
Abstract
Abstract
Objective:
With the improvement of endoscopic diagnosis, the discovery rate of the synchronous multiple primary early cancers in esophagus and stomach is gradually increased, while the traditional surgery bringing serious damages. Endoscopic submucosal dissection (ESD) has become the first treatment option of early cancer in the digestive tract partly. This study intends to explore the feasibility, safety, and effectiveness of ESD in the treatment of the synchronous multiple early gastric cancer or precancerous lesions in the esophagus and stomach.
Methods:
From January 2008 to December 2016, data of 12 patients with early esophageal cancer and early gastric cancer treated by ESD in the Endoscopy Center of Zhongshan Hospital, Fudan University were reviewed. We analyzed the patient's history, the size of esophageal and gastric lesions, pathological results, the results of complete or curative resection, and so on.
Results:
Among the 12 patients described in this study, all were diagnosed with synchronous multiple primary early cancers in the esophagus and stomach. Lesions were removed by ESD in 10 cases at the same time and were removed by stage in 2 cases. The complete resection rate was 100% (24/24), and the curative resection rate was 100% (24/24). Postoperative esophageal stricture occurred in 2 cases, which improved after dilation. Median follow-up time was 30 (8–115) months, when 9 patients survived and 3 patients died. However, the cause of death was not associated with treatment of this disease.
Conclusion:
ESD is a minimally invasive endoscopic surgery, which can be used as a method of treating synchronous multiple primary early cancers in the esophagus and stomach.
Introduction
S
With the development and popularization of endoscopic treatment technology, endoscopic submucosal dissection (ESD) has become widely accepted as a less invasive treatment for part of early cancer or precancerous lesions of the digestive tract.6–7 However, there are few reports about the safety and efficacy of ESD for synchronous esophageal and gastric cancers. Therefore, we retrospectively analyzed the patient data of the registry of our institution and summarized the experience in the treatment of synchronous primary esophageal squamous and gastric cancer or precancerous lesions.
Patients and Methods
Patient information
We retrospectively analyzed data of all the patients who underwent endoscopic treatment at the Zhongshan Hospital Fudan University between January 1, 2008 and December 12, 2013. Among this analysis, synchronous esophageal and gastric early cancer was found in 12 patients and standards proposed by Warren and Gates were satisfied 8 :(1) all cancers should be malignant by histology; (2) each cancer has to be geographically separate and distinct with presence of intervening normal-appearing mucosa; (3) metastatic cancer should be differentiated from multiple primary cancers and ruled out. 3 Synchronous multiple primary cancers are defined as those cancers which are diagnosed within 6 months of each other. 9 Twelve patients all underwent endoscopic examination showing mucosal lesions, and biopsies revealed a primary esophageal SCC and primary gastric adenocarcinoma, and chest, abdomen, and pelvic CT suggested no lymph node enlargement or distant metastasis. Twelve patients with 24 lesions were consistent with endoscopic indications. 10
In this study, we comprehensively analyzed factors, including patient's history, the size of esophageal and gastric lesions, the pathological results, complete or curative resection, intraoperative and postoperative complications and perioperative treatment, and the necessity for additional surgery, radiotherapy, chemotherapy, and so on. Informed consent was obtained from all subjects before the start of treatment.
Endoscopic equipment and technique
All endoscopic surgery procedures were performed by experienced endoscopists (P.H.Z., M.D.X., and Y.S.Z.). Standard single accessory-channel endoscopes (GIF-H260; Olympus, Japan and AQ100, Aohua, China) were used during the procedures. A short, transparent cap (ND-201-11802; Olympus, Japan) was attached to the tip of the gastroscope to provide a constant endoscopic view and to apply tension to the connective tissues during dissection. An insulated-tip (IT) knife (KD-611 L; Olympus, Japan), a hook knife (KD-620LR; Olympus, Japan), and/or HybridKnife (ERBE, Tuebingen, Germany) were used during ESD. The ERBE Hybridknife system (ERBE, Germany) was used as a high-frequency generator.
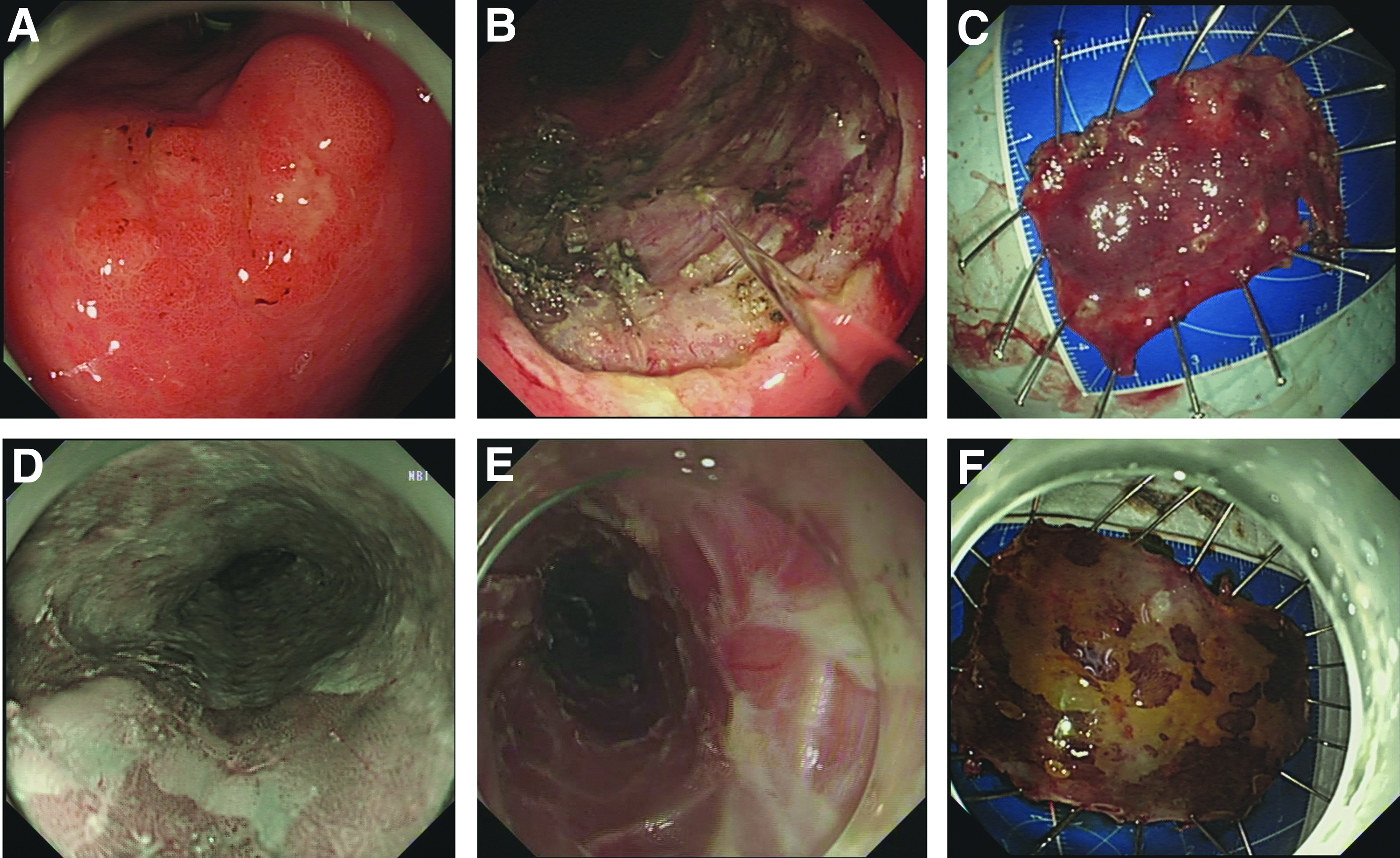
In 12 patients, a total of 24 upper gastrointestinal mucosal lesions were all treated with ESD. The procedure was as follows (Fig. 1): (1) Identification of lesion: marker dots are made ∼5 mm away from the lesion using argon plasma coagulation or an electrosurgical knife. (2) Submucosal Injection: Using a 23-gauge disposable needle (NM-4 L-1; Olympus, Tokyo, Japan), several milliliters of submucosal injection solution are injected around the lesion to lift it off the muscularis propria layer. (3) Circumferential resection: Circumferential mucosal incision of the lesion is performed with an electrosurgical knife outside the markings. (4) Submucosal dissection: The submucosal connective tissue immediately beneath the lesion was dissected from the muscularis propria with an electrosurgical knife. Submucosal injection was repeated as needed, and further dissection was performed to ensure a clear resection layer. Finally, the lesion was removed completely. (5) Hemostasis: Endoscopic hemostasis was performed with hemoclips or hemostatic forceps whenever bleeding or an exposed vessel was observed. (6) Specimen treatment: ESD specimens were stretched, pinned to a polystyrene plate, and fixed in formalin for the pathological examination to assess both lateral and vertical margins.7,11,6
ESD for the synchronous multiple primary early cancers in the esophagus and stomach
Postoperative treatment and follow-up
The day after ESD, fasting and rehydration were applied, and proton pump inhibitors 7 and antibiotics were used as routine. The drainage and drainage fluid color of gastrointestinal decompression, as well as chest pain, abdominal pain, and changes in abdominal signs were paid attention to. If there were no gastrointestinal bleeding or emphysema for 3 days after ESD, the gastric tube could be removed and patients could have a liquid diet. If there were hematemesis, melena, and other symptoms of delayed bleeding, timely endoscopic examination was necessary. Follow-up endoscopies were performed after 3, 6, and 12 months, and annually thereafter. 11 Patients who were not followed up on time, would be followed up once a year on telephone (the last telephone follow-up was on June 30, 2017). Postoperative esophageal stricture would be treated by EBD and local recurrence would be treated by endoscopic treatment or timely surgery.
Definitions and statistical analysis
Pathologic size of lesions was based on the longest diameter of the lesion in the endoscopic resected specimen. R0 resection was defined as en bloc resection with negative horizontal and vertical margins. The margins with electrosurgical or mechanical damage were classified as incomplete resections.7,6 Intraoperative bleeding is defined as the hemostasis needed to suspend surgery and replace with the hot biopsy forceps or other instrument, or the treatment for bleeding is relatively difficult and long. The bleeding that can be treated by simple electrocoagulation was not included. Esophageal stricture was defined as when the endoscope could not be passed through the treatment site; when the patient presented with a chief complaint of dysphagia to semisolid foods, and when endoscopic balloon dilatation was necessary. 12 Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) software (ver. 16.0; SPSS, Inc., Chicago, IL). The measurement data expressed (mean ± standard deviation) were statistically analyzed with t test and numeration data were statistically analyzed with χ2 test, respectively. For all analyses, a P value <0.05% was considered to be significant.
Results
Among the 12 patients described in this study, all were diagnosed with synchronous multiple primary early cancers in the esophagus and stomach, with a mean age of 67 ± 10.6 years. There were 9 male and 3 female cases. The mean size of the esophageal lesion was 2.2 ± 1.1 cm. The esophagus is divided into upper, middle, and lower sections by two points, distance from the incisors 23 cm and distance from the incisors 32 cm. The lesions were detected in the upper esophagus in 3 cases, in the middle esophagus in 8 cases, and 1 in the lower esophagus. The mean size of the gastric lesion was 2.1 ± 1.3 cm with 5 in the antrum, 2 in the gastric angle, and 5 in the cardia. All these lesions suggested early gastrointestinal cancer or precancerous lesions by preoperative endoscopic biopsy.
Lesions were removed in 10 cases at the same time and were removed by stage in 2 cases. The mean procedure time was (85 ± 17) minutes. Complete resection rate was 100% (24/24) with no intraoperative perforation, no uncontrollable bleeding, or no need of surgical resection. The pathological diagnoses were low-grade intraepithelial dysplasia in 1 esophageal lesion, high-grade intraepithelial dysplasia in 5 esophageal lesions, and the rest were SCC with staging of intraepithelial in 2 esophageal lesions, lamina propria in 1, muscularis mucosa in 1, and SM1 in 2 of the esophageal lesions. Out of the 12 lesions in the stomach, the pathological diagnoses were high-grade intraepithelial dysplasia in 7 lesions, and the rest were early gastric adenocarcinoma with staging of one intraepithelial lesion, 1 lesion in lamina propria, and 3 lesions of the muscularis mucosa. Taking the pathology of both the esophagus and stomach into account, postoperative pathological results showed that there were esophageal precancerous lesions with gastric precancerous lesions in 4 cases, esophageal precancerous lesions with early gastric cancer in 2 cases, early esophageal cancer with gastric precancerous lesions in 3 cases, and early esophageal cancer with early gastric cancer in 3 cases.
All the 24 lesions of 12 patients met the indication of the ESD and curative resection rate was 100%. No additional surgery, further chemotherapy, or radiotherapy was administered to all the patients. Postoperative esophageal stricture occurred in 2 cases 1 month after the ESD, which were improved after dilation. Median follow-up time was 30 (8–115) months, when 9 patients survived and 3 patients died. However, the cause of death was not associated with treatment of this disease. The last telephone follow-up was June 30 and the rest of 9 patients absolutely adhered to the follow-up asymptomatically and with no local recurrence.
Discussion
The occurrence of a primary esophageal SCC and a gastric adenocarcinoma is infrequent, especially when both present in the early stage. Good screening programs and increased cancer survival have led to the detection of synchronous and metachronous tumors at increased rates than before. The diagnosis of the synchronous multiple primary early cancers in the esophagus and stomach mainly relies on upper gastrointestinal endoscopy. Synchronous multiple primary early cancers in the esophagus and stomach were observed more frequently among male patients. The incidence of esophageal and gastric synchronous multiple primary cancers was significantly higher in patients who suffered subtotal gastrectomy due to benign gastric lesions than the patient with no remnant stomach. 3 The main feature of gastric cancer in China is the high incidence of cancer in the cardia, so the detection rate of the synchronous multiple primary early cancers in the esophagus and cardia is relatively higher than others.2,3 The number of cases we have presented in the article is not enough; among 12 patients, 5 cases were in the esophagus and cardia, and no case involved the remnant stomach.
At present, all cases reported about the synchronous multiple primary early cancers in the esophagus and stomach refer to at least one advanced lesion. In such cases, an invasive procedure involving anastomosis between the esophagus and the colon must be performed. However, this procedure is associated with a high incidence of mortality and morbidity. I H 13 reported that 7 patients with synchronous esophageal cancer and gastric epithelial neoplasia were encountered. First, ESD was performed for the gastric epithelial neoplasia. Then, following successful ESD, Ivor Lewis esophagectomy for esophageal cancer was planned 1 to 2 weeks later. Kwon et al. 14 also reported one case in which a 65-year-old man with synchronous carcinomas of the esophagus and stomach underwent esophageal reconstruction using a gastric tube following ESD. Among the 12 patients described in this study, all were diagnosed with synchronous multiple primary early cancers in the esophagus and stomach, so we chose ESD to treat the lesions both in the esophagus and stomach.
Among the 12 patients, in 10 cases the lesions were removed at the same time and in 2 cases, they were removed by stage. Removing the lesions at the same time, the patient only needs to be applied endotracheal intubation anesthesia once, as the operation time will be longer. In addition, the simultaneous resection may increase the probability of complications, such as bleeding, perforation, postoperative stricture, and if complications occur, it will be relatively difficult to treat. Resecting the lesions other than by ESD will increase the number of surgeries, whereas reduce the time of each operation, and the most important, makes the complications of treatment relatively simple. For the early gastrointestinal cancer or precancerous lesions, the resection interval of 1 month usually does not affect the postoperative pathological stage and prognosis of patients. The choice of simultaneous resection or resection by stage should depend on doctor's own experience of endoscopic diagnosis and treatment combined with the lesion size, location, and depth of invasion.
In our study, the lesions in case No. 3 (Table 1) were resected apart. The lesion size of the patient was 5 cm and located at the angular notch. It was estimated that the resection time would be long, the wound would be large, and the possibility of delayed bleeding was high. Therefore, ESD was applied on the lesion in stomach 1 month earlier than the lesion in esophagus. Postoperative esophageal stricture occurred 1 month later, which improved after dilation. At the last follow-up, the patient's feedback was good quality of life with no apparent discomfort.
Simultaneous endoscopic treatment for esophageal and gastric lesions is rarely reported. There are still many issues that need to be discussed, including whether lesions should be removed at the same time or by stage; which lesion should be removed first; if choosing removed by stage, how long the internal time should be, and so on. All the results of the present study will be confirmed by a large sample, multicenter, prospective, randomized study.
In our experience, (1) If both esophageal and gastric lesions are small enough and the operation time is expected to be less than 2 hours, the lesions can be removed at the same time. It is advantageous to remove the gastric tumor endoscopically before resection for esophageal cancer to avoid the friction of the endoscope to the wound. In the process of removing gastric lesions, if the border of the esophageal lesions becomes unclear or bleeding, making resection difficult, resecting by stage will be recommended. If there are any unexpected difficulties making the operation time much longer, resecting by stage will also be recommended. (2) If the operation time for simultaneous resection is more than 2 hours, resecting by stage will be recommended. If the preoperative endoscopy and histopathological results revealed that between the two lesions, one is severer than the other, the severer one will be resected prior. If the degree of lesions is similar, it is recommended to remove the lesion in stomach prior. (3) It usually takes 4 weeks for the surgical wound to be healed, so the interval between two ESD is about 4 weeks in order not to affect the operation and postoperative medication. Basically, the prognosis will not be affected. (4) Based on the specific condition of patients, additional surgery, radiotherapy, chemotherapy should be applied to the patients who does not fulfill the criteria for ESD according to postoperative pathology result.
The key point that synchronous multiple early cancer or precancerous lesions in esophageal and stomach can be removed by ESD is the early detection of cancer. Nowadays, there are many ways to detect early gastrointestinal cancer, such as conventional white light imaging, chromoendoscopy, narrow band imaging magnifying endoscope, and endoscopic ultrasonography etc. With careful endoscopic inspection of the esophagus and stomach, which does not focus too narrowly on only one lesion found initially, we should pay attention to detect more multiple early cancers and will not miss any other lesions.
In conclusion, early screening, correct diagnosis, and appropriate plans of management are crucial to reduce the morbidity and mortality of such patients who bear the burden of not just one, but multiple primary cancers. Simultaneous endoscopic treatment for esophageal and gastric lesions is rarely reported. There are still many issues that need to be discussed; however, ESD is a minimally invasive endoscopic surgery, which can be used as a method of treating synchronous multiple primary early cancers in the esophagus and stomach.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (81502000,W2015JZC12); and grant from the Shanghai Committee of Science and Technology (15ZR1406800,15DZ1940202,16DZ2280900)
Disclosure Statement
No competing financial interests exist.