
Abstract
Abstract
Aim:
The aim of this study was to compare the plastic stents with metal stents for preoperative biliary drainage (PBD) in terms of the rate of endoscopic reintervention and PBD-related pre- and postoperative complications in patients with resectable and borderline resectable periampullary cancer.
Methods:
We conducted a comprehensive search of the PubMed, EMBASE, and the Cochrane Library database to identify relevant available articles from their inception to September 2017. The odds ratio (OR) with 95% confidence interval (CI) was calculated to compare the incidence of endoscopic reintervention and stent-related complications between the plastic and metal stents groups. Also, we used RevMan 5.3 to perform the pooled analyses.
Results:
Four trials (three randomized controlled trials [RCT] and one prospective clinical trial) with 392 patients were included. One hundred seventy-four patients received metal stents for PBD, and 218 patients received plastic stents. The metal stents group had a significant lower rate of endoscopic reintervention (OR = 0.30, 95% CI = 0.13–0.73, P = .008) and preoperative cholangitis (OR = 3.60, 95% CI = 1.62–7.98, P = .002) compared with the plastic stents group. But there was a significantly higher rate of PBD-related pancreatitis (OR = 3.60, 95% CI = 1.62–7.98, P = .002) in the metal stents group.
Conclusions:
The present meta-analysis revealed that metal stents have significantly lower rate of reintervention and cholangitis than plastic stents. But plastic stents have an obvious superiority over metal stents in terms of the incidence of preoperative pancreatitis. More RCTs are required to support this conclusion and provide more detailed information about the complications and treatment. Meanwhile, a uniform standard for the PBD is required in patients with malignant distal biliary obstruction.
Introduction
P
For patients with resectable or borderline resectable MDBO, one of the most common complications is jaundice that can lead to hepatic impairment and cholangitis. Therefore, preoperative biliary drainage (PBD) is always utilized to relieve jaundice and recover the enter-hepatic circulation, then reduce the pre- and postoperative complications of patients.4,5 Although in recent years, several studies have evaluated that PBD should not be used routinely when compared with early surgery,6–8 the PBD procedure is still essential to patients with extreme hyperbilirubinemia, which is associated with profound hepatic impairment. Meanwhile, PBD may be necessary for patients with borderline resectable cancer and undergoing neoadjuvant therapy.1,9
Endoscopic stenting is the most common method for PBD, 1 and there are two types of stents: the plastic and metal stents. Several retrospective studies10–12 and one randomized controlled trial (RCT) 13 that compared the metal and plastic stents for PBD have shown that there were fewer stents failure and stent-related complications in patients with metal stents. However, a recent RCT 14 revealed that the outcomes of patients with plastic stents were similar to those with metal stents, and there were even fewer costs in patients with plastic stents. Meanwhile, all recent trials observed a high morbidity of preoperative pancreatitis in patients with metal stents, which was not well mentioned before.
Due to the above controversial findings, we carried out a meta-analysis to compare the plastic stents with metal stents for PBD in patients with resectable and borderline resectable MDBO, in terms of the rate of PBD-related pre- and postoperative complications.
Methods
Search strategy
We conducted a comprehensive electronic search in the PubMed, the EMBASE, and the Cochrane Library database to identify relevant available articles from their inception to September 2017. The search terms included “stenting”, “stent”, “stents” combined with the terms “plastic”, “plastics” and “metal”, “metals” and “biliary” and “decompression”, “drainage”. We also reviewed the reference lists of included studies and relevant reviews for identifying additional studies.
Inclusion and exclusion criteria
The inclusion criteria were set as follows: (1) studies that focused on metal versus plastic stents for PBD in patients with resectable and borderline resectable periampullary cancer; (2) research in adults; (3) studies presented at least one outcome that related to the rate of pre- or postoperative adverse events. The exclusion criteria were as follows: (1) retrospective studies; (2) studies contained patients undergoing early surgery; (3) patients with unresectable periampullary cancer; (4) the type of the articles is a review or case reports or editorial. Two of the authors scrutinized the titles and abstracts of all identified articles for the first step of selection, and then, we read the full text to further exclude the unqualified studies. If we could not reach a consensus, it would be resolved by consulting with a third author.
Data extraction and quality assessment
The following information was independently extracted by one author and checked carefully by others: first author, publication year, study location, study period, study design, demographics, clinical characteristics before PBD, the type of stents, and interval to surgery after PBD, PBD-related outcomes before and after surgery. The modified Jadad scoring system, an instrument for assessing the quality of RCT, was used for assessing each included trial according to the descriptions of randomization, blinding, and withdrawals in the trials. Each study can be awarded a score from one point to seven points.
Statistical analysis
The meta-analysis was conducted using the RevMan software version 5.3 (The Nordic Cochrane Center, Cochrane Collaboration, Copenhagen, Denmark). The odds ratio (OR) with 95% confidence interval (CI) was calculated to compare the incidence of stent-related complications and reintervention rate between the plastic and metal stents groups. Heterogeneity among the included studies was qualitatively evaluated using a χ2-based Q test. A P value less than .05 showed that there was significant heterogeneity across the studies. The level of heterogeneity between studies was evaluated by I2 statistics. I2 < 30% was considered to be low heterogeneity and a fixed effects model were applied. 30% ≤ I2 ≤ 50% was considered to be moderate heterogeneity, and I2 > 50% represented high heterogeneity. A random effects model was applied when I2 ≥ 30%.
Sensitivity analysis and assessment of risk of bias
Sensitivity analysis was performed by removing one study at a time to assess whether the results could have been markedly affected by the single study. The risk of bias was assessed by a quality checklist recommended by the Cochrane Handbook for Systematic Reviews.
Results
Search results and study characteristics
A total of 613 articles were retrieved by searching electronic databases and manual searching relevant reference lists. After duplicates were differentiated and excluded, 450 articles were left. Then, we excluded studies that were irrelevant to the topic based on the title and abstract, and 97 articles were left. Of those, 93 articles were excluded (36 articles were PBD versus early surgery, 24 articles with unresectable cancer, 18 retrospective studies, 10 review articles, 2 duplicate reports, and 3 articles without interesting outcome), and 4 trials (3 RCT and 1 prospective clinical trial)13–16 were selected for this meta-analysis. Study selection process was shown in Figure 1. Characteristics of the studies and demographics and clinical characteristics before PBD are presented in Table 1.
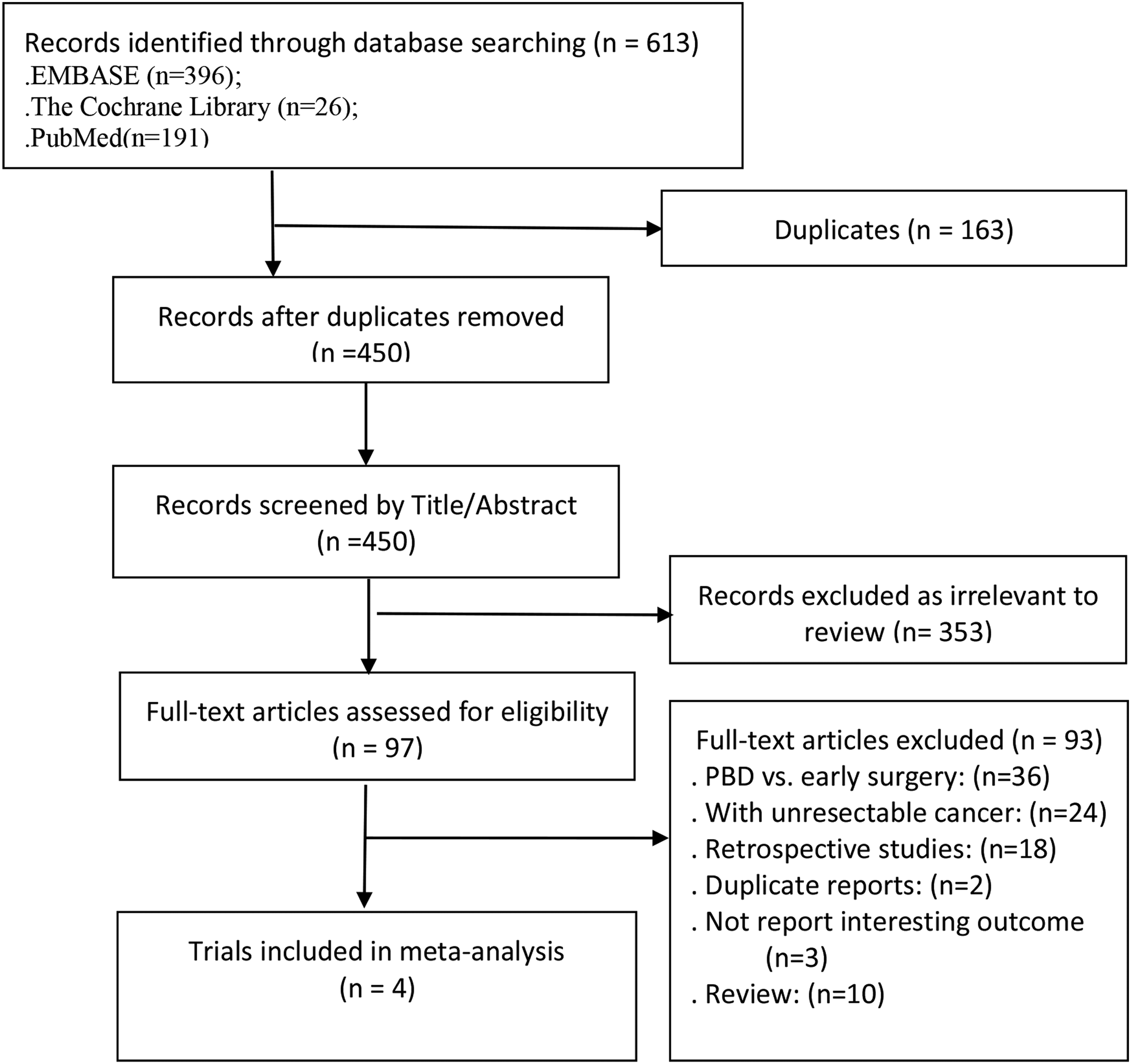
Study selection process.
BMI, body mass index; FCSEMS, fully covered self-expanding metal stents; NR, not reported; RCT, randomized controlled trial.
Four trials included 392 patients, of those, 174 patients received metal stents and 218 patients received plastic stents for PBD. In addition, trials were performed in four different countries (Spain, Netherlands, South Korea, and Sweden). The sample sizes ranged from 63 to 151. All plastic stents were 10F of the diameter, and length ranged from 5 to 9 cm. All metal stents were fully covered self-expanding metal stents (FCSEMS), In Song's trail, 14 stents of 8 or 10 mm in diameter were used, while in all other trials only stents with a diameter of 10 mm were used. Meanwhile, the length of metal stents ranged from 4 to 8 cm (most commonly 6 cm in Olsson's 16 trail, 4 to 7 cm in Song's 14 trail, and most 6 cm in Tol's 15 trail), and authors just stated that it depended on the stricture. For drainage time, three trials showed little difference (average 36.4 days to 42 days), but Song et al. 14 reported a much shorter drainage time (average 14.2 days in the plastic group and 12.3 days in the metal group).
Endoscopic reintervention
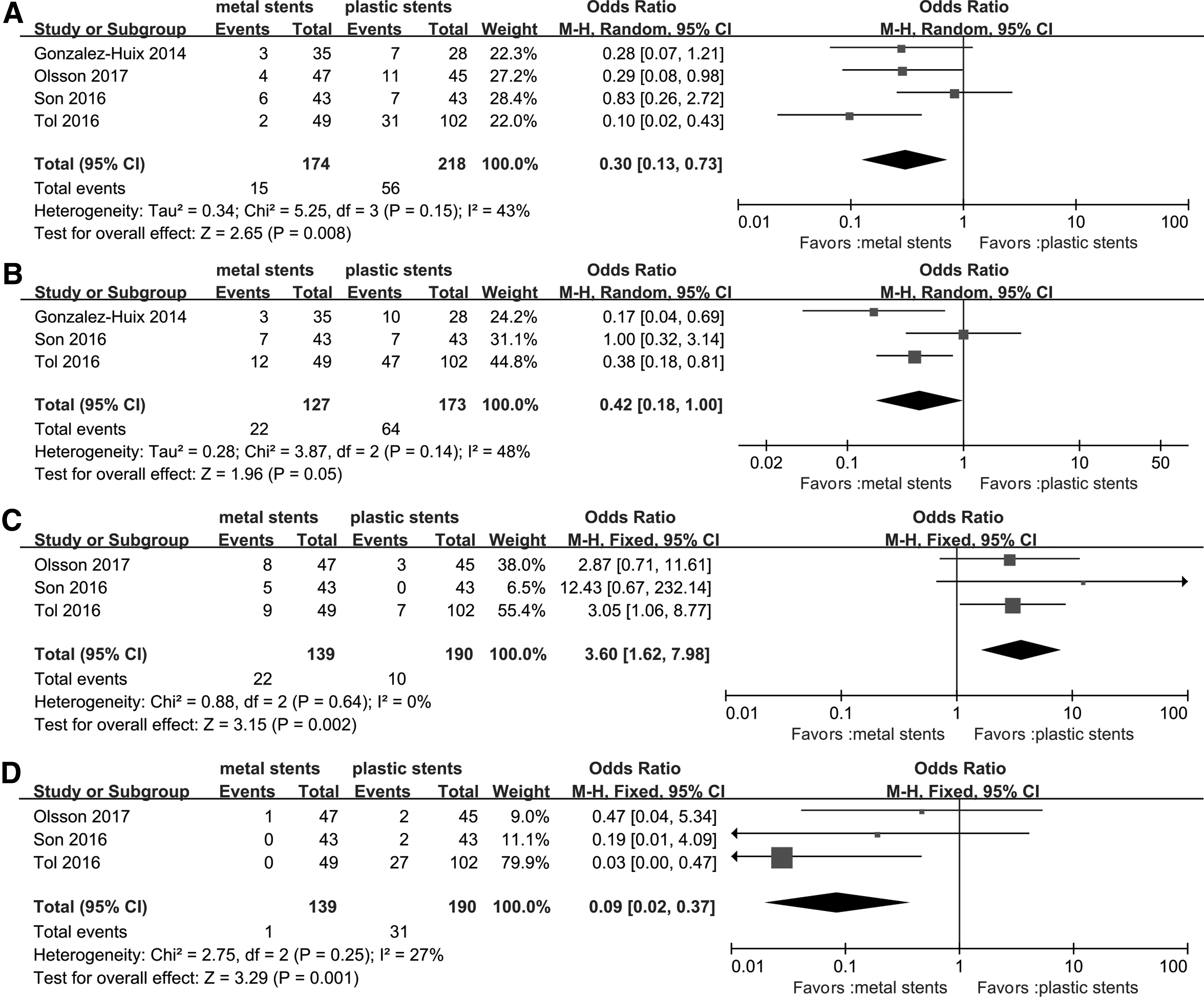
All studies,13–16 containing 174 cases in the metal stents group and 218 cases in the plastic group, provided data regarding the rate of reintervention before surgery. It means stent failure and stent changing. Moderate heterogeneity (I2 = 43%, P = .15) was found, therefore, a random effects model was used to pool the OR, and the rate of reintervention was significantly lower in the metal stents group than in the plastic stents group (OR = 0.30, 95% CI = 0.13–0.73, P = .008) (Table 2, Fig. 2A).
Forest plot of
NR, not reported; PBD, preoperative biliary drainage.
Overall PBD-related preoperative complications
Three studies,13–15 including 174 cases in the metal stents group and 218 cases in the plastic stents group, provided data for this outcome. Moderate heterogeneity (I2 = 48%, P = .14) was found, and the pooled data demonstrated that the overall PBD-related preoperative complications were lower in the metal stents group than the plastic stents group, but the results were not statistically significant (OR = 0.42, 95% CI = 0.18–1.00, P = .05) (Table 2, Fig. 2B).
Preoperative pancreatitis
Three studies14–16 provided data for this outcome, and all the three studies observed a great difference between the two groups, and no heterogeneity (I2 = 0%, P = .64) was found. The pooled data demonstrated that the rate of preoperative pancreatitis was significantly higher in the metal stents group (22/139, 15.8%) than plastic stents group (10/190, 5.3%) (OR = 3.60, 95% CI = 1.62–7.98, P = .002) (Table 2, Fig. 2C).
Preoperative cholangitis
Three studies14–16 provided data for this outcome, and all observed a lower rate of preoperative cholangitis in metal groups, and low heterogeneity (I2 = 27%, P = .25) was found. Also, the pooled data demonstrated that the rate of preoperative cholangitis was significantly lower in the metal group (1/139, 0.7%) than in the plastic group (31/190, 16.3%) (OR = 0.09, 95% CI = 0.02–0.37, P = .001) (Table 2, Fig. 2D).
Patients undergoing surgery and undergoing curative resection
The rate of patients undergoing surgery in those four studies13–16 was different, and high heterogeneity (I2 = 73%, P = .01) was found. The pooled data demonstrated that the results were not statistically significant (OR = 0.66, 95% CI = 0.27–1.58, P = .35) (Table 2, Fig. 3A).

Forest plot of
As for the rate of patients undergoing curative resection, three studies provided data.14–16 Moderate heterogeneity (I2 = 48%, P = .14) was found. The pooled data demonstrated that the results were not statistically significant in the rate of patients undergoing curative resection as well (OR = 0.56, 95% CI = 0.21–1.49, P = .25) (Table 2, Fig. 3B).
Overall postoperative complications
Three studies14–16 provided data for this outcome, and no heterogeneity (I2 = 0%, P = .69) was found, so we used a fixed-effect model to pool the OR. 42.7% of the patients in metal groups (50/117) versus 52.3% in plastic groups (88/168) suffered from postoperative complications. But the pooled data demonstrated that the result was not statistically significant (OR = 0.65, 95% CI = 0.40–1.05, P = .08) (Table 2, Fig. 3C).
Postoperative infection
The definition of infection included intraperitoneal infection and wound infection. Three studies14–16 provided data, and no heterogeneity (I2 = 0%, P = .62) was found. The rate of postoperative infection was 19.7% in metal group (23/117) versus 13.1% in plastic group (22/168), and there was no statistical difference (OR = 1.69, 95% CI = 0.87–3.26, P = .12) (Table 2, Fig. 3D).
Postoperative anastomotic leakage
The definition of anastomotic leakage included both pancreatic and biliary anastomotic leakage. Three studies14–16 provided data for this outcome, and no heterogeneity (I2 = 0%, P = .49) was found. The rate of postoperative anastomotic leakage was 5.1% in metal stents groups (6/117) versus 9.5% in plastic stents groups (16/168), but the result was not statistically significant (OR = 0.51, 95% CI = 0.19–1.35, P = .17) (Table 2, Fig. 3E).
Postoperative delayed gastric emptying
Three studies14–16 provided data for this outcome, and no heterogeneity (I2 = 0%, P = .92) was found. The rate of postoperative anastomotic leakage was 12.8% in metal group (15/117) versus 17.6% in plastic group (29/168), but the result was not statistically significant (OR = 0.70, 95% CI = 0.35–1.40, P = .32) (Table 2, Fig. 3F).
Sensitivity analysis and assessment of risk of bias
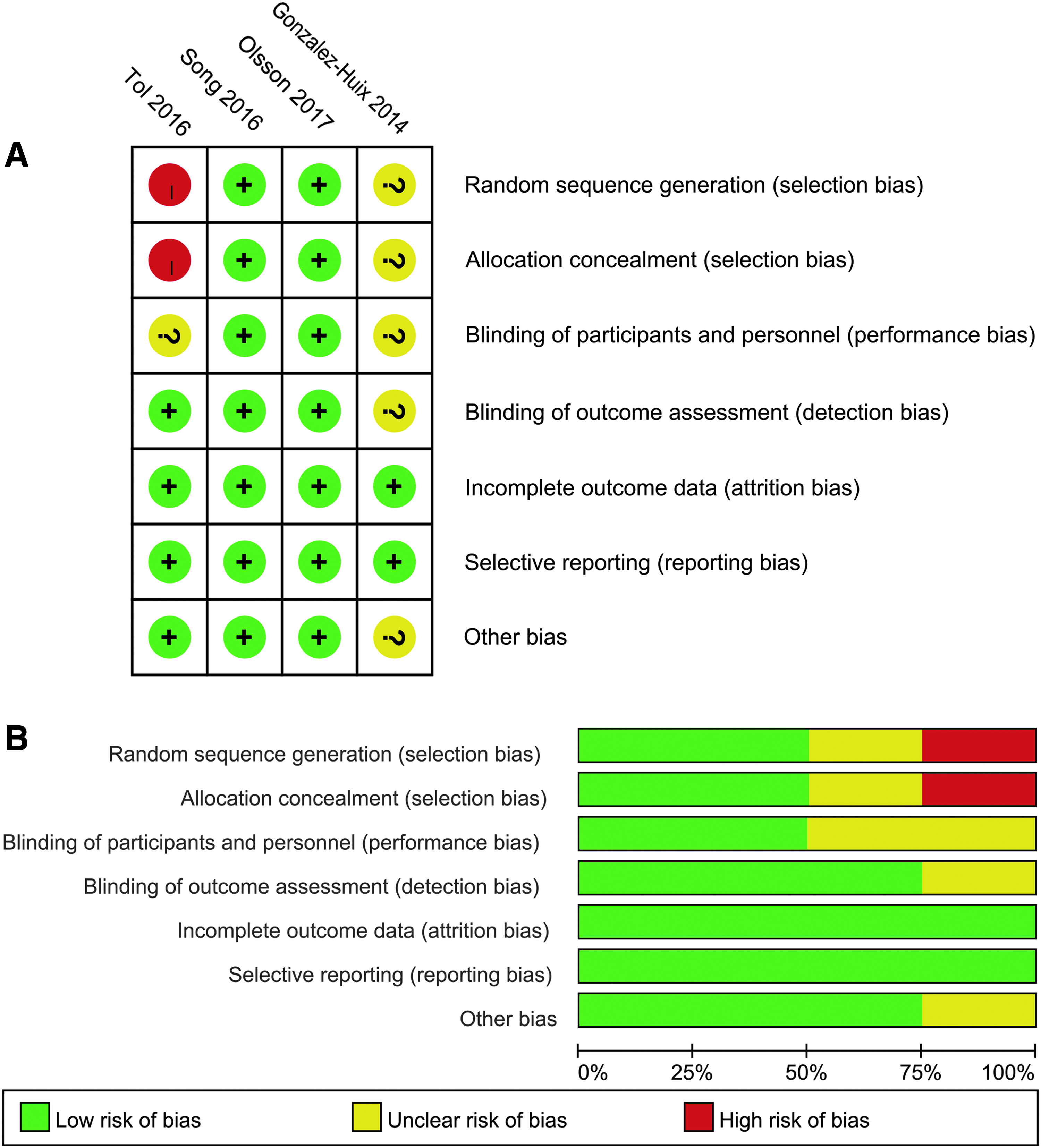
We performed a sensitivity analysis by removing one study at a time to assess whether the results could have been markedly affected by a single study in pooled data with moderate and high heterogeneity. Sensitivity analysis suggested that the results in this meta-analysis were relatively stable except for the rate of overall preoperative complications and the rate of patients undergoing curative resection. When removed Song's trial, the I2 = 0 and the results were statistically significant. The rate of overall preoperative complications was significantly higher in plastic groups (OR = 0.32, 95% CI = 0.16–0.62, P = .0007) (Fig. 4A), and the rate of patients undergoing curative resection was significantly higher in metal groups (OR = 0.34, 95% CI = 0.14–0.85, P = .02) (Fig. 4B). Meanwhile, high risk of bias was considered in two studies, and the risk of bias summary and risk of bias graph are shown in Figure 5.

Forest plot of
Forest plot of
Discussion
Although the necessity of PBD in patients with potentially curable malignant biliary obstruction (MBO) is controversial, 17 many trials have shown positive results to support PBD.17–20 Furthermore, patients with hyperbilirubinemia and profound hepatic impairment may not be able to get further treatments before PBD. Endoscopic stenting is the most common method for PBD, but which type of stent is more appropriate is still on debate. The present meta-analysis revealed that the rate of reintervention (OR = 0.30, 95% CI = 0.13–0.73, P = .008) and preoperative cholangitis (OR = 0.09, 95% CI = 0.02–0.37, P = .001) were both significantly lower in the metal group than the plastic group. But the rate of preoperative pancreatitis was significantly higher in the metal group (OR = 3.60, 95% CI = 1.62–7.98, P = .002). And the results about overall preoperative complications and postoperative outcomes between the two groups were not statistically significant.
Metal stents were evaluated to be superior to plastic stents for palliative drainage in patients with unresectable MBO. With a longer patency time, metal stents can reduce the stent-related complications and the frequency of replacement compared with plastic stents.21,22 For PBD, a period of 4 to 6 weeks, which was much shorter than the essential palliative drainage time, have been suggested to recover the normal major synthetic of the liver and the mucosal intestinal barrier functions. 23 Also, a meta-analysis showed that a drainage time less than 4 weeks increased overall morbidity from 7% to 23% compared with a drainage time more than 4 weeks on patients with obstructive jaundice. 17 Tol et al. 15 compared the relationship between drainage time and the incidence of preoperative complications in the metal and plastic stents groups. And there was no difference in terms of the rate of preoperative complications between the two groups in the first 2 weeks of PBD. However, when the drainage time exceeded 2 weeks, the preoperative complications rate was significantly higher in the plastic stents group. As for this reason, the difference in drainage time may explain the result of sensitivity analysis of overall preoperative complications. Song et al. 14 reported that the drainage time in their trial was much less than others. But this conclusion still needs to be further discussed, and more clinical trials are required.
Pancreatitis is a common complication of ERCP-related procedures, sphincterotomy and biliary stenting can increase the rate of pancreatitis. 24 For PBD, pancreatitis results from the combined effects of ERCP-related and stent compression on the pancreatic duct.25–27 FCSEMS have a wider diameter than plastic stents, and there may be more severe pressure on the pancreatic duct, therefore, the incidence of pancreatitis is higher in metal stents group. But the severity of pancreatitis in patients are mostly mild to moderate in both metal and plastic groups, and very few patients suffer from severe or hemorrhagic pancreatitis.8,28 Hashimoto et al. 29 did a research of the risk factors for pancreatitis in PBD, and they found that a normal bilirubin level is at high risk of pancreatitis. But for patients with MDBO, most of them are old and the main pancreatic duct already been obstructed by tumor. Meanwhile, biliary obstruction led to higher bilirubin levels in these patients. Therefore, some investigators believe that pancreatitis should not be a major concern in PBD-related complications in consideration of the effectivity of conservative treatment. 15 But attention should also be required to avoid pancreatitis and further deterioration of pancreatitis in view of the high incidence of pancreatitis in metal stent group. Furthermore, the cost of hospitalization is also an important factor that should be considered.
Some clinicians have a concern that using stents for PBD might cause local tissue inflammation, which may lead to the technical difficulties during surgery. 30 Siddiqui et al. 28 performed a large multicenter, retrospective study of PBD with metal stents, and in their study, technical success and clinical success were achieved in all patients. And several other studies drove the similar conclusion that metal stents did not affect the surgery.11,13 In addition, Olsson et al. 16 did pathological examination by using the incisal margin tissue, and no severe histiocytosis and cholangitis have been found.
Finally, there were several limitations in the present meta-analysis. First, only four studies met our inclusion criteria, and therefore, the sample size was not large enough. Second, the criteria for PBD and the standard for reintervention in the included trials were different, which may lead to bias in this meta-analysis. Third, all trials did not provide detailed information about the length of the metal stents using in their studies, we cannot comment on whether the difference in the length of the metal stents is an effect factor on the results. Fourth, the drainage time was different among the four involved studies and that might lead to bias in the results of the present meta-analysis, but further subgroup analysis cannot be implemented to prove our conjecture because of the lack of sample size.
Conclusion
For patients with resectable or borderline resectable periampullary cancer and MDBO, the present meta-analysis demonstrated that there were lower rates of reintervention and PBD-related cholangitis in patients with metal stents than in patients with plastic stents. However, plastic stents have an obvious superiority over metal stents in terms of the incidence of PBD-related preoperative pancreatitis. Also, there were no significant differences between the two types of stents in terms of the incidence of postoperative complications. More RCTs are required to support this conclusion and provide more detailed information about the complications and treatment. Meanwhile, a uniform standard for the PBD is required in patients with MDBO.
Footnotes
Disclosure Statement
No competing financial interests exist.