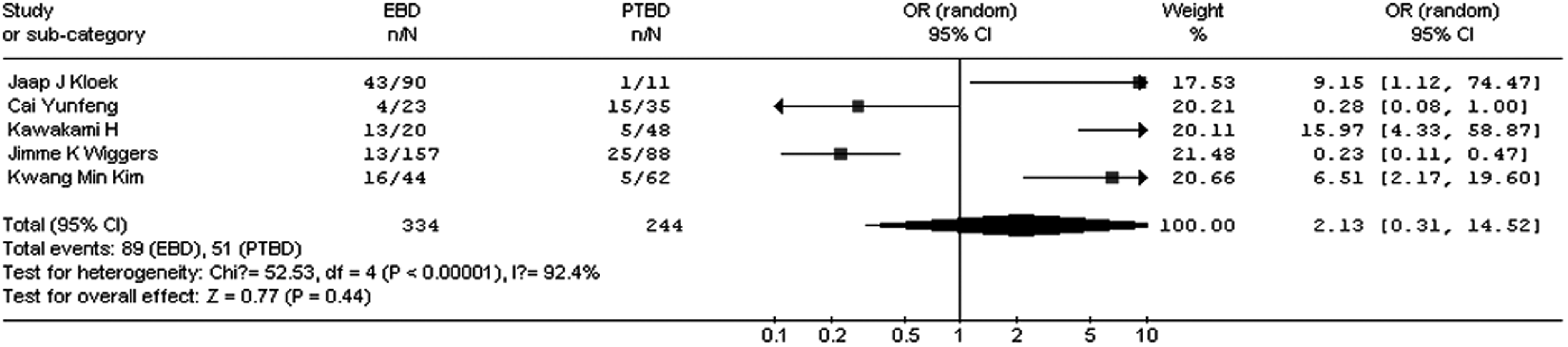
The fixed effects model of OR for cholangitis after treatment for the EBD group versus PTBD group. CI, confidence interval; EBD, endoscopic biliary drainage; OR, odds ratio; PTBD, percutaneous transhepatic biliary drainage.

The random-effect model of OR for R0 resection after treatment for the EBD group versus PTBD group. CI, confidence interval; EBD, endoscopic biliary drainage; OR, odds ratio; PTBD, percutaneous transhepatic biliary drainage.
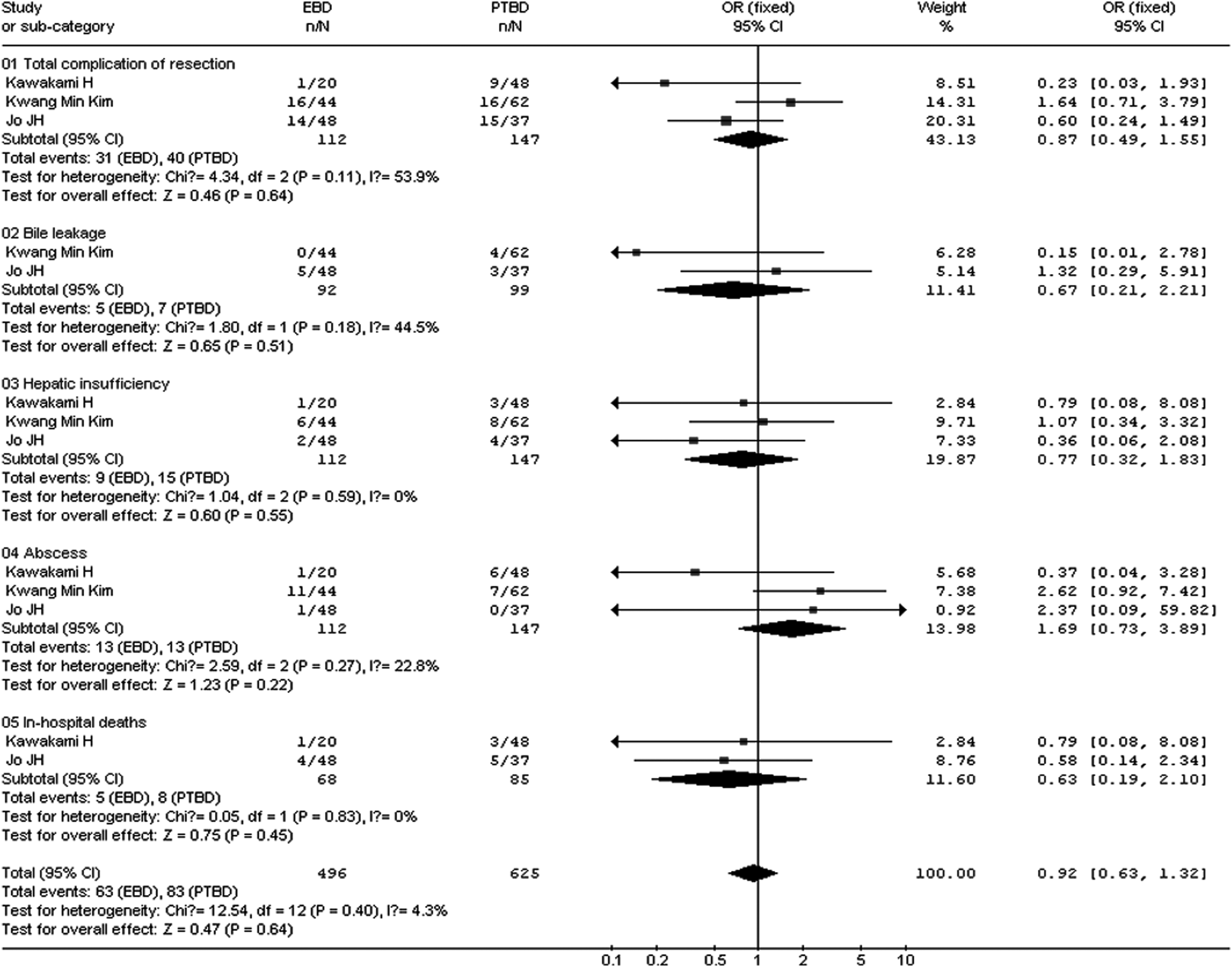
The fixed effects model of OR for complication after resection for the EBD group versus PTBD group. CI, confidence interval; EBD, endoscopic biliary drainage; OR, odds ratio; PTBD, percutaneous transhepatic biliary drainage.

The fixed effects model of OR (WMD) for postoperative hospital time for the EBD group versus PTBD group. CI, confidence interval; EBD, endoscopic biliary drainage; OR, odds ratio; PTBD, percutaneous transhepatic biliary drainage; SD, standard deviation; WMD, weighted mean difference.

The fixed effects model of OR (WMD) for resection time for the EBD group versus PTBD group. CI, confidence interval; EBD, endoscopic biliary drainage; OR, odds ratio; PTBD, percutaneous transhepatic biliary drainage; SD, standard deviation; WMD, weighted mean difference.
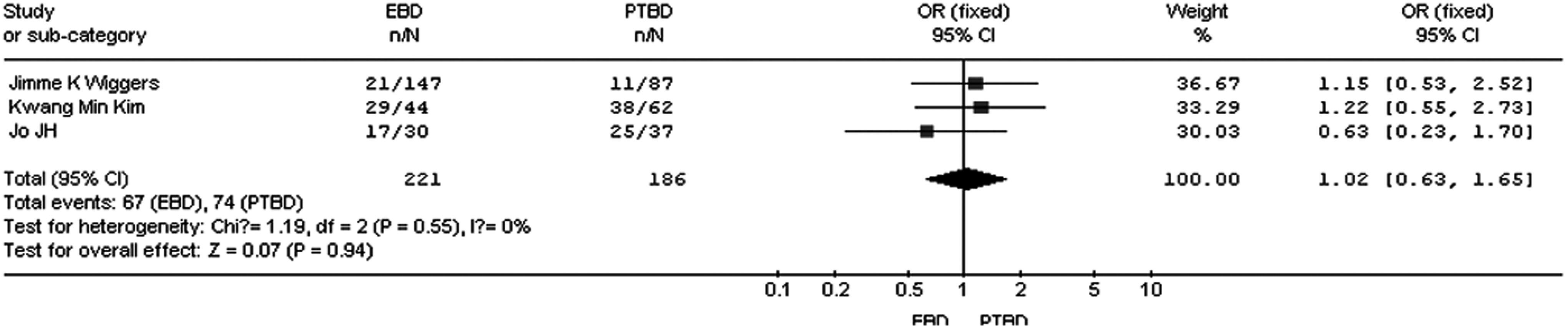
The fixed effects model of OR for recurrence after resection for the EBD group versus PTBD group. CI, confidence interval; EBD, endoscopic biliary drainage; OR, odds ratio; PTBD, percutaneous transhepatic biliary drainage.
Sensitivity analysis and publication bias
The funnel plots on technical success, cholangitis, bleeding, tube dislocation, pancreatis, total complications after PTBD or EBD treatment, R0 resection, total complications after resection, bile leakage, abscess, hepatic insufficiency, postoperative hospital time, resection time and recurrence after resection following EBD or PTBD treatment showed basic symmetry, which suggested no publication bias.
Discussion
HCCA, as the most common type of bile duct cancers, is a rare malignancy. The incidence of HCCA has remained stable over the past 3 years, and there are about 7000 new cases every year in North America. Primary sclerosing cholangitis, liver fluke infestation (Clonorchis sinensis and Opisthorchis viverrini) and hepatolithiasis were known as risk factors associated with HCCA. But most cases are sporadic without an apparent inciting factor. 13 Patients usually show cachexia, fatigue, and jaundice, often reflecting locally advanced or metastatic disease. About 90% of the patients had biliary tract symptoms, and painless jaundice was the most common. Up to 10% will have concomitant cholangitis. 14 As HCCA often has already progressed to an advanced stage at diagnosis and effective systemic agents are lack, most patients succumb within a year after diagnosis.
As far as it is known that radical resection of the tumor is the only feasible treatment for cure. However, most patients with HCCA show liver dysfunction caused by obstructive jaundice, which has been proved to be an important risk factor in lobectomy.15–17 Lai et al. 18 and Su et al. 19 reported that hepatectomy in patients with jaundice had a high incidence of morbidity and mortality. Therefore, PBD has always been advocated before radical operation to reduce morbidity and mortality.20–23 In the late 1970s, some studies on PBD reported that postoperative death rate was reduced in jaundiced patients.24,25 For patients with hyperbilirubinemia, which is associated with jaundice, cholangitis, malnutrition, liver or renal insufficiency, PBD is needed for preoperative antineoplastic therapy and the preparation for portal vein embolization. 26
EBD or PTBD can achieve the decompression of the bile duct for HCCA. In addition to reducing procedural risks and need to intervene again, the percutaneous transhepatic cholangiography catheter can provide a better delineation of the extent of endobiliary tumor spread in the liver resection plan.27–29 In addition, the time, as a measure of the success of technology, is from the first attempt to a satisfactory level of biliary tract, and the use of PTBD was more obvious (44 days) than using EBD (61 days). More than half of patients who initially received EBD would require PTBD later to achieve the anticipated therapeutic effect. 30 However, complex lesions may not completely respond to endobiliary drainage. Especially in patients who may be suitable for surgical resection, the medical team should not hesitate to establish durable biliary drainage through percutaneous catheter.
Although the discomfort of the patient is imposed by nasal drainage, endoscopic nasobiliary drainage is a better way to improve the durability and reduce cholangitis compared with endobiliary stenting. And it was recommended as an ideal preoperative drainage method. 9
This study suggests that the differences in most clinic outcomes were not statistically significant between the EBD and the PTBD treatment for patients with resectable HCCA. Of note, the PTBD group generally had less total complications compared with the EBD group. In patients with malignant biliary obstruction caused by resectable HCCA, the difference in recurrence after resection was not statistically significant between the EBD and PTBD groups (P > .05). The resection time and postoperative hospitalization time were not statistically significant either between the EBD and the PTBD group (P > .05). Taken together, PTBD may be more effective and more suitable for the treatments of resectable HCCA.
Stratified analysis was not performed because of other possible confounding factors in this study. Therefore, the conclusions drawn here need more detailed data for further validation. But according to the data and literature, PTBD does have advantages compared with EBD. Up to date, EBD versus PTBD in patients with resectable HCCA has been carried out only in a small number of cases for a short time period. Randomized controlled trials containing much larger cohorts with more standardized evaluation for certain outcomes (e.g., technical success and complications) are expected. Plus, it needs to be pointed out that surgeon's experience could also affect the comparison between PTBD and EBD.
An institution bias may exist in our study, and we speculate that this is probably due to the high requirements to conduct clinic studies of PTBD versus EBD, in which an institute should be able to provide both options for the patients. However, the fact is that EBD and PTBD are not easy to do at every institution, and they are not routinely taught in surgical residency or even advanced fellowship. Although EBD and PTBD are used more frequently for treating obstructive jaundice caused by unresectable or resectable tumor, they are both highly skill-demanded operation and we suggest that surgeons who are not proficient with them should operate under supervision for the sake of clinic safety.
Footnotes
Disclosure Statement
No competing financial interests exist.