
Abstract
Abstract
Background:
Class III obesity is a global health emergency associated with an increase in the incidence of many other diseases such as type 2 diabetes mellitus, hypertension, hyperlipidemia, cancer, obstructive sleep apnea, nonalcoholic fatty liver disease, osteoarthritis, infertility, and mental health disorders. Minimal work has been published regarding the efficacy of laparoscopic sleeve gastrectomy (LSG) in the veteran population to surgically manage morbid obesity.
Design:
Retrospective analysis of LSG performed at a Veterans Affairs Medical Center (VAMC) between 2010 and 2017. Veterans were followed from their enrollment in the bariatric program until twelve months following LSG. The primary outcome of interest was excess and total weight loss with resolution of associated comorbidities.
Results:
Excess weight loss at nine and 12 months was 43.5% and 40.7% and total weight loss was 20.1% and 19.0%, respectively. LSG performed at a VAMC resulted in 86.9% improvement in type 2 diabetes mellitus and a 66.1% improvement in hypertension and 74.3% improvement in hyperlipidemia. Approximately 10.0% of diabetics obtained partial and 9.0% obtained complete resolution of their disease. Similarly, 22.0% of Veterans obtained partial and 13.0% obtained complete resolution from hypertension. Complete resolution from hyperlipidemia was achieved in 8.8% of Veterans. There were no postoperative complications or staple line leaks.
Conclusion:
LSG is a safe and effective tool for morbid obesity with clinical and serological improvements for individuals who are unable to lose weight with medical management alone.
Introduction
B
Weight loss following sleeve gastrectomy is accomplished by both mechanical and neurohumoral pathways. Mechanically, gastric volume is restricted and gastric emptying is increased. As nutrients are introduced to the small intestine at an accelerated rate, the gut upregulates gastrointestinal hormones. Current research suggests that upregulation of both glucagon-like peptide-1 and peptide YY following bariatric surgery plays the largest role in neurohormone-mediated weight loss.5–8 While initially thought to have a large role in surgical weight loss, the effect of plasma ghrelin levels is marginal. The combination of the mechanical and neurohormonal changes leads to significant weight loss and can resolve obesity-related comorbidities such as diabetes, hyperlipidemia, and hypertension.9–15
Recently, the early outcomes of LSG in a Veterans medical center was published in 2012 and involved a cohort of 50 veterans who were followed for an average of 10 months. The results showed improvements in body mass index (BMI), fasting glucose, hemoglobin A1C (HgBA1c), and serum lipid values in addition to a decrease in the number of daily medications. 16 Since that report, the American Society for Metabolic and Bariatric Surgery (ASMBS) has issued guidelines for reporting success for weight loss surgery. These guidelines include: definitions for follow-up periods comprised of short (< 3 years), medium (>3 and < 5 years), and long (>5 years); metrics for evaluating improvement of comorbid diseases such as diabetes, hypertension, and hyperlipidemia based on serological improvements with or without medication improvement; metrics for evaluating improvement in obstructive sleep apnea and gastroesophageal reflux based on objective improvements in polysomnography or pH studies and subjective improvements in validated questionnaires; and definitions of major and minor postoperative complications. The purpose of this analysis was to benchmark the outcomes of LSG at a single Veterans Affairs Medical Center (VAMC) based on the most recent ASMBS guidelines.
Materials and Methods
The Institutional Review Board at the VAMC in Washington, DC approved a retrospective review of a prospectively maintained database of veterans enrolled in a bariatric surgery weight loss program at a single VAMC within Veteran Integrated Service Network (VISN) 5. Veterans who underwent LSG by a single surgeon between 2010 and 2017 were captured using the Computerized Patient Record System and Veterans Information Systems and Technology Architecture (VISTA) network. Veteran demographics, comorbidities, medications, serologies, and operative details were gathered encompassing six months before and 12 months post LSG.
Before surgery, all veterans were enrolled in either the MOVE! or the teleMOVE! Weight Management Program at the Washington, DC VAMC. 17 MOVE! utilizes preoperative counseling and medical management, including weekly in-person group sessions, whereas teleMOVE! includes remote daily interaction with in-home messaging. Within VISN 5, prediabetic and diabetic veterans are also offered weight loss counseling and services (LIVe Program). The Veterans Health Administration also covers antiobesity prescription medications for medically qualifying veterans.
Standardized outcomes of LSG were based on the guidelines set by the ASMBS published in 2015. 5 Briefly, improvement was defined by reduction in the degree of severity of comorbidity without an increase in medical therapy; partial resolution encompassed a reduced degree of severity in comorbid conditions without need for medical therapy; and complete resolution indicated a return to normal serological markers without need for medical therapy. The primary outcomes included total and excess weight loss and improvements or resolution of comorbid diseases. Secondary outcomes included perioperative outcomes focused on establishing the safety of the LSG at a VAMC for weight loss. Statistical analysis utilized chi-squared test for categorical data and t-tests for continuous data. Statistical processing was performed with IBM SPSS version 24 with P < .05 holding significance.
Surgical technique
A small incision is made in the left upper quadrant, and a Veress needle is inserted. The abdomen is insufflated to 15 mmHg with carbon dioxide. Subsequently, a 5-mm visual port is passed through the left upper quadrant incision and diagnostic laparoscopy is performed. A 12-mm port is then placed in the midline 20 cm from the xiphoid; additional 5-mm ports are placed in the left flank, the right upper quadrant, and subxiphoid, the latter for liver retraction. A point 10 cm from the pylorus is ascertained along the greater curvature of the stomach. The gastrocolic ligament, greater omentum, and short gastric vessels are divided with the Harmonic scalpel. The dissection proceeds toward the angle of His. Hemostasis is maintained throughout as the short gastric vessels are divided. Subsequently, a 42-French bougie is introduced through the gastroesophageal junction and passed toward the pylorus. Sequential staplers are utilized to divide the stomach at the level of the angle of His. The fundus is completely excluded. The bougie is removed, and the staple line is tested with air insufflation and methylene blue. Surgical clips are placed along the staple line to ensure hemostasis as needed. Subsequently the staple line is secured to the divided gastrocolic ligament to prevent torsion of the sleeve. The specimen is then extracted from the 12-mm port site, and this port site is then closed with a series of 0-Vicryl fascial stitches.
Veterans are transferred to the recovery room and then to a ward or intensive care unit based on comorbidities. On postoperative day number one, the veterans are advanced to a clear liquid diet. Depending on each veteran's dietary progress, they are discharged on postoperative day number two or three. Each veteran is seen as an outpatient in 1 week and then at 3, 6, 9, and 12 months. A bariatric laboratory panel is obtained at 6 and 12 months.
Results
The results of the first 100 veterans enrolled in the VAMC Bariatric Weight Loss program were evaluated, of which 12-month follow-up data were available for 57 veterans. All veterans underwent a LSG after completing the medical-based portion of the VAMC Bariatric Weight Loss program. The mean age at the time of surgery was 50 years, the mean BMI at initial appointment was 42.36 kg/m2 and 41.0% of Veterans enrolled in the program were male (Table 1). Veteran comorbidities were as follows: 57% hypertension, 57.0% obstructive sleep apnea, 53.0% type 2 diabetes mellitus, 29.0% smoking, 50.0% prior abdominal surgery; and 10.0% of Veterans had a concomitant hiatal hernia at the time of surgery.
Continuous variables reported as means, categorical variables reported as percentages.
SEM, standard error of the mean.
There was one preoperative complication due to multiple failed intubation attempts. The veteran was rescheduled. Overall, there were no major intraoperative or postoperative complications. There were no staple line leaks (Table 2). Mean operative time was 94.52 minutes with minimal blood loss (18.55 cc) and no Veterans required transfusions intra- or perioperatively. The average length of stay was 2.31 days and the readmission rate was 1.0%. The single readmission within 30 days of sleeve gastrectomy was secondary to constipation. The veteran received multiple enemas with subsequent return of normal bowel function before discharge. Perioperatively, 5.0% of veterans were treated for a superficial wound infection. The five individuals diagnosed with wound complications had a minor dehiscence of the skin at their supraumbilical midline laparoscopic port site. Each veteran was treated with antibiotic ointment and no wound hernias have developed to date.
Postoperative complication does not include wound complications. Continuous variables reported as mean, categorical variables reported as percentages.
Postoperative complication relates to morbidity during index hospital admission.
Paired testing of serologies and medication burden showed a statistically significant improvement from preoperative to postoperative values in HgBA1c (6.94 versus 6.17, P < .001), serum high-density lipoproteins (HDL) (47.25 versus 51.9, P < .001), serum glucose measured at first follow-up (115.51 versus 105.14, P = .038), and a trend toward a significant decrease in serum triglycerides (128.82 versus 109.07, P = .053). There were no statistically significant changes in the number of individuals taking antihypertensives, oral hyperglycemic agents, insulin, or statins. There was no significant difference in cholesterol and low density lipoproteins (LDL) levels (Table 3). Excess weight loss at nine and 12 months was 43.5% and 40.7% and total weight loss was 20.1% and 19.0%, respectively (Table 4). The trend in average BMI as a function of time is displayed in Figure 1. The preoperative MOVE! or teleMOVE! program alone contributed to overall BMI reduction by 1.45 (SEM 0.179) compared with overall BMI reduction by 6.52 (SEM 0.357) from LSG and continued lifestyle changes. There was no incidence of recidivism at 12 months, defined as individuals whose BMI following surgery surpassed their BMI before surgery.
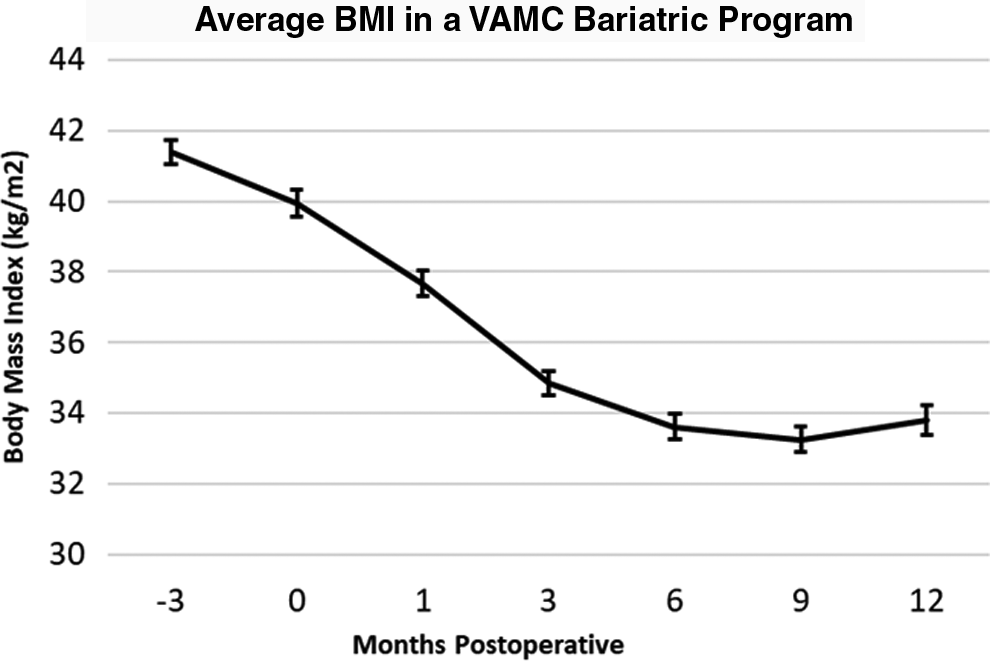
Average BMI of veterans enrolled in the VAMC bariatric surgery program. BMI reported in kg/m2. BMI, body mass index; VAMC, Veterans Affairs Medical Center.
Postoperative serum glucose measured at first follow-up. Postoperative hemoglobin A1c and cholesterol panel measured within 6–12 months following index operation. Postoperative medication burden analyzed at time of 3–6 month follow-up. Continuous variables reported as mean, categorical variables reported as percentages.
HDL, high density lipoproteins; LDL low density lipoproteins.
Formulas for each column are: excess weight loss = [(initial weight) − (postoperative weight)]/[(initial weight) − (ideal weight)]× 100; total weight loss = [(initial weight) − (postoperative weight)]/[initial weight]× 100.
Based on criteria set forth by the ASMBS 5 and detailed in the methods section, LSG performed at a VAMC resulted in 86.9% improvement in type 2 diabetes mellitus, a 66.1% improvement in hypertension, and 74.3% improvement in one or multiple aspects of their lipid panel. Furthermore, 9.9% of diabetics obtained partial and 8.6% obtained complete resolution of their disease. Similarly, 22.4% of Veterans obtained partial and 13.2% obtained complete resolution from weight-related hypertension. Complete resolution from hyperlipidemia was achieved in 8.8% of Veterans (Table 5).
Brethauer et al. (2015).
ASMBS, American Society for Metabolic and Bariatric Surgery.
Discussion
This analysis illustrates that the LSG is an effective form of weight loss surgery for veterans unable to lose weight or resolve obesity-related comorbidities using diet, exercise, or medical management alone. Furthermore, the LSG is a safe procedure with a low postoperative complication profile. Veterans enrolled in the bariatric weight loss program at the VAMC had a significant improvement in hypertension, diabetes, and hyperlipidemia with modest rates of complete resolution from disease.
Compared with medical management alone, recently published studies have validated the long-term benefits of bariatric surgery in decreasing and resolving hyperglycemia. 18 From a cost perspective, bariatric surgery has been shown to decrease overall healthcare costs for patients suffering from obesity compared with medical management. 19 Direct cost savings are derived from the reduction or resolution of diabetes, hypertension, hyperlipidemia, gastroesophageal reflux disease, and arthritis and average between $5000 and $10,000 per patient based on institution and duration of follow-up.20–22 Indirect cost savings stem from the reduction in risk for cardiovascular disease, 23 certain cancers, 24 and degenerative joint and bone diseases.
Comparing the LSG to the RYGB, both procedures provide similar short- and long-term weight loss, both procedures have similar degrees of recidivism with prolonged follow-up, but the resolution of weight-associated comorbidities favors RYGB.7,22,25 By comparison, the rate of postoperative complications and reoperation following the LSG is significantly lower than a RYGB.22,26 Nutritional deficiencies following either LSG or RYGB is still debated with small cohort studies reporting no difference or a slight improvement for LSG versus RYGB.27–29 Given the improved safety of the LSG with the equivocal improvement in excess weight loss, the LSG was adopted for the bariatric weight loss program at our VAMC.
Early studies analyzing the efficacy of the LSG as a primary surgical option for veterans suffering from morbid obesity documented the efficacy and safety of the LSG with a significant reduction in medications for hypertension, diabetes, and hyperlipidemia. 30 Since then, there have been comparisons between LSG and RYGB within the veteran population. These studies validate findings seen in the private sector and concluded that both the LSG and RYGB are safe, but that weight loss is slightly improved with RYGB. 31 The results of this analysis support the conclusion that LSG is a safe and effective method for surgical weight loss for veterans unable to lose weight by medical treatment alone.
We believe that the LSG has a lower overall morbidity compared with malabsorptive bariatric procedures such as the RYGB. Due to the nature of the procedure, LSG has a significantly lower incidence of internal hernia formation and marginal ulceration. The lack of gastrointestinal anastomoses as well as the utility of current-generation laparoscopic stapling devices has also led to a relatively low leak rate. While we accept that the weight loss may not be as robust as a RYGB, LSG is associated with fewer long-term adverse events.
Our program has the benefit of a single surgeon performing all of the procedures. Due to the relative ease of the LSG and the small learning curve, the procedure could be rapidly adopted at any VA medical center with appropriate staff and resources. Despite access to healthcare throughout the VA system, many veterans suffer from obesity and its complications. Unfortunately, access to minimally invasive or bariatric surgeons within the VA system is limited for many veterans. Based on the outcomes of this study and other series, minimally invasive bariatric surgery should be offered to veterans across the nation.
The limitations of this study stem from the fact that the results are retrospective and come from a single center. While the bariatric surgery database is maintained prospectively, the desired clinical endpoints were obtained in a retrospective fashion and subject to bias from incomplete outcomes. Despite the broad-reaching follow-up capabilities of the VAMC network, one-year follow-up data were only available for 57.0% of veterans enrolled in the program. In addition, this analysis only evaluated veterans receiving surgery at a VAMC and may not be generalized to the private sector. It is also important to note that surgeon experience may be underrepresented as the primary surgeon has 20 years of laparoscopic experience. This aspect may have artificially improved the reported safety profile of the LSG in the veteran population.
Considering the conclusions of this analysis, we recommend that veterans who are unable to resolve obesity-related comorbidities by nonsurgical methods be considered for LSG. The LSG is a low-risk procedure with moderate excess weight loss and moderate resolution of obesity-related comorbidities. Looking forward, subsequent analysis should attempt to incorporate national level data with 3–5 year follow-up to assess both a larger population base and further evaluate the durability of surgical weight loss following the LSG.
Conclusion
LSG is a safe and effective tool for morbid obesity with clinical and serological improvements for veterans who are unable to lose weight with medical management alone.
Footnotes
Acknowledgment
Adherence to Quality Reporting STROBE Checklist: The authors implicitly followed the guidelines while compiling this analysis.
Disclosure Statement
No competing financial interests exist.